

Abstract
To establish and verify a model for labour dystocia occurring in the active phase, this study retrospectively analysed the clinical data of primiparas with singleton cephalic full-term foetuses, who had delivered after a trial of labour. The Chi-square test, t-test, Mann–Whitney U test and multivariate logistic regression analysis were used for statistical analysis. Based on the model a nomogram was established using the R programming language. Multivariate logistic regression analysis showed that the foetal abdominal circumference, premature rupture of membranes (PROM), prolonged latent phase, foetal station and foetal position at the early stage of the active phase were independent factors influencing labour dystocia occurring in the active phase. The established model could effectively and accurately support clinicians in the early identification of labour dystocia to improve maternal and infant outcomes.
What is already known on this subject? Labour dystocia occurring during the active phase of the first stage, is the most commonly diagnosed as labour aberration. Previous studies have suggested that maternal age, body mass index, macrosomia and abnormal foetal position are the independent risk factors for labour dystocia. However, only the risk factors were reported, and few prediction models were established.
What do the results of this study add? This study uses data in the real world to establish a prediction model of full-term singleton primipara with labour dystocia occurring in the active phase by logistic regression analysis. Foetal abdomen circumference, PROM, prolonged latent phase, the foetal station and foetal position at the early stage of the active phase are independent factors influencing labour dystocia that occurs in the active phase. In addition, a nomogram is established as a visual graph to predict the probability of it.
What are the implications of these findings for clinical practice and/or further research? The nomogram based on the predictive model discarded complicated calculations and presented an easy visual graph-based method to predict the probability of labour dystocia occurring in the active phase. It helps to introduce interventions that could reduce the CS rate and occurrence of adverse maternal and foetal outcomes to ensure the safety of mothers and infants.
Impact statement
1. Background
Labour dystocia (LD), occurring during the active phase of the first stage, is the most commonly diagnosed as labour aberration. It is defined as abnormally slow or protracted labour, a lack of progressive cervical dilatation or no foetal head descent. It causes maternal and foetal complications such as postpartum bleeding, infection, foetal distress, mortality, increased caesarean sections (CSs) and unpleasant childbirth experiences (Conningham Citation2018). Therefore, diagnosing and dealing with the problem timely is important. Previous studies have suggested that maternal age, body mass index (BMI), macrosomia and abnormal foetal position are the independent risk factors for labour dystocia (American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins-Obstetrics Citation2016, Waldenström and Ekéus Citation2017, Hautakangas et al. Citation2018, Beta et al. Citation2019, Nahaee et al. Citation2020). However, only the risk factors were reported, and few prediction models were established. Therefore, this study uses data in the real world to establish a prediction model of full-term singleton primipara with labour dystocia occurring in the active phase by logistic regression analysis. In addition, a nomogram is established as a visual graph to predict the probability of it.
2. Materials and methods
2.1. Research object
This is a retrospective study. The data were retrospectively collected between 1 January 2015 and 30 April 2022 from women at the Affiliated Hospital of North Sichuan Medical College (NSMC), a university-based tertiary care centre with a medical radiation population of over 33 million. This study was approved by the ethics committee of NSMC (2022ER029-1).
In this research institution, we have been using the classic labour curve created by Friedman (Citation1954) to describe the progress of labour and guide intrapartum management until 1 January 2015. Since then, we adopted the guideline approved by The Obstetric Group of Obstetrics and Gynecology Branch of Chinese Medical Association (Citation2014). In this research institution, the labour assessment was evaluated by experienced midwives and attending physicians. Vaginal examinations were performed every 4 and 2 h during the latent and active phases, respectively, with intervals adjusted according to individual symptoms and labour progress. Women with cephalopelvic disproportion, pelvic size abnormalities, abnormality in soft tissues of the genital area, severe pregnancy complications, pathological obstetric conditions or complicated cardiac insufficiency were not allowed a vaginal delivery.
