

Abstract
The current study sought to investigate the effect of nimotuzumab combined with concurrent chemoradiotherapy (CCRT + Nim) on T lymphocyte subsets in middle-advanced CC. Firstly, patients with middle-advanced CC were administered CCRT or CCRT + Nim. Next, levels of T lymphocytes in peripheral blood of CC patients pre- or post-treatment and healthy females were determined by flow cytometry. The short-term efficacy was evaluated, and overall survival (OS) and progression-free survival (PFS) of patients were recorded. In addition, the correlation of T lymphocyte subsets post-treatment with OS/PFS was assessed with Pearson analysis. CC patients exhibited decreased total T cells/T helper cells/CD4+/CD8+ ratio and increased T suppressor cells/Tregs in peripheral blood. Meanwhile, CCRT and CCRT + Nim improved T lymphocyte subset imbalance, with CCRT + Nim exhibiting better efficacy. CCRT + Nim exhibited better short-term efficacy and higher PFS than CCRT, with no evident difference in OS. The levels of total T cells/T helper cells/T suppressor cells/Tregs were not significantly-correlated with OS/PFS, and the CD4+/CD8+ ratio was correlated with PFS but not OS. Collectively, CCRT + nimotuzumab ameliorate the imbalance of T lymphocyte subsets in peripheral blood of middle-advanced CC patients, and the CD4+/CD8+ ratio after therapy is correlated with PFS.
What is already known on this subject? The utilisation of Nimotuzumab targeting epidermal growth factor receptor (EGFR) combined with concurrent chemoradiotherapy (CCRT) as an efficient treatment for middle-advanced cervical cancer (CC) has garnered the attention of numerous researchers over the years. T cells represent a major immune cell type in the tumour microenvironment and serve as the basis for maintaining cellular immune functions.
What do the results of this study add? Our findings revealed that nimotuzumab combined with CCRT improves the abnormality of T lymphocyte subsets in peripheral blood of patients with middle-advanced CC, such that the CD4+/CD8+ ratio after treatment was significantly correlated with progression-free survival (PFS).
What are the implications of these findings for clinical practice and/or further research? CCRT of CC may have a short-term negative impact on the peripheral T-cell immune micro-environment, and the combination of nimotuzumab, cisplatin-based chemotherapy, and radiotherapy enhances the frequency of Tregs in peripheral blood. Our findings illustrated that nimotuzumab combined with CCRT can improve the imbalance of T lymphocyte subsets in peripheral blood of patients with middle-advanced CC. A better understanding of the mechanisms of these therapies will optimise the selection of patients most likely to benefit from treatment, serving as a reference for further research on the relationship between EGFR-specific T cells and clinical benefit in patients treated with nimotuzumab in combination with CCRT.
IMPACT STATEMENT
Introduction
Cervical cancer (CC) is regarded as the 4th most widespread malignancy and primary cause of cancer-associated deaths in women throughout the world, especially in low-income countries (Castle et al. Citation2021). Recent investigations have to come to light indicating that approximately 99.7% of CC cases are attributed to persistent high-risk human papillomavirus (HPV) infection (Okunade Citation2020). Fortunately, CC is regarded as highly preventable and can be cured if detected at early stages (Pimple & Mishra Citation2019). However, only a minority of CC patients are detected at the early stage (13% at stage I), and the vast majority are diagnosed at mid-to-late stages (35% at stage II, 44% at stage III, and 8% at stage IV) (Gopu et al. Citation2021), which are attributed to its asymptomatic nature at early stages. Meanwhile, treatment modalities largely depend on CC severity at diagnosis and resources available locally, with conservative and fertility-preserving surgery serving as the standard treatment option for early-stage CC (Cohen et al. Citation2019). Concurrent chemoradiotherapy (CCRT) represents a well-established treatment modality for locally advanced CC, and this approach is associated with improved patient survival (Matsuzaki et al. Citation2020). However, this regimen can result in chronic morbidity and adverse events, and the outcome of patients remains suboptimal (Naga Ch et al. Citation2018, Burmeister et al. Citation2022). Accordingly, it remains imperative to explore novel, effective treatment methods to prolong the survival time of patients and improve their quality of life.
Targeted therapy has received increasing attention as an efficient treatment, and in particular, epidermal growth factor receptor (EGFR) has emerged as an attractive potential target for CC treatment owing to its function in malignant transformation and tumorigenesis (Gopu et al. Citation2021). Inherently, EGFR forms a dimer by binding to ligands and activates the downstream signal transduction pathways, thereby inhibiting apoptosis and facilitating cell formation and angiogenesis (Liu et al. Citation2020, Muthusami et al. Citation2022). Essentially, over-expression of EGFR exhibits a close correlation with resistance to radiation and cytotoxic chemotherapy in squamous CC (Crowley et al. Citation2021). Meanwhile, nimotuzumab, a well-known IgG1 humanised monoclonal antibody, possesses the ability to competitively-block the binding of EGFR with its ligands, and the agent exhibits the advantages of unique pharmacodynamic properties, low toxicity, and low immunogenicity, which can be potentially utilised in the treatment of different epithelial tumours (Mazorra et al. Citation2018). The utilisation of nimotuzumab as a single agent, or in a combination with radiation and chemotherapy has been evaluated in solid tumours, with evidence suggesting that nimotuzumab can efficiently stabilise the disease for a long time while conferring very low toxicity (Cetina et al. Citation2015). To the best of our knowledge, there are very few clinical studies concerning the combination of nimotuzumab and CCRT in middle-advanced CC, and thus more exploration is still warranted.
