

Abstract
Pelvic floor muscle training (PFMT) reduces the symptoms in women with pelvic floor dysfunction (PFD); however, the optimal initial timing for secondary prevention of PFD by PFMT is not clear. To identify the optimal timing in Asian primiparas with vaginal delivery, bladder neck descent (BND), levator hiatus areas, and levator hiatus distensibility and contractility were assessed in 26 nulliparous women at 36 weeks of gestation and at 2, 4, 6, and 12 weeks postpartum. We found that BND increased significantly from 2 weeks onwards until 6 weeks postpartum (p = 0.004); the levator hiatus area at rest and contraction both showed the largest value at 2 weeks postpartum (p = 0.005 and p < 0.005 respectively), followed by a continuous decrease; the hiatus area during Valsalva manoeuvre, and the levator hiatus distensibility and contractility showed the lowest value at 2 weeks postpartum, followed by a continuous increase; the changes in BND showed no correlation with the changes in distensibility or hiatus area during Valsalva manoeuvre (p = 0.073 and 0.590 respectively). In Asian primiparas with vaginal delivery, the recovery of levator hiatus and bladder neck mobility begins at 2 and 6 weeks, respectively. This information could be useful in defining the best time to begin PFMT for secondary prevention of postpartum PFD in Asian primiparous women.
What is already known on this subject? Pelvic floor muscle training (PFMT) helps to reduce symptoms of pelvic floor dysfunction (PFD), however, there are no clear time strategies for the secondary prevention of PFD by PFMT in Asian primiparas with vaginal delivery.
What do the results of this study add? This study was the first longitudinal study in Asian primipara to investigate the natural regeneration of pelvic floor functions in the early postpartum period by intensively monitoring the bladder neck mobility and levator hiatus dimensions at multiple time points. We found that bladder neck descent (BND) increased significantly from 2 weeks onwards until 6 weeks postpartum; the levator hiatus area at rest and contraction both showed the largest value at 2 weeks postpartum, followed by a continuous decrease; the hiatus area during Valsalva manoeuvre, and the levator hiatus distensibility and contractility showed the lowest value at 2 weeks postpartum, followed by a continuous increase; the changes in BND showed no correlation with the changes in distensibility or hiatus area during Valsalva manoeuvre.
What are the implications of these findings for clinical practice and/or further research? Our study suggested that in Asian primipara, the recovery of bladder neck mobility after vaginal delivery begins at 6 weeks postpartum, while the levator hiatus muscle begins to recover within the first 2 weeks postpartum. Therefore, it could be useful in deciding the best time to start PFMT for secondary prevention of postpartum PFD in Asian primiparous women.
IMPACT STATEMENT
Introduction
The female pelvic floor is composed of pelvic organs with multiple layers of supporting tissues such as the levator ani muscle and fascia. These supporting tissues act as a "hammock" holding the pelvic organs including the bladder, uterus, and rectum. Disorder of these supporting tissues results in pelvic floor dysfunction (PFD). The most common symptoms of PFD include pelvic organ prolapse and stress urinary incontinence. Vaginal delivery is the primary risk factor for PFD (Dietz Citation2006, Blomquist et al. Citation2018). Both the levator hiatus dimension (a parameter associated with pelvic organs prolapse (Shek et al. Citation2012, Staer-Jensen et al. Citation2013, van Veelen et al. Citation2014b) and bladder neck descent (BND) (a parameter related to stress urinary incontinence (Staer-Jensen et al. Citation2015, van Veelen et al. Citation2014a, de Araujo et al. Citation2018, Reimers et al. Citation2019) are increased postpartum.
Pelvic floor muscle training helps to reduce prolapse and overactive bladder symptoms in women with PFD (Hagen et al. Citation2017, Toprak Celenay et al. Citation2022). However, the optimal initial timing of the intervention for secondary prevention of PFD in puerpera is not clear. Waarsenburg et al found that the structure of the puborectalis muscle largely recovered during the first three weeks postpartum, while the stretch of the puborectalis muscle consistently increased 24 weeks after the first vaginal delivery (Van de Waarsenburg et al. Citation2018). These findings suggested that the best window to initiate secondary prevention of PFD may be within the first 3 weeks postpartum. However, the early regeneration of bladder neck activity after first vaginal delivery is not well characterised; in addition, whether the changes of BND are associated with the changes in levator hiatus dimensions is not clear.