2.2. Inclusion criteria
The inclusion criteria were primiparas with the gestational age 37+0–41+6 weeks, singleton, cephalic, who delivered after trial of labour.
2.3. Exclusion criteria
The following classes of primiparas were excluded from the study:
Women with psychological and mental disorders.
Women with cervical dilation > 6 cm at admission, epidural analgesia, CS in latent phase and second stage of labour, CS because of foetal distress and elective CS during the active phase, operative vaginal delivery (vacuum or forceps), shoulder dystocia and induction of labour because of severe malformations such as full-term stillbirth, hydrocephalus and anencephaly.
Those with incomplete demographic data.
2.4. Diagnostic criteria
Labour dystocia occurring in the active phase was diagnosed when the membrane was broken and cervical dilatation was ≥ 6 cm; cervical dilatation was stopped at ≥ 4 h with regular uterine contractions or cervical dilatation was stopped at ≥ 6 h with uterine atony. Vaginal delivery (VD) is performed in primiparous women with a gestational age of 37+0–41+6 weeks, having normal labour progress, and the foetus was delivered naturally with a cephalic presentation.
2.5. Grouping criteria
According to the diagnostic criteria, the subjects were divided into labour dystocias occurring in the active phase (LDs group) and vaginal deliveries (VDs group).
2.6. Data collection
The clinical data was retrospectively recorded, including the maternal age, height, antepartum weight, gravidity, gestational age, foetal abdominal circumference, foetal position, station at the early stage of the active phase, delivery mode, indications of CS and proportion of cases with a premature rupture of membranes, labour induction, nuchal cord, prolonged latent phase.
2.7. Related definitions
Foetal abdominal circumference: Taken within one week before delivery by ultrasound through a transverse section with the umbilical vein into the liver and the abdomen perpendicular to the foetal spine.
The early stage of the active phase: The time when cervical dilation is 4–6 cm.
Prolonged latent phase: The latent phase lasts for more than 20 h in primiparas, from the beginning of regular labour contractions to the starting of the active phase.
Foetal station at the early stage of the active phase: The relationship between the lowest point of the foetal skull and the ischial spine at the early stage of the active phase, ranging from −3 to +3.
Foetal position at the early stage of the active phase: It determines the relationship between the foetal occiput and maternal pelvis at the early stage of the active phase such as in front of the pelvis for the occipital anterior position (OA). Not OA: any foetal position other than OA, including occipital posterior position (OP), occipital transverse position (OT), occipitopubic position, occipitosacral position, anterior asynclitism and face presentation.
2.8. Statistical analysis
Statistical analyses were conducted using the IBM Statistical Package for the Social Sciences (SPSS) version 25.0 software package for Windows. The nomogram was plotted using the ‘rms’ package, and the receiver operating characteristic (ROC) curves were drawn using the ‘ROCR’ package in R version 4.1.2. The sample size of this study conformed to the optimal combination of predictive factors and sample size stipulated by multivariate regression analysis (Norman Citation2012). Missing data accounted for less than 1.4%, which did not affect the analysis result and was deleted. The measurement data conforming to normal and non-normal distributions were described using X ± S and median (P25, P75), and the counting data were described using percentages. Univariate analysis was performed using the t-test, Mann–Whitney U test or Pearson Chi-Square (χ2) test. The variables with statistical significance in univariate analysis were included in the multivariate logistic regression, and risk factors were screened to establish the prediction model of labour dystocia occurring in the active phase. A nomogram was established using the R programming language based on the predictive model. The cut-off value was calculated using the Yoden index (sensitivity + specificity − 1). Discrimination and calibration evaluate the predictive ability of the model, while Bootstrap repeated sampling (1000 sampling times) was used for the internal model verification.