Accumulating evidence further indicates that persistent HPV infection is tightly-associated with the body’s immunity, especially cervical T-cell immunity (Zhang et al. Citation2020). The functional state of T cells in the tumour microenvironment is essential for successful anti-tumour immunity (Zhao et al. Citation2020). Moreover, T lymphocyte subsets for the basis for the maintenance of the cellular immune function of the body, primarily including CD4+ and CD8+ T cells, of which CD4+ T cells regulate the differentiation and proliferation of immune cells to enhance the body immunity, while CD8+ T cells inhibit B-cells to produce antibodies, thereby diminishing the body immunity (Chraa et al. Citation2019). In light of the robust function of T cells, the current study set out to investigate the exact effect of nimotuzumab combined with CCRT (CCRT + Nim) on T lymphocyte subsets in the peripheral blood of patients with middle-advanced CC to provide novel insights into the clinical treatment for CC.
Methods
Ethics statement
The current study was ratified by the Ethics Committee for Clinical Investigations of Affiliated Hospital of Chengde Medical College (Approval number: 20220207001), and all experimentation complied with the ethical principles of medical research in the Declaration of Helsinki. Signed informed consent was obtained from each participant prior to enrolment. This study conformed to the Enhancing the QUAlity and Transparency Of health Research (EQUATOR) network guidelines.
Study subjects
A total of 150 patients with middle-advanced CC who were admitted at the Affiliated Hospital of Chengde Medical College from July 2017 to June 2019 were enrolled as study subjects, all of whom conformed to the following inclusion criteria: (1) age ≥18 years; (2) diagnosed as clinical stages IIA-IVA based on the 2009 International Federation of Gynaecology and Obstetrics (FIGO) classification system; (3) presented with primary CC; (4) presented without a history of CRT and other anti-tumour treatments; (5) treated with CCRT alone or its combination with nimotuzumab for at least two cycles; (6) in concert with the basic requirements of RT, including a Karnofsky Performance Status score of ≥60 and estimated survival of more than 3 months; (7) signed the informed consent and voluntarily underwent nimotuzumab treatment; (8) presented with complete follow-up data. Meanwhile, the exclusion criteria were as follows: (1) patients with contraindications to CRT; (2) patients allergic to drugs involved in this study; (3) combined with other primary malignancies; (4) presented with blood system diseases, autoimmune system diseases, and organ dysfunction, as well as acute and chronic infections; (5) pregnant or breastfeeding; (6) dying of non-CC causes. Additionally, another 80 healthy females during the same period were enrolled as controls (the control group), with a mean calculated age of 50.67 ± 4.33 years and a mean body mass index (BMI) of 22.36 ± 1.62 kg/m2. Their general data showed no evident differences compared with that of included patients (p > 0.05).
Treatment regimens
In accordance with different treatment regimens, all patients with middle-advanced CC were allocated into the CCRT group (N = 78) or the CCRT + Nim group (N = 72).
CCRT group: Intensity-modulated RT: The patients were asked to fill the bladder as much as possible within their tolerance, and uninterrupted scanning was performed by means of computed tomography (CT). Through CT image localisation, visual target areas such as the uterus, cervix, and tumour were delineated, and then the specific tumour targets were delineated, including lymph nodes located in the left and right common iliac vessels, presacral region, parametrium, and obturator foramen, with the upper bound to L4-5 and the lower bound to the lower edge of the obturator foramen. Next, a margin extension of 0.5–1 cm surrounding the tumour target area was regarded as the planning target volume (PTV), and meanwhile, the organs at risk such as the rectum, small intestine, and bladder were delineated. With the geometric centre of PTV as the centre field, irradiation was carried out with 15 MV X-rays from a linear accelerator electric multi-leaf collimator (23-EX, Varian, Palo Alto, CA, USA), with 6 coplanar fields. The prescription dose was calculated to be 50–55 Gy, and the dose of PTV was 54.5 Gy for 1.8–2.2 Gy/fraction and 4 fractions/week. Chemotherapy: All patients were intravenously infused with paclitaxel at a rate of 135 mg/m2 (11110040, Taiji Group, Chengdu, Sichuan, China) and cisplatin at 50–60 mg/m2 (Hansoh Pharmaceutical Group, Lianyungang, Jiangsu, China) once per week during RT. Prophylactic anti-emetics were routinely administered during chemotherapy.
CCRT + Nim group: The CCRT procedures were the same as above. Additionally, 200 mg nimotuzumab (S20080001, Biotech Pharma, Beijing, China) was diluted with normal saline, and then injected into patients via intravenous infusion for more than 60 min at 4 h prior to RT on the 1st, 8th, 15th, 22nd, 29th, 36th and 42nd day during RT. Cimetidine and dexamethasone were routinely administered prior to nimotuzumab treatment to prevent allergic reactions.
