

Abstract
Two-round Delphi study carried out in Spain. Three theme-based blocks were set out: 1) Patient profiles: therapeutic goal and parameters to be analysed according to POSEIDON patient profiles; 2) Ovarian stimulation protocols with antagonists: monotherapy (FSH) vs combined therapy (FSH + LH/HMG); 3) Safety and effectiveness of the devices. The antral follicle count and the anti-Müllerian hormone level were considered indicators that can be used to predict ovarian response. More than 80% of the participants agreed that FSH monotherapy is the recommended regimen in normal/hyper-responsive patients of < 35 years of age; that 150–300 IU is the dose to be used in ovarian stimulation in monotherapy depending on clinical parameters; and that FSH monotherapy improves patients’ comfort compared to two combined drugs. It was unanimously considered that the type of device used by the patient influences the comfort of the treatment.
What is already known on this subject? There is currently no consensus on the optimal treatment for controlled ovarian stimulation for patients undergoing IVF which leads to highly variable clinical practices.
What the results of this study add? This study’s strong point is that, since it is a consensus, it has been possible to include more topics than would normally be dealt with in a systematic review or guidelines, which are generally based on a strict method that restricts the scope of the research. Experts have reached a consensus on most of the statements and based on these they have issued consensus statements that will enable the optimal use of gonadotropins in IVF.
What the implications are of these findings for clinical practice and/or further research? This Delphi consensus provides a real-life clinical perspective on gonadotropin usage in IVF.
IMPACT STATEMENT
Introduction
Ovarian stimulation is crucial in each cycle of in vitro fertilisation (IVF) because the development of a sufficient number of follicles and attainment of a sufficient number of oocytes increases not only the live birth rate per cycle but also the cumulative live birth rate per cycle of treatment (Drakopoulos et al. Citation2016; Siristatidis, Citation2013).
Ovarian stimulation faces different challenges. On the one hand, the live birth rate per mature oocyte retrieved is lower than 5% (Goldman et al. Citation2013). On the other, the number of oocytes necessary to obtain at least one live birth increases exponentially with age (Goldman et al. Citation2017). Furthermore, a significant number of patients (from 9% to 24%) show a poor ovarian response (POR) to stimulation with exogenous gonadotropins (Roque et al. Citation2021). As a result, low rates of pregnancy and live births are obtained, both varying from 3% to 14% (Drakopoulos et al. Citation2016; Humaidan et al. Citation2017; La Marca et al. Citation2016; Tarlatzis et al. Citation2003; Ulug et al. Citation2003).
In order to predict the clinical response to stimulation and choose the most appropriate protocol, patients should be stratified according to ovarian reserve markers (La Marca et al. Citation2016). However, the choice of a marker is controversial and there is still debate as to what marker (or combination of them) is the most suitable (Bulletti et al. Citation2021).
The POSEIDON criteria stratify patients into four groups depending on a combination of quantitative and qualitative parameters (Alviggi et al. Citation2016). They are based on the woman’s age, ovarian reserve biomarkers, ovarian sensitivity to exogenous gonadotropins, and the number of oocytes retrieved in an IVF cycle (Alviggi et al. Citation2016).
The ‘ideal’ approach to performing ovarian stimulation with POR patients is still not known in terms of medication type, dose and devices used (Bulletti et al. Citation2021). There is no single procedure that appears to clearly improve IVF outcomes for this subgroup of patients, and clinical trials are generally highly biased (Papathanasiou, et al. Citation2016). Various ovarian stimulation protocols have been put forward that use exogenous FSH combined with gonadotropin-releasing hormone (GnRH) analogues (Bulletti et al. Citation2021). Another point of discrepancy is whether to use a combined treatment of FSH with luteinising hormone (LH), hormones with an LH effect, or else monotherapy with FSH (Ferrando et al. Citation2020).
It can be concluded that there is currently no consensus on the optimal treatment for controlled ovarian stimulation for POR patients undergoing IVF (Olgan and Humaidan Citation2017; Pandian et al. Citation2010; Papathanasiou, et al. Citation2016), which leads to highly variable clinical practices.