3. Results
From 1 January 2015 to 30 April 2022, 4026 full-term singleton cephalic primiparas had delivered after a trial of labour in the research institution, of which 2161 were included in this study. As shown in , the research objects included 184 (8.5%) and 1977 (91.5%) cases in the LDs and VDs groups, respectively. The women in LDs group were older [(27.6 ± 3.2) vs (26.6 ± 3.3) years, t = −3.620, p < .001] and had higher antepartum BMI [(27.4 ± 2.8) vs (26.3 ± 3.0) kg/m2, t = −4.774, p < .001], larger foetal abdomen circumference [(339.5(331.9,350.0)) vs (331.9(324.0,339.0)) mm, z = −8.398, p < .001] and delivered later [(281.0(276.2,284.0)) vs (277.0(273.0,282.0)) day, z = −5.288, p < .001] compared with those in VDs group. The incidence of PROM [29.9% (55/184) vs 19.5% (386/1977), χ2 =11.138, p = .001], labour induction [31.0% (57/184) vs 18.3% (361/1977), χ2 =17.453, p < .001], and the proportion of cases with prolonged latent phase [40.8% (75/184) vs 3.3% (65/1977), χ2 = 390.142, p < .001] were all higher in LDs group than in VDs group. The foetal station at the beginning of the active phase in LDs group were more higher(≦-1) [66.3%(122/184) vs 17.6% (347/1977), χ2= 235.451, p < .001] than that of in VDs group. The abnormal foetal position (not OA) at the beginning of the active phase [77.7%(143/184) vs 8.1% (160/19777), χ2= 676.882, p < .001] were more in LDs group than in VDs group. There were no significant differences in gravidity and the proportion of nuchal cord between the two groups (p > .05) ().
Table 1. Comparison of data about demographic and during labour between the two groups.
3.1. Establishment of the prediction model
Influencing factors of labour dystocia in the active phase were screened to build the prediction model, based on multivariate logistic regression analysis. Variables with a statistically significant difference from those above were the input, and the dependent variable was the delivery outcome (VDs = 0, LDs = 1). The multivariate analysis revealed PROM, foetal abdominal circumference, prolonged latent phase, foetal position, and station at the early stage of the active phase as the primary risk factors of labour dystocia that occurred in the active phase (). The risk factors mentioned above were imported into the R software, and the nomogram was constructed using the ‘rms’ package ().
Figure 1. Nomogram of prediction model.a aThe total points were obtained by adding the five factors, including premature rupture of membranes (PROM), foetal abdominal circumference (FAC), prolonged latent phase (PLP) and foetal position and station at the early stage of active phase (FPESAP, FSESAP). It represents predicting the occurrence probability of labour dystocia occurring in the active phase.
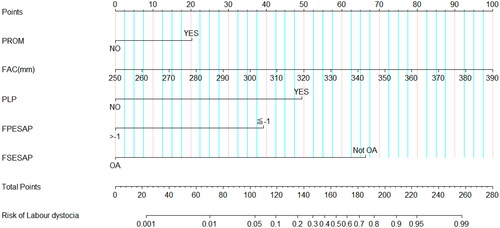
Table 2. Pre-labour and during labour predictors of LD that occurring in the active phase.
3.2. Evaluation and internal verification of nomogram
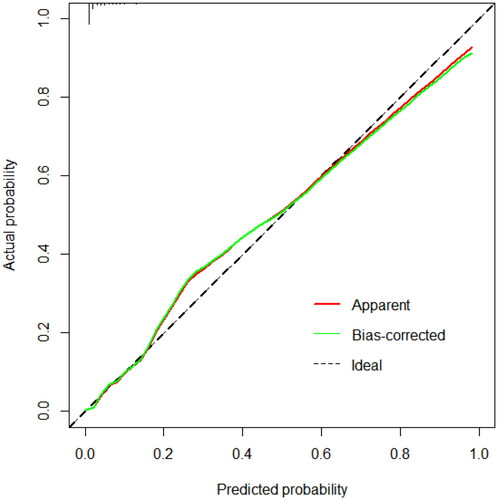
The ROC curve was drawn through the prediction probability of the nomogram (). The area evaluated the discrimination of the nomogram under the ROC curve. The AUC of the nomogram was 0.942 (95% CI: 0.922–0.962), indicating a better prediction performance. The cut-off value was 12.9%, with sensitivity and specificity of 0.842 and 0.929, respectively. The Hosmer–Lemeshow goodness-of-fit test revealed the goodness of fit of the nomogram (p = .536). Results of the internal validation using the Bootstrap method (1000 sampling times) verify that the predicted LD rates were consistent with the actual data ().