Both groups underwent continuous treatment for 2 cycles, with each cycle lasting 3 weeks.
Data and sample collection
Clinical data of all subjects were recorded at enrolment, including age, BMI, FIGO stage, histological type, histological differentiation degree, lymph node status, parametrial invasion, and tumour size prior to treatment. Additionally, 5 mL fasting venous blood samples were collected from all subjects at enrolment and CC patients in the morning of the 4th week after treatment, which were collected in ethylenediaminetetraacetic acid (EDTA) tubes (BD Vacutainer®, Plymouth, UK) at −80 °C for subsequent flow cytometry analysis of T lymphocyte subsets.
Flow cytometry
Flow cytometry was carried out in order to analyse the T lymphocyte subsets (T. Chen et al. Citation2020). CD3+CD45+ cells indicated the total T cells. Various T lymphocyte subsets, containing T helper cells (CD3+CD4+), T suppressor cells (CD3+CD8+), and regulatory T cells (Tregs; CD4+CD25+CD127Dim) were individually detected with an FC500MCL flow cytometer (Beckman Coulter, Chaska, MN, USA) using corresponding antibodies anti-CD3-PC5, anti-CD4-PE, anti-CD8-ECD, anti-CD4-PC5, anti-CD25-FITC, and anti-CD127-PE (all procured from Beckman Coulter). Briefly, 2 mL venous peripheral blood samples were collected into EDTA tubes for cytometric analysis, 50 μL whole blood per tube was incubated with monoclonal antibodies for 30 min in conditions void of light, and thereafter red blood cells were lysed using a buffer comprising 0.8% NH4Cl and 0.1% KHCO3 (pH 7.1–7.4). Following a rinse with phosphate-buffered saline (PBS), the cells were suspended with 200 µL PBS for detection of T lymphocyte subsets. The percentages of CD3+ T cells, CD3+CD4+ T cells, CD3+CD8+ T cells, and Tregs were calculated using the BD Multitest software (BD Biosciences, San Jose, CA, USA).
Evaluation of short-term efficacy and follow-up of patients
In accordance with the Response Evaluation Criteria in Solid Tumours (version 1.1) issued by the World Health Organisation, clinical response was initially examined by means of CT, magnetic resonance imaging, and gynecological examination at the 4th week post-treatment in order to assess the size and location of the tumour, the degree of invasion of adjacent structures, and lymph node metastasis. Efficacy evaluation results were divided into the following 4 grades: complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). CR was regarded as the disappearance of all lesions. PR was defined as a reduction in the longest diameter of target lesions of > 30% relative to the baseline. PD was considered as the appearance of new target lesions or an increase in target lesions of <20%. SD was defined as a reduction in lesion size of <30% or an increase in size of <20%. Overall response rate = CR + PR.
Patients were followed up by means of re-visitation or telephony to record overall survival (OS) and progression-free survival (PFS). OS was defined as the time from the beginning of the study to the last follow-up visit or death. PFS was defined as the time from enrolment to disease progression or death. The follow-up began in the 4th week after the last treatment and carried out every 3 months for 3 years.
Statistical analysis
Measurement data were statistically analysed and graphed using the GraphPad Prism 8.01 (GraphPad Software Inc., San Diego, CA, USA) and SPSS 21.0 (IBM Corp. Armonk, NY, USA) software. The normal distribution of continuous variables was verified using the Kolmogorov-SmiRnov. Measurement Data were displayed as mean ± standard deviation. The t-test was conducted for data comparisons between two groups, one-way analysis of variance (ANOVA) was utilised for comparisons among three groups, and Tukey’s multiple comparisons test was implemented for post-hoc analysis. The Chi-square test was adopted for analysis of categorical variables. The Kaplan–Meier curve was used for survival analysis. Pearson analysis was performed to examine the correlation between factors. A value of p < 0.05 was regarded as statistically significant.
Results
Comparative analysis of clinical baseline data
The clinical data of patients in the CRT group and CCRT + Nim group were compared and analysed, the results of which revealed that there were no significant differences in regard to parameters such as age, BMI, FIGO stage, histological type, histological differentiation degree, lymph node status, parametrial invasion, and tumour size prior to treatment between the CCRT group and CCRT + Nim group () (all p > 0.05), with comparability between groups.
Table 1. Comparative analysis of clinical baseline data.