Given this background, this study took up the following goals: 1) To identify the points of agreement or disagreement as regards the use of gonadotropins in IVF in Spain; and 2) To issue recommendations to optimise the use of gonadotropins in IVF, both conventionally and using IVF-ICSI.
Method
Scientific committee and panel of experts
This project was carried out using the Delphi method from March to December 2021 in Spain. Initially, an advisory committee was set up tasked with analysing the main controversies in the sphere of ovarian stimulation in IVF, drawing up a questionnaire, interpreting the results from the Delphi rounds and critically reviewing the final report.
The committee members were chosen based on the following: they should be specialists and spend most of their working days in IVF sites (public or private); belong to a scientific society in this field; and be authors of publications or communications or have participated in clinical trials in the sphere of IVF.
In order to answer the questionnaire, a panel of experts was created with 40 fertility specialists from public and private sites with extensive experience in IVF and from all regions in the country.
As this study was based on a Delphi survey ethics approval was not required.
Creating statements. Questionnaire
The advisory committee first identified the areas of uncertainty that should form the basis for the questionnaire’s structure. Three theme-based blocks were set out: 1) Patient profiles: therapeutic goal and parameters to be analysed based on POSEIDON patient profiles; 2) Ovarian stimulation protocols: monotherapy (FSH) vs combined therapy (FSH + LH/HMG); 3) Safety and effectiveness of the devices.
Each member of the committee proposed different statements for the questionnaire with their corresponding bibliographic basis. To do so, the guidelines, protocols and other available evidence were reviewed, putting them into context with each committee member’s clinical experience. A work meeting was held to pool all of the statements and validate the choices. The final questionnaire contained 33 statements divided into five blocks or sub-blocks. It was posted on a microsite that the participants accessed via a web link with a user password.
Statistical analysis and interpretation of results
Two Delphi rounds were carried out. In each of them, the panel of participants scored each statement on a 9-point Likert scale. The level of agreement was classified as 1–3 (disagree), 4–6 (neither agree nor disagree), or 7–9 (agree).
The mean values (standard deviation) were calculated, as well as the median and interquartile range (p25–p75) for each of the questionnaire’s items. The level of significance was measured with the Kolmogorov-Smirnov goodness-of-fit test for distribution.
The criteria for consensus included ‘unanimity’ when 100% of participants agreed on the same Likert scale category, ‘consensus’ when there was agreement among ≥ 80% of participants, ‘majority’ when there was agreement among ≥ 66% of participants, and ‘disagreement’ when there was agreement among < 66% of the participants. For the purposes of this analysis, the ‘unanimity’, ‘majority’ and 'consensus’ groups were considered all together as consensus.
After the first round, the questions that did not reach a consensus in replies went on to the second, reformulating the ones whose wording could be improved. When the statistical analysis of the results was available, the advisory committee met to discuss and define the conclusions from the study.
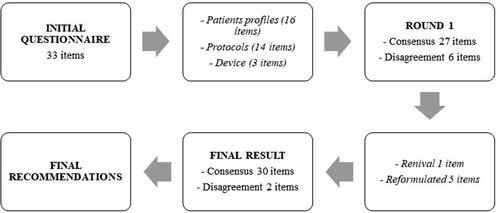
The initial questionnaire contained 33 statements divided among the three aforementioned blocks (with 16, 14 and 3 statements respectively).
Patient profiles
Parameters to stratify patients with a low ovarian response: 9 statements
Goals of the ovarian stimulation treatment: 7 statements
Ovarian stimulation protocols: monotherapy (rFSH) vs. combined therapy (rFSH + LH/HMG) with antagonists
Monotherapy: 10 statements
Combined therapy: 4 statements
Safety/efficiency of the device: 3 statements
Results
The questionnaire was answered by 40 fertility specialists. The participating entities are listed in .
Table 1. Participating sites.
shows the process of Delphi rounds. In the first round, a consensus was reached for 27 of the 33 matters raised. Of the six remaining questions, one was eliminated after being reviewed by the committee and considering that consensus would not be reached, while the rest went on to the second round, having been reformulated to make them more understandable, so that the final results included 32 statements.