Figure 2. ROC of the nomogram.
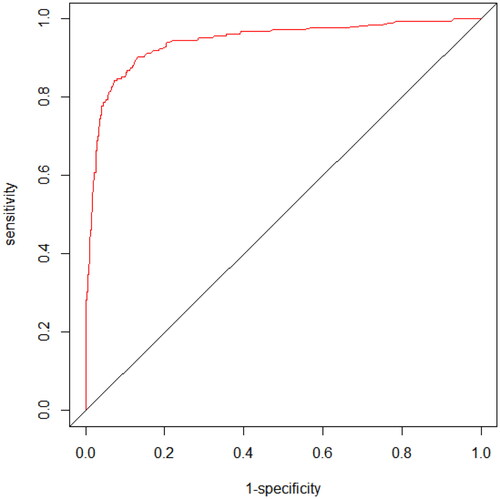
Figure 3. Internal verification calibration diagram of the nomogram.b bThe X- and Y-axis represent the predicted and actual occurrence probability of labour dystocia occurring in the active phase, respectively. The diagonal black dotted line represents the prediction of an ideal model, and the green solid line represents the performance of the nomogram; the closer the green line is to the diagonal black dotted line, the better is the prediction performance.
4. Discussion
The onset of the active phase has been a popular topic in labour research in recent years. Professor Friedman (Citation1954) proposed that the onset of the active phase should be 3 cm in the last century. However, in the past 10 years, labour researchers including Professor Zhang Jun questioned this, and considered that the onset of the active phase should be 6 cm (Cohen Citation2010), which was recognised by the American Association of Obstetrics and Gynaecology. Qi Shi, a member of our research team, conducted a prospective study on the labour process in 2015 and found that the possible acceleration point of labour process in most Chinese pregnant women was between 5 cm and 6 cm dilatation and at 4 cm for a small number of people (Shi Citation2016). With the accumulation of evidence, for the onset of the active phase, a 5 cm acceleration point was suggested in ‘Intrapartum care for a positive childbirth experience’ published by the World Health Organization (Citation2018) in February 2018. Thus, it is more reasonable to define the onset of the active phase as a time period at the acceleration point of 4–6 cm dilatation, which is defined as the early stage of the active phase and is the application time of the prediction model constructed in this study.
4.1. Analysis of related factors of labour dystocia occurring in the active phase
Labour dystocia often occurs in the active phase, in which case CS is required to end delivery. Although CS is convenient and not time intensive, it would negatively impact the mother and foetus if not handled properly. Therefore, understanding the related factors causing labour dystocia, which occurs in the active phase, is necessary to promote natural childbirth and reduce the rate of CS and the incidence of maternal and foetal loss in the perinatal period. In this study, by integrating the factors of pre-labour and during labour, we found premature rupture of membranes, foetal abdominal circumference, prolonged latent phase and foetal position and station at the early stage of the active phase as the risk factors causing labour dystocia occurring in the active phase.
The premature rupture of membranes before labour is a common complication in obstetrics. The incidence rate is about 2.7%–17.0%. It could lead to premature delivery, foetal distress, infection and dystocia, even fatally threatening the health of the mother and foetus (American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins-Obstetrics Citation2016). The premature rupture of membranes was often considered a warning sign of dystocia, most of which occurred in those who did not engage in the foetal head. It is caused by the gap between the foetal presentation and pelvis, communication between anterior and posterior amniotic fluid and uneven stress on the anterior amniotic sac. The premature rupture of membranes causes amniotic fluid loss. The uterine wall is close to the carcase and is prone to uncoordinated uterine contraction or blocked rotation of the foetal head, increasing the chance of dystocia (Waters and Mercer Citation2009).