Changes of T lymphocyte subsets in peripheral blood of patients with middle-advanced CC
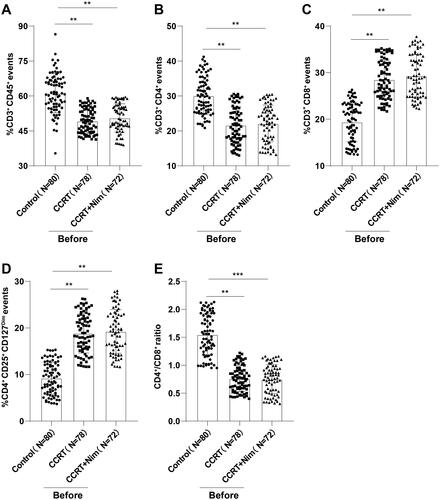
Thereafter, we determined the levels of T lymphocytes in peripheral blood of CC patients prior to treatment and healthy females, including total T cells (CD3+CD45+), T helper cells (CD3+CD4+), T suppressor cells (CD3+CD8+), and Tregs (CD4+CD25+CD127Dim). The representative flow cytometric diagram of CD3+CD4+/CD3+CD8+ cells was illustrated in Supplementary Figure 1 and the representative flow cytometric diagram of CD4+CD25+CD127Dim Tregs was illustrated in Supplementary Figure 2. Relative to the control group, the CCRT group and CCRT + Nim group prior to treatment presented with lowered total T cells () (p < 0.01, 95% CI = 9.408–14.470; p < 0.01, 95% CI = 8.025–13.200) and T helper cells () (p < 0.01, 95% CI = 6.433–10.390; p < 0.01, 95% CI = 5.902–9.937), elevated T suppressor cells () (p < 0.01, 95% CI = −10.730–−7.487; p < 0.01, 95% CI = −11.600–−8.283) and Tregs () (p < 0.01, 95% CI = −11.180–−8.079; p < 0.01, 95% CI = −11.600–−8.438), and decreased CD4+/CD8+ ratio () (p < 0.01, 95% CI = 0.679–0.900; p < 0.001, 95% CI = 0.687–0.912). Together, the above findings evidenced the abnormality of T lymphocyte subsets in peripheral blood of middle-advanced CC patients.
Figure 1. Changes in T lymphocyte subsets in peripheral blood of patients with middle-advanced CC. Flow cytometry was used to determine the levels of (A) total T cells (CD3+CD45+); (B) T helper cells (CD3+CD4+); (C) T suppressor cells (CD3+CD8+); (D) Tregs (CD4+CD25+CD127Dim) in healthy subjects and middle-advanced CC patients before treatment, and (E) CD4+/CD8+ ratio was calculated. Data were presented as mean ± standard deviation, and one-way ANOVA was used for comparisons among multiple groups, followed by Tukey’s test. *p < 0.05, **p < 0.01, ***p < 0.001.
Changes of T lymphocyte subsets in peripheral blood of middle-advanced CC patients treated with CCRT + Nim
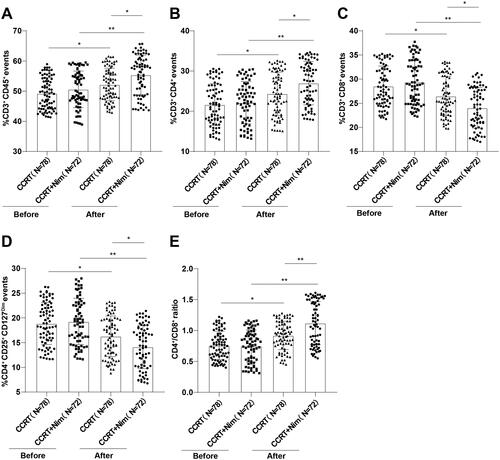
To further elucidate the precise effects of CCRT + Nim on T lymphocyte subsets, we subsequently determined the levels of T lymphocyte subsets in peripheral blood in patients with middle-advanced CC in the 4th week after treatment. Subsequent results demonstrated that compared to the levels detected prior to treatment, total T cells () (p < 0.05, 95% CI = −8.568–−3.652; p < 0.01, 95% CI = −7.287–−2.274), T helper cells () (p < 0.05, 95% CI = −4.902–−0.517; p < 0.01, 95% CI = −7.131–−2.567) and CD4+/CD8+ ratio () (p < 0.01, 95% CI = −0.272–−0.048; p < 0.01, 95% CI = −0.486–−0.253) were markedly enhanced at week 4 post-treatment in the CCRT group and CCRT + Nim group, and the CCRT + Nim group exhibited higher levels than the CCRT group (p < 0.05, 95% CI = −5.629–−0.712; p < 0.05, 95% CI = −4.867–−0.391; p < 0.01, 95% CI = −0.313–−0.085); T suppressor cells () (p < 0.05, 95% CI = 0.294–3.806; p < 0.01, 95% CI = 3.503–7.158) along with Tregs () (p < 0.05, 95% CI = 0.788–4.392; p < 0.01, 95% CI = 3.265–7.016) were both decreased in the CCRT group and CCRT + Nim group, and the CCRT + Nim group exhibited lower levels than the CCRT group (p < 0.05, 95% CI = 0.658–4.242; p < 0.05, 95% CI = 0.321–3.999). Altogether, the above findings indicated that CCRT or CCRT + Nim could improve the disorder of T lymphocyte subsets in peripheral blood of middle-advanced CC individuals, with CCRT + Nim exhibiting higher efficacy.
Figure 2. Changes in T lymphocyte subsets in peripheral blood of middle-advanced CC patients treated with CCRT + Nim. Flow cytometry was performed to determine the levels of (A) total T cells (CD3+CD45+); (B) T helper cells (CD3+CD4+); (C) T suppressor cells (CD3+CD8+); (D) Tregs (CD4+CD25+CD127Dim) at week 4 after treatment in middle-advanced CC patients, and (E) CD4+/CD8+ ratio was calculated. Data were exhibited as mean ± standard deviation, and one-way ANOVA was adopted for comparisons among multiple groups, followed by Tukey’s test. *p < 0.05, **p < 0.01.