Race is also considered as a risk factor for PFD (Bump and Norton Citation1998). Previous studies have shown inter-racial differences in the dimensions of pelvic floor and the risk of pelvic floor prolapse (Graham and Mallett Citation2001, Zarate-Kalfopulos et al. Citation2012, Abdool et al. Citation2017, Cheung et al. Citation2019). However, to the best of our knowledge, no studies have investigated the early postpartum changes in BND and levator hiatus dimensions in Asian women. Therefore, we assessed the dynamic postpartum changes in pelvic floor structure and function in Asian primipara based on 4D ultrasound imaging.
Materials and methods
The procedures followed were in accordance with the ethical standards of Chengdu Women’s and Children’s Central Hospital and the Helsinki Declaration of 1975, as revised in 2000. The study is registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2000033979) and approved by the Ethics Committee of the Chengdu Women’s and Children’s Central Hospital.
Primiparas in 30–35 weeks of gestation were enrolled from January 2019 to December 2021. Exclusion criteria were multiple pregnancy, signs of threatened abortion, history of urogenital surgery, connective tissue disease, history of neurological disease and lumbosacral trauma, and suspected PDF diagnosis based on Pelvic Organ Prolapse Quantification (POP-Q) examination (Bump et al. Citation1996). Written informed consent was obtained from all subjects prior to their enrolment. All subjects completed clinical questionnaires and signed the consent forms after enrolment. The survey information included: age, height, weight, parity, gestational age, presence of PFD symptoms during pregnancy and postpartum by using Pelvic Organ Prolapse Symptom Score (POP-SS) (Hagen et al. Citation2009), and results of gynecological clinical examination.
The pelvic floor ultrasound examination was performed at 36 weeks of gestation and at 2, 4, 6, and 12 weeks postpartum respectively by two experienced sonographers, who also analysed the ultrasonogram by using GE 4D View offline analysis software. A GE Voluson E8 ultrasound equipment with 4–8 MHz curved array four-dimensional ultrasound transducer was used; the two-dimensional emission angle of the probe and the 4D scanning angle was adjusted to the maximum (70° and 85°, respectively). The volume probe was coated with a sterile ultrasound gel and covered with a disposable probe cover. Participants were instructed to empty the bladder before examination and to maintain a supine position during an ultrasound. The probe was placed on the perineum in the sagittal plane to clearly show the pubic symphysis, urethra, bladder neck, posterior bladder wall, vagina, rectum, and anal canal. Data sets were obtained at rest, contraction, and maximum Valsalva manoeuvre; each action was performed at least three times. The procedures for 2D and 4D perineal pelvic floor ultrasound examinations are described elsewhere (2019). The levator hiatus area was measured as the area bordered by the pubovisceral muscle, pubic symphysis, and the inferior pubic ramus. The BND was calculated by subtracting the bladder neck-symphysis distance at rest from the bladder neck-symphysis distance during Valsalva manoeuvre; the distensibility was calculated by subtracting the hiatal area at rest from the hiatal area during Valsalva manoeuvre; the contractility was calculated by subtracting the hiatal area at contraction from the hiatal area at rest, as previously reported (van Veelen et al. Citation2014b, Dietz et al. Citation2016, Van de Waarsenburg et al. Citation2018).
Statistical analysis
SPSS version 24.0 statistical software (IBM, Armonk, NY, USA) was used for data analysis. Normality of distribution of variables was assessed using the Shapiro-Wilk normality test or KS normality test. One-way Repeated Measures ANOVA followed by Tukey’s Honestly Significant Difference analysis (Tukey’s HSD) was used to assess whether the values at various time-points were significantly different. Correlation analysis was performed using the Mantel-Haenszel Chi-square test. P values < 0.05 were considered indicative of statistical significance. Figures were created using GraphPad Prism 7.00 (GraphPad Software Inc.).