Foetal weight is an important factor influencing obstetricians to evaluate the success of delivery. Foetal abdominal circumference is the most effective parameter for evaluating foetal weight (Hautakangas et al. Citation2018). Catalin pointed out that the increase in foetal weight in the third trimester was primarily manifested by the increased foetal abdominal circumference and not by the changes in the foetal head circumference and biparietal diameter, which was related to the continuous accumulation of fat and the accumulation and storage of liver glycogen (Catalin Citation2009). One systemic review reported that both foetal abdominal circumference and the estimated foetal weight are equally accurate in predicting macrosomia (Coomarasamy et al. Citation2005). Foetal macrosomia was recognised as one of the risk factors for intrapartum dystocia and other major maternal and foetal childbirth complications (American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins-Obstetrics Citation2016, Araujo Júnior et al. Citation2017). Therefore, the foetal abdominal circumference was considered an independent risk factor for dystocia (Henrichs et al. Citation2003).
The prolonged latent phase is the earliest sign of dystocia. However, by occurring in the early stages of labour, it is difficult to distinguish it from false labour. Hence, it is ignored, and an early treatment opportunity to prevent dystocia and the adverse outcome for the mother and foetus is missed (Bauer and Voutsos Citation2013, ACOG Committee Citation2019). A study of 10,677 women found that the longer the latent phase, the greater is the probability of CS. Moreover, the rate of postpartum haemorrhage, chorioamnionitis, blood transfusion and dystocia is increased (Grobman et al. Citation2018). The causes of a prolonged latent phase are uterine atony, cephalopelvic disproportion and abnormalities in pelvic size (Ängeby et al. Citation2018).
Souka et al. reported that the anterior occipital position was the most common position during labour, followed by the posterior and transverse occipital positions (Souka et al. Citation2003). These could be converted to the anterior occipital position during labour. However, the labour process, if stagnant, should be diagnosed as persistent occipital transverse or posterior position. In the first stage of labour, these were related to labour dystocia (Choi et al. Citation2016, Tempest et al. Citation2020). Abnormal foetal position can affect foetal head descent, making the head float high and resulting in labour dystocia. The foetal station was above the level of the ischial spine during the active phase, increasing the possibility of dystocia (Kimmich et al. Citation2018).
4.2. Application and advantages of the nomogram for predicting labour dystocia occurring in the active phase
Five risk factors, namely, premature rupture of membranes, foetal abdominal circumference, prolonged latent phase, and foetal position and station at the early stage of the active phase, were incorporated into the R software to construct the prediction nomogram of labour dystocia occurring in the active phase. The total score was obtained by adding the scores of all the risk factors according to the nomogram model at the early stage of the active phase. The value corresponding to the total score was the probability of labour dystocia occurring in the active phase. For example, a primipara who had just been admitted to the hospital had a premature rupture of membranes. The abdominal circumference of the foetus measured by B-ultrasound was approximately 348 mm. The latent phase lasted 18 h, and the foetal station revealed ‘−1’, and occipital posterior position, at a cervical dilation of 5 cm. The score based on the nomogram was 20 + 70 + 39 + 66.5 = 195.5, and the corresponding probability of dystocia was approximately 83%. The probability of dystocia was high and some interventions were needed to change the risk factors, for example, turning the abnormal foetal position into the anterior occipital position by hand or oxytocin for augmentation.