Efficacy of CCRT + Nim in patients with middle-advanced CC
Furthermore, we evaluated the efficacy at the 4th-week post-treatment. In the CCRT group, 39 patients (50.00%) presented with CR, 18 patients (23.08%) presented with PR, 14 patients (17.95%) presented with SD, and 7 patients (8.97%) presented with PD, with an overall response rate of 73.08%. In the CCRT + Nim group, 42 patients (58.33%) presented with CR, 20 patients (27.78%) presented with PR, 8 patients (11.11%) presented with SD, and 2 patients (2.78%) presented with PD, with an overall response rate of 86.11%. The difference in the overall response rate was significant between the two groups (p = 0.049), and the CCRT + Nim group exhibited better short-term efficacy than the CCRT group ().
Table 2. Comparison of short-term efficacy between CCRT group and CCRT + Nim group.
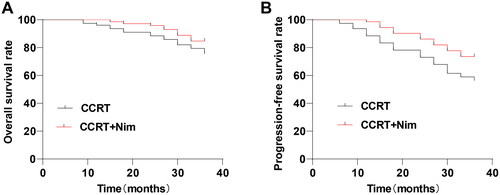
Thereafter, patients after treatment were followed up for 3 years to record 3-year OS and PFS. In the CCRT group, 19 patients died within 3 years, with an OS of 75.64% (19/78); 15 patients experienced PD, with a PFS of 56.41% (34/78). In the CCRT + Nim group, 11 patients died within 3 years, with an OS of 84.72% (11/72), and 8 patients experienced PD, with a PFS of 73.61% (19/72). The Kaplan–Meier survival curves (log-rank test) illustrated that there were no evident differences in OS between the two groups () (p = 0.153), while the CCRT + Nim group exhibited a higher PFS rate than the CCRT group () (p = 0.020, 95% CI = 1.107–3.330).
Figure 3. Kaplan–Meier survival curves for middle-advanced CC patients treated with CCRT + Nim. Differences in (A) OS and (B) PFS of middle-advanced CC patients in the CCRT group and CCRT group were analysed by Kaplan-Meier survival curves.
Correlation between T lymphocyte subsets in peripheral blood and OS/PFS in patients with middle-advanced CC
Lastly, we analysed the correlation between T lymphocyte subsets in peripheral blood at week 4 after treatment and OS/PFS in patients with middle-advanced CC by means of Pearson analysis. Subsequent results elicited () that the levels of total T cells, T helper cells, T suppressor cells, and Tregs after CCRT or CCRT + Nim treatment all showed no significant correlation with OS and PFS (all p > 0.05), while the CD4+/CD8+ ratio showed no evident correlation with OS (p = 0.093) but significant relevance to PFS (p < 0.001, r = −0.463, 95% CI = −0.579–−0.326).
Table 3. Correlation between T lymphocyte subsets and OS/PFS in patients with middle-advanced CC.
Discussion
CC represents highly-prevalent cancer in women, accounting for approximately 604,000 new cases, in addition to 342,000 deaths globally in 2020 (Sung et al. Citation2021). Current-day treatment modalities, such as CCRT have improved patients’ outcomes and reduced recurrence and death rates by about 30–50%, however, the vast majority of patients are in only partial remission or remission for merely a short period after treatment, with more than 35% of patients still presenting with tumours and experiencing recurrence and metastasis (W. Chen et al. Citation2019). Interestingly, an array of biologic agents targeting molecular pathways such as EGFR have garnered the attention of numerous researchers (Eskander & Tewari Citation2014). Indeed, nimotuzumab, an anti-EGFR monoclonal antibody, was recently indicated to exert anti-tumour activity primarily through anti-proliferation, anti-angiogenesis, and pro-apoptosis (Mazorra et al. Citation2018). Herein, the current study sought to explore the effect of nimotuzumab plus CCRT regime on patients with middle-advanced CC.
EGFR is inherently capable of regulating tumour cell proliferation, signal transduction, and resistance to chemotherapy, and surfaced as a crucial target for the treatment of CC (Gomes et al. Citation2021, Shi et al. Citation2022). Over-expression of EGFR has been previously documented in 70–90% of CC cases, and further closely-linked with recurrent CC, advanced stages, and poor prognosis (Schrevel et al. Citation2017, Liu et al. Citation2020). Nimotuzumab, a humanised monoclonal antibody, possesses the ability to target EGFR to hamper tumour progression, and its combination with CCRT in treating stage IIb-IIIb CC is associated with longer PFS and higher CR rates than individual CCRT, accompanied by no increase in the incidence of adverse events (W. Chen et al. Citation2019). Additionally, nimotuzumab alongside chemotherapy is not only well tolerated, but also contributes to disease stabilisation among 35% of CC patients, such that this effect can definitively translate into OS and PFS rates of 299 and 163 days, respectively (Cetina et al. Citation2015). In our study, the efficacy of the two therapy regimes (CCRT alone or nimotuzumab combined with CCRT) among patients with middle-advanced CC was evaluated at week 4 post-therapy. In much agreement with previous studies, our findings unearthed that CCRT + nimotuzumab exhibited better short-term efficacy than individual CCRT (CR: 58.33% vs 50.00%; PR: 27.78% vs 23.08%; SD: 11.11% vs 17.95%; PD: 2.78% vs 8.97%: overall response rate: 86.11% vs 73.08%). Additionally, we found that CCRT in combination with nimotuzumab produced similar 3-year OS (84.72% vs 75.64%, p = 0.153), in addition to an elevated 3-year PFS rate (73.61% vs 56.41%, p = 0.020) compared with individual CCRT. Collectively, the aforementioned findings and evidence underscore the promising application of a combination of CCRT and nimotuzumab in CC therapy.