Results
Forty nulliparous women (age >18 years) with a singleton pregnancy were enrolled; of these, 10 were excluded because of caesarean section; 3 were ruled out because of inability to perform effective Valsalva manoeuvre postpartum; and one was excluded because of perianal abscess that required surgery. Finally, 26 subjects completed the entire schedule of pelvic floor ultrasound examinations at 36 weeks of gestation, and at 2, 4, 6, and 12 weeks postpartum. The maternal and obstetric characteristics, including the occurrences of episiotomy, perineal tear and obstetric anal sphincter injuries, are summarised in . There is no association between patient’s demographics and ultrasonogram parameters.
Table 1. Maternal characteristics and obstetrical characteristics.
Bladder neck descent
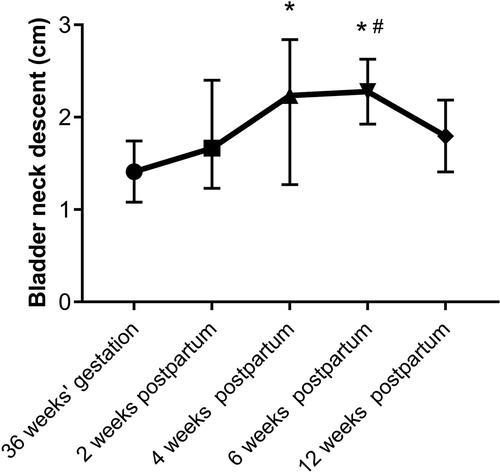
shows the median ± 95% confidence intervals (CI) of BND at 36 weeks of gestation, and at 2, 4, 6, and 12 weeks postpartum. The changes in BND over time were significant (p < 0.005). BND was smallest at 36 weeks of gestation, and continued to increase postpartum until 6 weeks. The highest value of BND was observed at 6 weeks postpartum and it was significantly higher than that at 36 weeks of gestation (p = 0.004). The value of BND at 12 weeks postpartum was significantly lower than the value at 6 weeks postpartum (p = 0.005). Notably, the BND values were less than 2.5 cm in all participations assessed at 5-time points. The detailed data of BND is provided in supplemental Table S1.
Figure 1. Bladder neck descent at 36 weeks of gestation, and at 2, 4, 6, and 12 weeks postpartum. *indicates significant difference from 36 weeks of gestation. #indicates significant difference from 12 weeks postpartum. Data presented as median with 95% confidence intervals (CIs); between-group differences assessed by One-way Repeated Measures ANOVA followed by Tukey’s Honestly Significant Difference analysis; p < 0.05 was considered statistically significant.
Levator hiatus area
shows the median ± 95% CI of the levator hiatus area at 36 weeks of gestation, and at 2, 4, 6, and 12 weeks postpartum, at rest (), contraction () and during Valsalva manoeuvre (), respectively.
Figure 2. Levator hiatus area at rest (2 A), contraction (2B) and during Valsalva manoeuvre (2 C) at 36 weeks of gestation, and at 2, 4, 6, and 12 weeks postpartum. Data presented as median with 95% confidence interval (CI); between-group differences assessed by One-way Repeated Measures ANOVA followed by Tukey’s Honestly Significant Difference analysis; p < 0.05 was considered statistically significant, # indicates significant difference from 12 weeks postpartum, § indicates significant difference from 2 weeks postpartum.
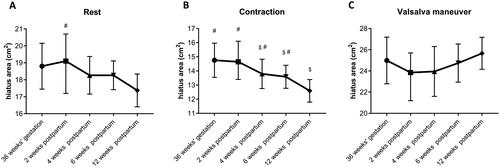
At rest, the value of the hiatus area was highest at 2 weeks postpartum and showed a decreasing trend thereafter. The value at 12 weeks postpartum was significantly lower than the value at 2 weeks postpartum (p = 0.005), although the overall changes over time were not significant (p = 0.106).
During contraction manoeuvre, the changes in the hiatus area over time were significant (p = 0.001). The highest value of hiatus area postpartum also appeared at 2 weeks after delivery, followed by a gradual decrease. The values of hiatus area at 4, 6, and 12 weeks postpartum, respectively, were significantly lower than that at 2 weeks postpartum (p = 0.013, 0.009, and < 0.005 respectively).
During Valsalva manoeuvre, the changes in the hiatus area over time were also significant (p = 0.041). The hiatus area was smallest at 4 weeks postpartum and showed an increasing trend thereafter. The hiatus area at 12 weeks postpartum was higher than that at 36 weeks of gestation, although the difference was not significant. The detailed data of levator hiatus area at different manoeuvres are provided in supplemental Table S1.