In previous studies, only the risk factors of labour dystocia were reported, and few prediction models were established. Nahaee (Citation2020) predicted labour dystocia in the active phase and found that a maternal height of less than 160 cm, low income, labour induction, epidural analgesia, maternal anxiety, dehydration and insufficient support from medical staff during delivery were the predictive factors of labour dystocia. However, the study primarily focussed on maternal factors and the lack of foetal factors, such as foetal weight, foetal station and position, affecting the labour progress. In our study, the multivariate logistic regression analysis integrated maternal and foetal data pre-labour and during labour to establish the prediction model of labour dystocia occurring in the active phase. The sensitivity and specificity of the proposed model were high, suggesting the clinical significance of the model. The nomogram based on the predictive model discarded complicated calculations and presented an easy visual graph-based method to predict the probability of labour dystocia occurring in the active phase. The included variables in this nomogram were simple and easy to obtain at the early stage of the active phase. For example, the abdominal circumference of the foetus, accurately obtained through B-ultrasound in the week before delivery, replaced the foetal weight, which could only be estimated before delivery. In addition, by using this prediction model, new team members can be trained to judge the labour situation, remind them of the focus that affects the progress of labour, consolidate their basic knowledge and translate it into clinical practice. Therefore, this model not only has certain clinical application value, but also can be used for team training and promote the homogenisation of labour management.
4.3. Limitations and future study prospects
First, this study only involved a single-centre population in this region. Because the selected centre treated critically ill pregnant women, there were relatively few pregnant women without contraindications to a trial of vaginal delivery, leading to a small number of included populations and a lack of external validation.
Second, all parameters related to labour progress were artificially evaluated. However, according to medical conventions, the subjective finger examination method was used for evaluation (Buchmann and Libhaber Citation2007, Zhang et al. Citation2010). The resulting judgement error is a common problem that was difficult to solve when studying the labour process. The midwifery team in this research institution was mostly permanent, receiving periodic skill assessments and training. In case of abnormal labour progress, attending physicians are requested for joint evaluation and treatment, developing certain homogeneity for the judgement of the labour process.
To solve the above limitations and deficiencies, we plan to conduct multi-centre and big data analysis to evaluate the prediction model performance externally.
5. Conclusion
Foetal abdomen circumference, PROM, prolonged latent phase, the foetal station and foetal position at the early stage of the active phase are independent factors influencing labour dystocia that occurs in the active phase. The prediction model and nomogram were established according to these factors to effectively and accurately predict the LD in the active phase for primipara. In addition, it can help clinicians in the early identification of labour dystocia in the active phase to improve maternal and infant outcomes. However, clinicians cannot simply rely on the model but also consider the actual situation of each pregnant woman to ensure the safety of mothers and infants.
Author contributions
The paper was co-authored by Liu Yanqing, Gong Qingquan and Yuan Yuhong. All authors agree to be responsible for all aspects of the work and approve the final manuscript submitted.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- ACOG Committee, 2019. Opinion no. 766: approaches to limit intervention during labour and birth. Obstetrics and Gynecology, 133, e164–e173.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins-Obstetrics, 2016. Practice Bulletin No. 173. Practice Bulletin No. 173: foetal macrosomia. Obstetrics and Gynecology, 128, e195–e209.
- Ängeby, K., et al., 2018. Prevalence of prolonged latent phase and labour outcomes: review of birth records in a Swedish population. Journal of Midwifery & Women’s Health, 63 (1), 33–44.
- Araujo Júnior, E., et al., 2017. Macrosomia. Best Practice & Research Clinical Obstetrics & Gynaecology, 38, 83–96.
- Bauer, C. and Voutsos, L.J., 2013. Preventing the first cesarean delivery: summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development’, Society for Maternal-Foetal Medicine, and American College of Obstetricians and Gynecologists workshop. Obstetrics and Gynecology, 121 (3), 686–687.
- Beta, J., et al., 2019. Maternal and neonatal complications of foetal macrosomia: cohort study. Ultrasound in Obstetrics & Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 54 (3), 319–325.
- Buchmann, E.J. and Libhaber, E., 2007. Accuracy of cervical assessment in the active phase of labour. BJOG : An International Journal of Obstetrics and Gynaecology, 114 (7), 833–837.