T cells are well-known for their imperative role in CC pathogenesis as HPV employs a variety of mechanisms to evade host T-cell immune surveillance, thus contributing to persistent infection and subsequent onset of cancer (Chauhan & Bharadwaj Citation2018). Accumulating evidence also emphasised the breakdown of Th17/Treg balance in peripheral blood of CC patients, partly manifested as an elevated number of Tregs (Z. Chen et al. Citation2013). In addition, recent investigations have indicated the presence of more CD8+ cells in larger tumours or stage III diseases, and the CD4+/CD8+ ratio is lower with higher stages of CC (Das et al. Citation2018). Moreover, a decreased proportion of tumour-infiltrated CD4+ T cells is closely associated with lymph node metastasis and rapid tumour growth in CC individuals (Zhang et al. Citation2020). Intriguingly, radiotherapy can alter the functions and differentiation pathways of T cells, which in turn facilitates immune responses of T cells (C. Chen et al. Citation2021). What’s more, the study carried out by Teng et al. highlighted that nimotuzumab combined with CRT can effectively protect the immune function of CC patients, partly evidenced by increased Th1/Th2 levels and decreased Th17/Treg levels (Teng et al. Citation2023). Therefore, we determined the levels of T lymphocyte subsets before and after treatment. Subsequently, we learned that 4-week treatment with either of these two modalities could elevate the levels of total T cells, T helper cells, and CD4+/CD8+ ratio, as well as diminish T suppressor cells and Tregs in peripheral blood of middle-advanced CC patients, with the combination of CCRT + nimotuzumab exhibiting better effects in alleviating T cell imbalance than individual CCRT.
Furthermore, much evidence has come to light suggesting that the trends of different T lymphocyte subsets vary inconsistently (Chraa et al. Citation2019). Our study focussing on elucidating their change trends is carried out based on a specific context as follows. The cellular immune function of CC patients is lower than that of normal people, and the disturbance of T cell subsets is highly-correlated with the severity of the clinical CC stage, which is manifested by the abnormal levels of T lymphocyte subsets. More specifically, CD4+ T cells which represent the total T cells are obviously at a low expression level, while the CD8+ T cells are present at a high expression level, ultimately resulting in a reduction in CD4+/CD8+. Unlike our findings, a prior study documented a slight increase in CD8+ T cells during CCRT (J. Chen et al. Citation2021), which indicates that CCRT therapy may have a short-term negative impact on the peripheral T cell immune microenvironment. Positive CD4+ T cells have also been revealed to be decreased after CCRT, suggesting the fatigue of anti-tumour immune response after early CCRT (Li et al. Citation2021). In addition, recent studies have unveiled the inconsistent expression levels of CD8+ tumour-infiltrating lymphocytes (TILs) at different time points, which may be attributed to radiotherapy regimens (Hou et al. Citation2014, Assad et al. Citation2016, de Melo et al. Citation2016, Frenel et al. Citation2017).
It is also noteworthy that TILs are closely-associated with better clinical outcomes in CC (Shah et al. Citation2011), and can further predict survival outcomes in CC patients treated with CCRT (Ohno et al. Citation2020). However, our findings unveiled that the levels of total T cells, T helper cells, T suppressor cells, and Tregs in CC patients receiving CCRT or CCRT + nimotuzumab exhibited no evidence of correlation with OS and PFS. Of utmost interest, only the CD4+/CD8+ ratio was prominently related to PFS but not to the OS.