Distensibility and contractility of levator hiatus
shows the median ± 95% CI of distensibility (rest-to-Valsalva hiatal area difference). The distensibility was lowest at 2 weeks postpartum and showed a continuous increase thereafter. The highest value of distensibility was observed at 12 weeks postpartum, which was greater than the one at 36 weeks of gestation, but the difference was not significant. However, there was a significant difference between the value at 12 weeks postpartum with those at 2 and 4 weeks postpartum (p = 0.006 and 0.026, respectively).
Figure 3. Levator hiatus distensibility (3A) and contractility (3B) at 36 weeks gestation and at 2, 4, 6, and 12 weeks postpartum. Data presented as median with 95% confidence interval (CI); between-group differences assessed by One-way Repeated Measures ANOVA followed by Tukey’s Honestly Significant Difference analysis; p < 0.05 was considered statistically significant. # indicates significant difference from 12 weeks postpartum.
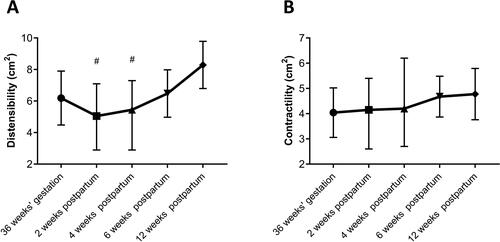
shows the median ± 95% CI of contractility (rest-to-contraction hiatal area difference). The contractility showed a continuously increasing trend after delivery; however, the changes over time was not significant (p = 0.386). The detailed data on distensibility and contractility are provided in supplemental Table S1.
Correlation between BND and distensibility
To determine if the changes of BND were associated with the hiatus area during Valsalva manoeuvre or distensibility, we conducted a correlation analysis of the changing trends of median value between BND and hiatus area during Valsalva manoeuvre, distensibility, respectively. The results showed no significant correlation either between BND and hiatus area during Valsalva manoeuvre (p = 0.590) or between BND and distensibility (p = 0.073).
Discussion
The purpose of this study was to characterise the changes in BND and levator hiatus dimensions in Asian primiparas at 5-time points (during the third trimester and short-term postpartum) using transperineal 4D ultrasound. Previous studies have documented increased BND after vaginal delivery (Peschers et al. Citation1996, Dietz et al. Citation2002), and a definition of abnormal (hypermobile) BND with 2.5 cm or a higher value was suggested, as it showed a significant association with urodynamic stress incontinence (Naranjo-Ortiz et al. Citation2016). Although the value of BND was less than 2.5 cm in all participations assessed at 5 time-points, we did observe a continued increase of BND until 6 weeks postpartum followed by a recovery trend. Another study demonstrated that this trend of recovery can continue to 6 months postpartum, but the BND at 12 months after vaginal delivery was still significantly higher than the values at 21 weeks of gestation (Staer-Jensen et al. Citation2015). This unrecoverable change in BND may be one of the reasons for the high risk of postpartum urinary incontinence.
The levator anus muscle is the main supporting muscle for the pelvic organs. The levator hiatus area assessed at rest and during contraction manoeuvre reflects the length of the levator anus muscle fibre during relaxation and contraction, respectively. The contractility was further calculated by the rest-to-contraction difference of the levator hiatal area, reflecting the overall contractile ability of the levator anus muscle. Previous studies demonstrated a significantly increased levator hiatus area during contraction at 36 weeks gestation (van Veelen et al. Citation2014b). In our study, both the hiatus area at rest and during contraction manoeuvre showed a gradual decrease; in addition, the change in contractility showed an increasing trend from 2 weeks postpartum onwards, indicating that the recovery trend in the contractility of the levator anus muscle began within 2 weeks postpartum, which is consistent with previous findings (Tunn et al. Citation1999, Van de Waarsenburg et al. Citation2018).