- Catalin, S., 2009. Spatiotemporal electromyography during human labour to monitor propagation of the uterine contraction wave and diagnose dystocia. American Journal of Obstetrics and Gynecology, 11, 53–55.
- Choi, S.K., et al., 2016. Sonographic assessment of foetal occiput position during labour for the prediction of labour dystocia and perinatal outcomes. The Journal of Maternal-Fetal & Neonatal Medicine, 29 (24), 3988–3992.
- Cohen, W.R., 2010. The natural history of the normal first stage of labour. Obstetrics and Gynecology, 116 (3), 772.
- Conningham, F.G., et al., 2018. Williams obstetrics. 25th ed, vol. 1. New York: McGraw-Hill Education, 214–219.
- Coomarasamy, A., et al., 2005. Accuracy of ultrasound biometry in the prediction of macrosomia: a systematic quantitative review. BJOG : An International Journal of Obstetrics and Gynaecology, 112 (11), 1461–1466.
- Friedman, E., 1954. The graphic analysis of labour. American Journal of Obstetrics and Gynecology, 68 (6), 1568–1575.
- Grobman, W.A., et al., 2018. Defining failed induction of labour. American Journal of Obstetrics and Gynecology, 218 (1), 122.e1–122.e8.
- Hautakangas, T., et al., 2018. Impact of obesity and other risk factors on labour dystocia in term primiparous women: a case control study. BMC Pregnancy and Childbirth, 18 (1), 304.
- Henrichs, C., et al., 2003. Detecting foetal macrosomia with abdominal circumference alone. The Journal of Reproductive Medicine, 48 (5), 339–342.
- Kimmich, N., et al., 2018. Impact factors on foetal descent rates in the active phase of labour: a retrospective cohort study. Journal of Perinatal Medicine, 46 (6), 579–585.
- Nahaee, J., et al., 2020. Preand during- labour predictors of dystocia in active phase of labour: a case-control study. BMC Pregnancy and Childbirth, 20 (1), 425.
- Norman, G., Monteiro, S., and Salama, S., 2012. Sample size calculations: should the emperor’s clothes be off the peg or made to measure? BMJ (Clinical Research ed.), 345, e5278.
- Shi, Q., et al., 2016. Labour patterns in Chinese women in Chongqing. BJOG: An International Journal of Obstetrics & Gynaecology, 123 (Suppl 3), 57–63.
- Souka, A.P., et al., 2003. Intrapartum ultrasound for the examination of the foetal head position in normal and obstructed labour. The Journal of Maternal-Fetal & Neonatal Medicine, 13 (1), 59–63.
- Tempest, N., Lane, S., and Hapangama, D., 2020. Babies in occiput posterior position are significantly more likely to require an emergency cesarean birth compared with babies in occiput transverse position in the second stage of labour: a prospective observational study. Acta obstetricia et Gynecologica Scandinavica, 99 (4), 537–545.
- The Obstetric Group of Obstetrics and Gynecology Branch of Chinese Medical Association, 2014. Specialist consensus on new labour standards and treatment. Chinese Journal of Obstetrics and Gynecology, 49, 486.
- Waldenström, U. and Ekéus, C., 2017. Risk of labour dystocia increases with maternal age irrespective of parity: a population-based register study. Acta Obstetricia et Gynecologica Scandinavica, 96 (9), 1063–1069.
- Waters, T.P. and Mercer, B.M., 2009. The management of preterm premature rupture of the membranes near the limit of foetal viability. American Journal of Obstetrics and Gynecology, 201 (3), 230–240.
- World Health Organization, 2018. WHO recommendations: intrapartum care for a positive childbirth experience [S/OL](2018-02-15) [2018-08-18]. Available from: http://www.who.int/reproductivehealth/publications/intrapartum-care guidelines/en/ [Accessed 06 Aug 2022].
- Zhang, J., et al., 2010. Contemporary patterns of spontaneous labour with normal neonatal outcomes. Obstetrics and Gynecology, 116 (6), 1281–1287.