Figure 1. Delphi study flow chart.
shows the results from the Delphi study.
Table 2. Final results from the Delphi study. Statements that did not reach consensus by the end of the study are marked in italics.
Discussion
This Delphi consensus provides a real-life clinical perspective on gonadotropin usage in IVF. The experts reached a consensus on most of the statements and based on these they have issued recommendations () that will enable optimal use of gonadotropins in IVF, whether conventionally or as IVF-ICSI.
Table 3. Recommendations to optimise the use of gonadotropins in IVF, both conventionally and in IVF-ICSI.
As regards the parameters for stratifying patients with low ovarian response, initially there are different parameters available to stratify the patients, such as age, baseline follicle-stimulating hormone (FSH) concentration, anti-Müllerian hormone (AMH) concentration, and the antral follicle count (AFC), used alone or in combination via algorithms or clinical nomograms. Despite this, the choice of marker is controversial and there is still debate as to what marker (or combination of them) is the most suitable (Bulletti et al. Citation2021).
Although other authors have described baseline FSH, body mass index and older age as predictors of ovarian response, the experts considered antral follicle count and the AMH value to be predictors of response, which are also indicators that are preferentially recommended by the guidelines of the European Society of Human Reproduction and Embryology (Bosch et al. Citation2020) compared to other markers. The participants agreed on recommending antral follicle counts for all patients before stimulation and in each cycle. The experts also consider that when a previous cycle is available, an antral follicle count or a determination of AMH should be carried out, but that it is unnecessary to measure the basal FSH.
Other authors have described factors such as baseline FSH, BMI, age or the number of follicles smaller than 11 mm as the most conclusive variables for patients under 35 years of age treated with recombinant FSH (rFHS) monotherapy (Howles et al. Citation2006).
As for the goals of treatment for ovarian stimulation, there was agreement of greater than 80% that the goal of ovarian stimulation for normal-responding patients could be set at obtaining 10–15 oocytes. There was also consensus that the adequate number of oocytes to be obtained in a cycle may vary depending on the patient’s age and clinical profile, with a higher risk of complications if the result is greater than 20 oocytes; and that the increase in this risk determines the number of oocytes to be obtained in an ovarian stimulation cycle. In this vein, a recent Delphi study by Bulletti et al has revealed a broad consensus on assertions such as the goal of 8–14 oocytes retrieved after ovarian stimulation in fresh cycles (Bulletti et al. Citation2021). According to data from the National Registry of the Spanish Fertility Society (SEF) for 2019 (Sociedad Española de Fertilidad, Citation2019), the estimated number of oocytes necessary to achieve pregnancy was 14.3, and the number of inseminated or injected oocytes necessary to achieve pregnancy was 11.3 (in both fresh and cryopreserved transfers) (Sociedad Española de Fertilidad, Citation2019).
In terms of the ovarian stimulation protocols, a consensus was achieved in all of the items in this block. The experts agreed that the most usual indications for receiving ovarian stimulation treatment combined with LH are an age of over 35 years and poor response in previous cycles, although the scientific evidence is controversial, to say the least. It was unanimously accepted that other indications for adding LH-acting drugs are excessive pituitary LH suppression or a lack of response to FSH alone in previous cycles.
As regards ovarian stimulation, there is no single intervention that clearly improves IVF outcomes for patients with poor ovarian response. In general, clinical trials give controversial results (Papathanasiou et al. Citation2016). In a systematic review of 75 clinical trials carried out with POR patients over 15 years, there was a notable heterogeneity detected in defining this type of patient and in the interventions studied, as well as serious methodological problems (Papathanasiou et al. Citation2016). Only 10% of the trials reported a significant improvement in reproductive outcomes after applying different protocols, many of which were based on a single clinical trial (Papathanasiou et al. Citation2016).