The distensibility was calculated by the rest-to-Valsalva difference of the levator hiatal area. Both the distensibility and the size of the levator hiatus area during Valsalva manoeuvre reflect the ability of the levator anal muscles to resist an increase in abdominal pressure. In previous studies, the levator hiatus area during Valsalva manoeuvre was shown to be significantly increased after vaginal delivery (van Veelen et al. Citation2014b, Staer-Jensen et al. Citation2015). In our study, the distensibility was lowest at 2 weeks postpartum followed by a continued increase, which was consistent with the increasing trend of levator hiatus area during Valsalva manoeuvre from 2 weeks postpartum, indicating a continually reduced resistance ability of the levator hiatus muscle throughout the 12 weeks postpartum. It is worth noting that the lowest value of distensibility observed at 2 weeks postpartum may be attributable to the reluctance of puerpera to perform maximum Valsalva manoeuvre shortly after delivery (Van de Waarsenburg et al. Citation2018).
It is reported that levator avulsion increased the levator hiatus area and the mobility of bladder neck (Shek et al. Citation2010). Furthermore, the avulsion was previously shown to be associated with increased BND postpartum (Dietz and Lanzarone Citation2005). However, the change of BND was not related to the change of either levator hiatus area or distensibility in our study, indicating that the BND may be associated with the levator hiatus area only under conditions of levator avulsion; this aspect needs to be further investigated but was beyond the scope of the study.
On the other hand, previous studies have demonstrated that nulliparous Caucasians have larger hiatal area during Valsalva manoeuvre compared with Asians (Cheung et al. Citation2015). Besides, black nulliparous have greater levator hiatal area compared with South Asian and Caucasian (Abdool et al. Citation2017), indicating distinct inter-racial differences concerning the dimensions of levator hiatal area. The overall trends of change in BND and levator hiatal area after vaginal delivery in our study population (exclusively Asian women) are consistent with those in similar studies conducted in the European region (Van de Waarsenburg et al. Citation2018), although the absolute values may be different, which needs further confirmation in future studies with larger sample size. Furthermore, the normal range of levator hiatal area and distensibility in Asian women are still unclear and need to be further established.
Strengths and limitations
The strength of this study is that this was the first longitudinal study of Asian primipara women to study the temporal regeneration in pelvic floor function in the early postpartum period by intensively monitoring the bladder neck mobility and levator hiatus dimensions at multiple time points. We further assessed the correlation between regeneration of the BND and levator hiatus. The limitation of this study includes the small number of participants and relatively short-term follow-up periods. In addition, we did not perform the sample size calculation as there was no similar data available from the literature. Nevertheless, as a prospective study, our results may provide a reference for a large-scale study in the future.
Conclusion
In Asian primipara, the recovery of bladder neck mobility after vaginal delivery begins at 6 weeks postpartum, while the levator hiatus muscle begins to recover within the first 2 weeks postpartum. In addition, the changes in BND showed no correlation with the changes in levator hiatus distensibility. This information could be useful when defining the best time to start postpartum secondary prevention measures.
Supplemental Material
Download MS Excel (14.5 KB)Declaration statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abbas, S., et al., 2019. AIUM/IUGA practice parameter for the performance of urogynecological ultrasound examinations: developed in collaboration with the ACR, the AUGS, the AUA, and the SRU. Journal of Ultrasound in Medicine., 38 (4), 851–864.
- Abdool, Z., Dietz, H. P. and Lindeque, B. G., 2017. Ethnic differences in the levator hiatus and pelvic organ descent: a prospective observational study. Ultrasound in Obstetrics & Gynecology, 50 (2), 242–246.
- Blomquist, J. L., et al. 2018. Association of delivery mode with pelvic floor disorders after childbirth. JAMA, 320 (23), 2438–2447.
- Bump, R. C., et al., 1996. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. American journal of Obstetrics and Gynecology, 175 (1), 10–17.
- Bump, R. C. and Norton, P. A., 1998. Epidemiology and natural history of pelvic floor dysfunction. Obstetrics and Gynecology Clinics of North America, 25 (4), 723–746.
- Cheung, R. Y., et al., 2015. Pelvic floor muscle biometry and pelvic organ mobility in East Asian and Caucasian nulliparae. Ultrasound in Obstetrics & Gynecology, 45 (5), 599–604.
- Cheung, R. Y. K., et al., 2019. Pelvic organ prolapse in Caucasian and East Asian women: a comparative study. Ultrasound in Obstetrics & Gynecology, 53 (4), 541–545.