To conclude, findings uncovered in the current study highlighted that nimotuzumab combined with CCRT improved the abnormality of T lymphocyte subsets in peripheral blood of patients with middle-advanced CC, and the CD4+/CD8+ ratio after treatment was prominently correlated with PFS. However, there are a few limitations to our study, starting with a small sample size and a short follow-up period. In addition, we solely analysed the changes in T helper cells (CD3+CD4+), T suppressor cells (CD3+CD8+), and Tregs (CD4+CD25+CD127Dim), and failed to analyse other specific cells. Additionally, the time point of the immune status examination was single. In future studies, we shall strive to conduct a multi-centre study with an expanded sample size and further investigate the level changes in Th1, Th2, Th9, and Th17 cells, as well as the dynamic and long-term effects on the immune status. In particular, sexual dysfunction is common among CC survivors, and exerts a great burden on the long-term quality of life and sexual relationships (Valenti et al. Citation2017, Vizzielli et al. Citation2021). Surgery, chemotherapy, and radiotherapy possess the risk of serious damage and there is still a lack of specific assessment tools to evaluate sexual dysfunction in CC patients. Interventional studies are still at an exploratory stage, and the intervention effect needs to be further verified. Therefore, special attention is also warranted for the management of quality of life and sexual function in CC women after nimotuzumab combined with CCRT. Moreover, several lines of evidence support the possibility to employ specific biomarkers to identify early-stage CC. In fact, cancer biomarkers are not only effective for early diagnosis, they also have other application areas such as assessing and monitoring treatment to improve the diagnosis and treatment of CC (Valenti et al. Citation2017, Bizzarri et al. Citation2021). Accordingly, investigating the dynamic changes of relevant biomarkers after treatment with nimotuzumab combined with CCRT also provides a certain reference value for assessing efficacy. Furthermore, it is worth noting that the microbiota can also modulate the immune response and alter the physiological function of human body, thereby augmenting the risk of infection and tumour susceptibility. A better understanding of the microbiota may be key to personalised and specific management of cervical precancerous lesions, and also serve as a critical factor for achieving complete viral clearance in most infected populations (Cascardi et al. Citation2022). In addition, the application of anti-EGFR drugs may trigger cerebral ischaemic injury (Sacks et al. Citation2018). Therefore, it is prudent to carry out a multidisciplinary study to assess the changes in microflora and the impact on cerebral ischaemic injury for a comprehensive assessment of the efficacy of nimotuzumab in combination with CCRT.
Ethics approval
The current study was ratified by the Ethics Committee for Clinical Investigations of Affiliated Hospital of Chengde Medical College (Approval number: 20220207001), and all experimentation complied with the ethical principles of medical research in the Declaration of Helsinki.
Consent form
Signed informed consent was obtained from each participant prior to enrolment. Conform the Enhancing the QUAlity and Transparency Of health Research (EQUATOR) network guidelines.
Authors’ contributions
MA is the guarantor of integrity of the entire study and contributed to the study design, manuscript editing; YTH contributed to the study concepts, manuscript review; PYL contributed to the definition of intellectual content, literature research; XJL contributed to the clinical studies, data acquisition; DXS contributed to the experimental studies, manuscript preparation; SLX contributed to the data analysis, statistical analysis; All authors read and approved the final manuscript.
Supplemental Material
Download Zip (2.2 MB)Acknowledgements
Not applicable.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Assad, D. X., et al., 2016. Potential impact of mTOR inhibitors on cervical squamous cell carcinoma: a systematic review. Oncology Letters, 12 (5), 4107–4116.
- Bizzarri, N., et al., 2021. Peritoneal HPV-DNA test in cervical cancer (PIONEER study): a proof of concept. International Journal of Cancer, 148 (5), 1197–1207.
- Burmeister, C. A., et al., 2022. Cervical cancer therapies: current challenges and future perspectives. Tumour Virus Research, 13, 200238.
- Cascardi, E., et al., 2022. Association between cervical microbiota and HPV: could this be the key to complete cervical cancer eradication? Biology, 11 (8), 1114.
- Castle, P. E., Einstein, M. H. and Sahasrabuddhe, V. V., 2021. Cervical cancer prevention and control in women living with human immunodeficiency virus. CA Cancer Journal for Clinicians, 71 (6), 505–526.
- Cetina, L., et al., 2015. A pilot study of nimotuzumab plus single agent chemotherapy as second- or third-line treatment or more in patients with recurrent, persistent or metastatic cervical cancer. Cancer Biology & Therapy, 16, 684–689.
- Chauhan, S. R. and Bharadwaj, M., 2018. Gearing up T-cell immunotherapy in cervical cancer. Current Problems in Cancer, 42, 175–188.
- Chen, C., Liu, Y. and Cui, B., 2021. Effect of radiotherapy on T cell and PD-1/PD-L1 blocking therapy in tumor microenvironment. Human Vaccines & Immunotherapeutics, 17 (6), 1555–1567.
- Chen, J., et al., 2021. Heterogeneity of IFN-mediated responses and tumor immunogenicity in patients with cervical cancer receiving concurrent chemoradiotherapy. Clinical Cancer Research, 27 (14), 3990–4002.
- Chen, T., et al., 2020. T-lymphocyte subsets and Th1/Th2 cytokines in convalescent patients with Epstein-Barr virus-associated aplastic anemia. Hematology, 25 (1), 11–16.
- Chen, W., et al., 2019. Clinical study of nimotuzumab combined with concurrent radiochemotherapy for treatment of locally advanced cervical cancer. Cancer Management and Research, 11, 8157–8165.
- Chen, Z., et al., 2013. The Th17/Treg balance and the expression of related cytokines in Uygur cervical cancer patients. Diagnostic Pathology, 8, 61.
- Chraa, D., et al., 2019. T lymphocyte subsets in cancer immunity: Friends or foes. Journal of Leukocyte Biology, 105 (2), 243–255.
- Cohen, P. A., et al., 2019. Cervical cancer. Lancet, 393, 169–182.
- Crowley, F. J., O'Cearbhaill, R. E. and Collins, D. C., 2021. Exploiting somatic alterations as therapeutic targets in advanced and metastatic cervical cancer. Cancer Treatment Reviews, 98, 102225.
- Das, D., et al., 2018. An altered ratio of CD4+ And CD8+ T lymphocytes in cervical cancer tissues and peripheral blood – a prognostic clue? Asian Pacific Journal of Cancer Prevention, 19 (2), 471–478.