Although there are guidelines on ovarian stimulation in IVF-ICSI published in 2019 by the ESHRE (Bosch et al. Citation2020), they are limited by the fact that only a small proportion of patients are included in randomised controlled trials; it is estimated that only 35% of POR patients would meet the inclusion criteria used in large clinical trials (Orvieto et al. Citation2021). Thus, prospective studies with an adequate sample size and statistical power are still needed to respond to the clinical questions raised about ovarian stimulation for these patients.
Some authors have put forward different protocols using exogenous FSH combined with gonadotropin-releasing hormone (GnRH) analogues, whether agonist or antagonist (Bulletti et al. Citation2021). On the one hand, proper individualisation of the FSH dose has been put forward as one of the most sensitive steps to give a successful outcome and reduce complications from IVF (Bulletti et al. Citation2021). On the other, fixed-dose gonadotropin stimulation regimens (as opposed to variable doses during stimulation) have been considered a suitable option for some patients due to their lower cost and greater comfort, with fewer follow-up visits compared to the protocol with variable doses of gonadotropins (Bulletti et al. Citation2021). Another point of discrepancy is whether to use monotherapy wit FSH or else combine FSH with luteinising hormone (LH) or hormones with an LH effect (Ferrando et al. Citation2020). The scarcity of scientific evidence and the variability in clinical practice have prompted several Delphi studies to seek consensus (Bulletti et al. Citation2021; Orvieto et al. Citation2021).
The clinical effectiveness of rFSH monotherapy has been demonstrated in both clinical trials and real-life studies (Ferrando et al. Citation2020; Selman and Rinaldi Citation2016; Vlaisavljević et al. Citation2010; Strowitzki et al. Citation2016). In one of them, carried out in Spain with 1,222 patients treated in 26 sites, the pregnancy rates varied from 23.2% in poor responders to 37% in normal-responders (Ferrando et al. Citation2020).
The range of rFSH doses chosen by experts for ovarian stimulation protocols generally coincides with the range published in the ESHRE guide, which recommends doses ranging from 150 IU for good responders to 300 IU for poor responders (Bosch et al. Citation2020).
The results obtained in terms of safety and efficiency of the device agree with various studies comparing devices used in ovarian stimulation. However, these show differences in the reduction of handling errors (Imthurn et al. Citation2014; Saunders et al. Citation2020), comfort of use (Quintero et al. Citation2016) and the patient’s preference (Quintero et al. Citation2016).
This study’s strong point is that, since it is a consensus, it has been possible to include more topics than would normally be dealt with in a systematic review or guidelines, which are generally based on a strict method that restricts the scope of the research. Nevertheless, the consensus also has its limitations. For example, not all of the statements reached 100% agreement. Furthermore, although these recommendations represent experts’ points of view, they are not universal. The patient’s individual characteristics should always be taken into account before choosing the type of treatment.
We trust that this analysis will provide a contribution in improving care and therapeutic outcomes for POR patients undergoing IVF.
Conclusions
This Delphi study gives relevant data regarding the clinical reality of ovarian stimulation for POR patients undergoing IVF in Spain: 1) The different gonadotropins cannot alter the quality of the oocytes obtained; 2) The goal of ovarian stimulation is to obtain an adequate number of oocytes (in poor responders this is the maximum number possible, and in normal- or hyper-responders it is between 10 and 15); 3) The starting dose is determined well by response prediction factors; 4) The most valid prediction factor is the response in a previous cycle; 5) If there is no previous cycle, the antral follicle count and AMH value are the most reliable indicators of response.
This practical perspective is of great value in a field with numerous clinical questions raised and a high variability in clinical practice due to the scarcity of conclusive scientific evidence.