- DE Araujo, C. C., et al., 2018. Does vaginal delivery cause more damage to the pelvic floor than cesarean section as determined by 3D ultrasound evaluation? A systematic review. International Urogynecology Journal, 29 (5), 639–645.
- Dietz, H. P., 2006. Pelvic floor trauma following vaginal delivery. Current opinion in Obstetrics & Gynecology, 18 (5), 528–537.
- Dietz, H. P., Clarke, B. and Vancaillie, T. G., 2002. Vaginal childbirth and bladder neck mobility. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 42 (5), 522–525.
- Dietz, H. P. and Lanzarone, V., 2005. Levator trauma after vaginal delivery. Obstetrics and Gynecology, 106 (4), 707–712.
- Dietz, H. P., et al., 2016. Warping of the levator hiatus: how significant is it? Ultrasound in Obstetrics & Gynecology, 48 (2), 239–242.
- Graham, C. A. and Mallett, V. T., 2001. Race as a predictor of urinary incontinence and pelvic organ prolapse. American Journal of Obstetrics and Gynecology, 185 (1), 116–120.
- Hagen, S., et al., 2017. Pelvic floor muscle training for secondary prevention of pelvic organ prolapse (PREVPROL): a multicentre randomised controlled trial. Lancet, 389 (10067), 393–402.
- Hagen, S., et al., 2009. Psychometric properties of the pelvic organ prolapse symptom score. BJOG : An International Journal of Obstetrics and Gynaecology, 116 (1), 25–31.
- Naranjo-Ortiz, C., et al., 2016. What is normal bladder neck anatomy? International Urogynecology Journal, 27 (6), 945–950.
- Peschers, U., et al., 1996. Changes in vesical neck mobility following vaginal delivery. Obstetrics and Gynecology, 88 (6), 1001–1006.
- Reimers, C., et al., 2019. Risk factors for anatomic pelvic organ prolapse at 6 weeks postpartum: a prospective observational study. International Urogynecology Journal, 30 (3), 477–482.
- Shek, K. L., Kruger, J. and Dietz, H. P., 2012. The effect of pregnancy on hiatal dimensions and urethral mobility: an observational study. International Urogynecology Journal, 23 (11), 1561–1567.
- Shek, K. L., Pirpiris, A. and Dietz, H. P., 2010. Does levator avulsion increase urethral mobility? European Journal of Obstetrics, Gynecology, and Reproductive Biology, 153 (2), 215–219.
- Staer-Jensen, J., et al., 2015. Postpartum recovery of levator hiatus and bladder neck mobility in relation to pregnancy. Obstetrics and Gynecology, 125 (3), 531–539.
- Staer-Jensen, J., et al., 2013. Ultrasonographic evaluation of pelvic organ support during pregnancy. Obstetrics and Gynecology, 122 (2 Pt 1), 329–336.
- Toprak Celenay, S., et al., 2022. The effects of pelvic floor muscle training combined with Kinesio taping on bladder symptoms, pelvic floor muscle strength, and quality of life in women with overactive bladder syndrome: a randomized sham-controlled trial. Physiotherapy Theory and Practice, 38 (2), 266–275.
- Tunn, R., et al., 1999. MR imaging of levator ani muscle recovery following vaginal delivery. International Urogynecology Journal and Pelvic Floor Dysfunction, 10 (5), 300–307.
- VAN DE Waarsenburg, M. K., et al., 2018. Recovery of puborectalis muscle after vaginal delivery: an ultrasound study. Ultrasound in Obstetrics & Gynecology, 52 (3), 390–395.
- VAN Veelen, A., Schweitzer, K. and Van Der Vaart, H., 2014a. Ultrasound assessment of urethral support in women with stress urinary incontinence during and after first pregnancy. Obstetrics and Gynecology, 124 (2 Pt 1), 249–256.
- VAN Veelen, G. A., Schweitzer, K. J. and Van Der Vaart, C. H., 2014b. Ultrasound imaging of the pelvic floor: changes in anatomy during and after first pregnancy. Ultrasound in Obstetrics & Gynecology, 44 (4), 476–480.
- Zarate-Kalfopulos, B., et al., 2012. Differences in pelvic parameters among Mexican, Caucasian, and Asian populations. Journal of Neurosurgery. Spine, 16 (5), 516–519.