- de Melo, A. C., et al., 2016. A phase I study of mTOR inhibitor everolimus in association with cisplatin and radiotherapy for the treatment of locally advanced cervix cancer: PHOENIX I. Cancer Chemotherapy and Pharmacology, 78 (1), 101–109.
- Eskander, R. N. and Tewari, K. S., 2014. Beyond angiogenesis blockade: targeted therapy for advanced cervical cancer. Journal of Gynecologic Oncology, 25 (3), 249–259.
- Frenel, J. S., et al., 2017. Safety and efficacy of pembrolizumab in advanced, programmed death ligand 1-positive cervical cancer: results from the phase Ib KEYNOTE-028 trial. Journal of Clinical Oncology, 35 (36), 4035–4041.
- Gomes, F. G., et al., 2021. Epidermal growth factor receptor regulates fibrinolytic pathway elements in cervical cancer: functional and prognostic implications. Brazilian Journal of Medical and Biological Research, 54 (6), e10754.
- Gopu, P., et al., 2021. Updates on systemic therapy for cervical cancer. Indian Journal of Medical Research, 154 (2), 293–302.
- Hou, M. M., et al., 2014. Targeted PI3K/AKT/mTOR therapy for metastatic carcinomas of the cervix: a phase I clinical experience. Oncotarget, 5 (22), 11168–11179.
- Li, R., et al., 2021. The dynamic alternation of local and systemic tumor immune microenvironment during concurrent chemoradiotherapy of cervical cancer: a prospective clinical trial. International Journal of Radiation Oncology Biology Physics, 110 (5), 1432–1441.
- Liu, Y., An, Q. and Zhao, X., 2020. A pan-HER-targeted approach for recurrent or late-stage cervical cancer therapy: mechanisms, recent advances, and clinical prospects. European Review for Medical and Pharmacological Sciences, 24 (8), 4123–4131.
- Matsuzaki, S., et al., 2020. Management of stage IIB cervical cancer: an overview of the current evidence. Current Oncology Reports, 22 (3), 28.
- Mazorra, Z., et al., 2018. Nimotuzumab: beyond the EGFR signaling cascade inhibition. Seminars in Oncology, 45 (1–2), 18–26.
- Muthusami, S., et al., 2022. A review on the role of epidermal growth factor signaling in the development, progression and treatment of cervical cancer. International Journal of Biological Macromolecules, 194, 179–187.
- Naga Ch, P., et al., 2018. The management of locally advanced cervical cancer. Current Opinion in Oncology, 30 (5), 323–329.
- Ohno, A., et al., 2020. Tumor-infiltrating lymphocytes predict survival outcomes in patients with cervical cancer treated with concurrent chemoradiotherapy. Gynecologic Oncology, 159 (2), 329–334.
- Okunade, K. S., 2020. Human papillomavirus and cervical cancer. Journal of Obstetrics and Gynaecology, 40 (5), 602–608.
- Pimple, S. A. and Mishra, G. A., 2019. Global strategies for cervical cancer prevention and screening. Minerva Ginecologica, 71 (4), 313–320.
- Sacks, D., et al., 2018. Multisociety consensus quality improvement revised consensus statement for endovascular therapy of acute ischemic stroke. International Journal of Stroke, 13 (6), 612–632.
- Schrevel, M., et al., 2017. Autocrine expression of the epidermal growth factor receptor ligand heparin-binding EGF-like growth factor in cervical cancer. International Journal of Oncology, 50 (6), 1947–1954.
- Shah, W., et al., 2011. A reversed CD4/CD8 ratio of tumor-infiltrating lymphocytes and a high percentage of CD4(+)FOXP3(+) regulatory T cells are significantly associated with clinical outcome in squamous cell carcinoma of the cervix. Cellular & Molecular Immunology, 8 (1), 59–66.
- Shi, K., et al., 2022. Emerging strategies to overcome resistance to third-generation EGFR inhibitors. Journal of Hematology & Oncology, 15 (1) 94.
- Sung, H., et al., 2021. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer Journal for Clinicians, 71, 209–249.
- Teng, F., et al., 2023. Changes of T lymphocyte subsets in peripheral blood of patients with intermediate and advanced cervical cancer before and after nimotuzumab combined with chemoradiotherapy. International Archives of Allergy and Immunology, 184 (1), 85–97.
- Valenti, G., et al., 2017. Tumor markers of uterine cervical cancer: a new scenario to guide surgical practice? Updates in Surgery, 69 (4), 441–449.
- Vizzielli, G., et al., 2021. Is a vaginectomy enough or is a pelvic exenteration always required for surgical treatment of recurrent cervical cancer? A propensity-matched study. Annals of Surgical Oncology, 28 (6), 3281–3290.
- Zhang, L., et al., 2020. A review of the research progress in T-lymphocyte immunity and cervical cancer. Translational Cancer Research, 9, 2026–2036.
- Zhao, Y., Shao, Q. and Peng, G., 2020. Exhaustion and senescence: two crucial dysfunctional states of T cells in the tumor microenvironment. Cellular & Molecular Immunology, 17 (1), 27–35.