Acknowledgements
The authors would like to express their gratitude to the experts who have taken part as panellists in the Delphi study. Puerta del Mar Hospital, Cádiz; Reina Sofía Hospital, Córdoba; Virgen de las Nieves, Granada; Gutenberg Centre, Málaga; Juan Ramón Jiménez Hospital, Huelva; Hospital of Jaén, Jaén; Virgen del Rocío Hospital, Seville; IVI Clinic, Seville; Montpellier Reproduction Unit, Zaragoza; University Complex of the Canary Islands, Santa Cruz de Tenerife; Hospital of the Canary Islands, Las Palmas; Marqués de Valdecilla Hospital, Santander; Bernabéu Institute, Albacete; Clinical Hospital of Valladolid, Valladolid; CIRH, Barcelona; Eugin Clinic, Barcelona; Ginefiv, Barcelona; Clinical Hospital, Barcelona; Hospital of Santa Creu i Sant Pau, Barcelona; IVI Clinic, Barcelona; Hospital Quirón Salud, Barcelona; Embryogyn, Tarragona; IVI Clinic, Madrid; Ginefiv, Madrid; San Carlos Clinical Hospital, Madrid; Gregorio Marañón Hospital, Madrid; Bernabéu Institute, Madrid; IVF Life, Madrid; Institute of Assisted Reproduction Quirón Salud, Pamplona; UR Vistahermosa, Alicante; IVI Clinic, Valencia; CERHA Extremadura Centre for Assisted Human Reproduction, Badajoz; IVI Clinic, Vigo; Hospital Son Espases Reproduction Unit, Majorca; Bernabéu Institute, Majorca; IVI Clinic, Majorca; Donostia Hospital, Guipuzcoa; Cruces Hospital, Biscay; IVI Clinic, Murcia; Virgen de la Arrixaca Clinical Hospital, Murcia.
Disclosure statement
Julio Herrero has received honoraria for participating in conferences or courses of Gedeon Richter, Merck and Ferring. Luis Martínez Navarro has received honoraria for participating in conferences or courses of Merck, Ferring, Theramex and Gedeon Richter. José María Rubio has received honoraria for participating in conferences or courses of Ferring, Gedeon Richter, Theramex, Organon, Merck, Ediciones Mayo, Chiesi and Saned. Gorka Barrenetxea has received honoraria for participating in conferences or courses of Gedeon Richter and Organon. Gorka Barrenetxea, Cora Hernández, Manuel Muñoz, Fernando Sánchez, Jesús Zabaleta: report there are no competing interests to declare.
Additional information
Funding
References
- Alviggi, C., et al., 2016. A new more detailed stratification of low responders to ovarian stimulation: from a poor ovarian response to a low prognosis concept. Fertility and Sterility, 105 (6), 1452–1453.
- Bosch, E., Broer, S. and Griesinger, G., 2020. The ESHRE Guideline Group On Ovarian Stimulation. ESHRE guideline: ovarian stimulation for IVF/ICSI. Human Reproduction Open, 2020 (2), hoaa009.
- Bulletti, C., et al., 2021. How fixed versus variable gonadotropin dose during controlled ovarian stimulation could influence the management of infertility patients undergoing IVF treatment: a national Delphi consensus. Gynecological endocrinology: The Official Journal of the International Society of Gynecological Endocrinology, 37 (3), 255–263.
- Drakopoulos, P., Blockeel, C. and Stoop, D., 2016. Estimulação ovariana convencional e caracterization de embrião único para FIV/ICSI. Quantos oócitos precisamos para maximizar as taxas cumulativas de nascidos vivos após a utilização de todos os embriões frescos e congelados? Human Reproduction, 31, 370–376.
- Ferrando, M., et al., 2020. The continuum of ovarian response leading to BIRTH, a real-world study of art in Spain. Fertility Research and Practice, 6, 13.
- Goldman, K. N., et al., 2013. Oocyte efficiency: does live birth rate differ when analyzing cryopreserved and fresh oocytes on a per-oocyte basis? Fertility and Sterility, 100 (3), 712–717.
- Goldman, R. H., et al., 2017. Predicting the likelihood of live birth for elective oocyte cryopreservation: a counseling tool for physicians and patients. Human Reproduction, 32 (4), 853–859.
- Howles, C. M., et al., 2006. Predictive factors and a corresponding treatment algorithm for controlled ovarian stimulation in patients treated with recombinant human follicle stimulating hormone (follitropin alfa) during assisted reproduction technology (ART) procedures. An analysis of 1378 patients. Current Medical Research and Opinion, 22 (5), 907–918.
- Humaidan, P., et al., 2017. Efficacy and safety of follitropin alfa/lutropin alfa in art: a randomized controlled trial in poor ovarian responders. Human Reproduction, 32 (3), 544–555.
- Imthurn, B., et al., 2014. Evaluation of the use and handling of three different pen systems considered for in vitro fertilization treatment. Expert Opinion on Drug Delivery, 11 (12), 1859–1864.
- La Marca, A., et al., 2016. The use of ovarian reserve markers in IVF clinical practice: a national consensus. Gynecological Endocrinology : The Official Journal of the International Society of Gynecological Endocrinology, 32 (1), 1–5.
- Olgan, S. and Humaidan, P., 2017. GnRH antagonist and letrozole co-treatment in diminished ovarian reserve patients: a proof-of-concept study. Reproductive Biology, 17 (1), 105–110.
- Orvieto, R., et al., 2021. Optimising follicular development, pituitary suppression, triggering and luteal phase support during assisted reproductive technology: a delphi consensus. Frontiers in Endocrinology, 12, 675670.
- Pandian, Z., et al., 2010. Interventions for ‘poor responders’ to controlled ovarian hyper stimulation (COH) in in-vitro caracterization (IVF). Cochrane Database of Systematic Reviews, (1), CD004379.
- Papathanasiou, A., et al., 2016. Trends in 'poor responder’ research: lessons learned from RCTs in assisted conception. Human Reproduction Update, 22 (3), 306–319.,
- Quintero, L. A., Verdú, V. and De la Fuente, L., 2016. Evaluación del uso y manejo de la pluma Bemfola® en comparación con el de la pluma Gonal-f® y la pluma Puregon® en pacientes potenciales de FIV/donantes de ovocitos. Revista Iberoamericana de Fertilidad y Reproducción, 33 (3), 42–51.
- Roque, M., et al., 2021. The POSEIDON stratification – moving from poor ovarian response to low prognosis. JBRA Assisted Reproduction, 25 (2), 282–292.
- Saunders, H., Bjaergestad, L., Donat, H., 2020. Suitability of multidose vs single dose gonadotropin injection pens for ART use: A usability pen study. Poster presented at the American Society for Reproductive Medicine (ASRM) Virtual Congress, October 2020. Available in: https://www.fertstert.org/article/S0015-0282(20)31313-3/fulltext#relatedArticles. Last access September 2022.
- Selman, H. and Rinaldi, L., 2016. Effectiveness of corifollitropin alfa used for ovarian stimulation of poor responder patients. International Journal of Women’s Health, 8, 609–615.
- Siristatidis, C., Sergentanis, T. N., and Kanavidis, P., 2013. Hiperestimulação ovariana controlada para fertilização in vitro: impacto no cáncer ovariano, endometrial e cervical – uma revisão sistemática e metaanálise. Atualização Human Reproduction, 19, 105–123.
- Sociedad Española de Fertilidad 2019. Registro Nacional de Actividad 2019-Registro SEF. [Last access September 2022]. Available in: https://www.registrosef.com/public/docs/sef2019_IAFIVm.pdf
- Strowitzki, T., et al., 2016. Randomized, active-controlled, comparative phase 3 efficacy and safety equivalence trial of Ovaleap® (recombinant human follicle-stimulating hormone) in infertile women using assisted reproduction technology (ART). Reproductive Biology and Endocrinology, 14, 1.
- Tarlatzis, B. C., et al., 2003. Clinical management of low ovarian response to stimulation for IVF: a systematic review. Human Reproduction Update, 9 (1), 61–76.
- Ulug, U., et al., 2003. Conception rates following assisted reproduction in poor responder patients: a retrospective study in 300 consecutive cycles. Reproductive Biomedicine Online, 6 (4), 439–443.
- Vlaisavljević, V., et al., 2010. An observational study of assisted reproductive technology outcomes in new European Union member states: an overview of protocols used for ovarian stimulation. Current Medical Research and Opinion, 26 (4), 819–825.