

Abstract
This study evaluated whether psychological stress increases the incidence of ovarian cancer. A literature search of the electronic databases PubMed and Web of Science from the date of inception to August 2022 was undertaken. Studies with data on psychosocial factors associated with ovarian cancer incidence were included in this study. A random-effect model meta-analysis was undertaken to estimate these data. We used subgroup analysis to adjust for heterogeneity. A total of 4 articles, 10 sets of data, 8 cohort studies, and 2 case–control studies from 682 records were included in this review. Meta-analyses of the included cohort study subgroups suggested that psychological factors increase the risk of ovarian cancer (effect size = 1.37, 95% CI: 1.20–1.53); the subgroup of case–control studies suggested that psychological factors did not increase ovarian cancer risk (effect size = 0.84, 95% CI: 0.70–0.98). These findings indicate that psychological stress is a possible new risk factor for ovarian cancer.
Prospero registration number: CRD42022357983
What is already known on this subject? Psychological stress has been shown to increase the risk of many diseases. The relationship between psychological stress and the incidence of ovarian cancer has not been confirmed.
What do the results of this study add? The effect of psychological stress on the risk of ovarian cancer was estimated using meta-analysis as an overall ratio.
What are the implications of these findings for clinical practice and/or further research? Relaxing psychological stress and appropriate psychotherapy in clinical settings can help reduce the risk of ovarian cancer.
IMPACT STATEMENT
1. Introduction
Whether psychosocial stress is a risk factor in cancer aetiology has attracted attention. A recent meta-analysis reported that psychosocial factors are associated with a higher incidence of lung cancer in patients with breast, lung, head and neck, hepatobiliary, and lymphoid or haematopoietic cancers (Chida et al. Citation2008). This study reported a 6% increased risk of cancer associated with psychosocial stress (Chida et al. Citation2008, Poole et al. Citation2016), but the study did not evaluate ovarian cancer. Ovarian cancer is the twentieth most common cancer and the fourteenth leading cause of cancer death worldwide (Sung et al. Citation2021). Current treatment modalities, including lymph node dissection and chemotherapy, do not ensure a good prognosis for patients with ovarian cancer, and it remains important to better understand the aetiology of ovarian cancer to reduce its incidence and improve survival (Panici et al. Citation2020, Musella et al. Citation2017). A review detailing current epidemiologic findings identified several ovarian cancer risk factors, including a family history of ovarian cancer, nulligravity, elevated sex hormone levels, endometriosis, obesity and extremes in latitude (Hunn and Rodriguez Citation2012). Psychosocial factors were not included. Few known risk factors are easily modifiable, but psychosocial factors may be an intervenable risk factor.
Psychosocial factors affecting cancer incidence may differ among different cancer types (Chida et al. Citation2008). Evidence-based medical research is critical to explore the impact of psychological factors on the incidence and other related properties of specific cancer subtypes.
Over the past 7 years, a series of studies have investigated associations between psychosocial factors and ovarian cancer development. However, these studies have produced disparate findings (Huang et al. Citation2015, Idahl et al. Citation2018, Roberts and Huang, Citation2019, Trudel-Fitzgerald et al. Citation2019). The heterogeneity of the study results may be due to experimental design or other confounding factors. No study has used meta-analytic techniques to quantify the extent to which psychosocial factors affect ovarian cancer.
According to the guidance of Prisma, this study standardised the various steps of meta-analysis, hoping to give peers and readers a quantitative overview of whether psychological stress can increase the risk of ovarian cancer and analyse the reasons for the disparate study results.
2. Method
2.1. Search strategy
Due to differences in the terms used to describe psychological factors, a broad range of search terms was used. The electronic databases of PubMed and Web of Science were searched from inception up to August 2022 using the following keywords: (ovarian cancer) AND (“anxiety” OR “coping” OR “depress*” OR “personality” OR “psych*” OR “social support” OR “stress”) AND (“longitudinal” OR “prospective”) (Chida et al. Citation2008). presents the process and results of the screening studies.
Figure 1. Search strategy and flow chart of the included studies.
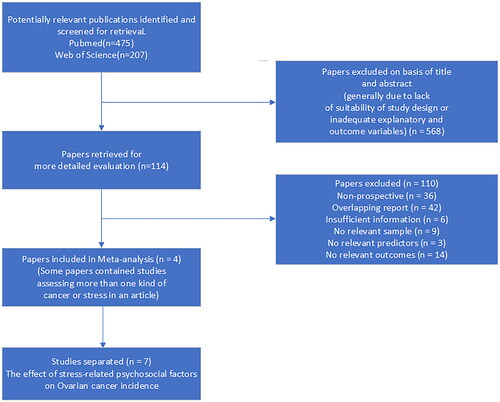
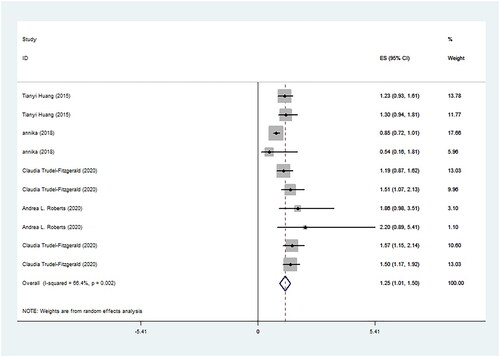
Figure 2. Results of meta-analyses for enrolled studies.
2.2. Inclusion and exclusion criteria
For inclusion, studies were required to (1) be in the English language; (2) report at least one psychological factor exposure; (3) report effect size (RR, HR or OR) and 95% confidence interval; and (4) include an exposure group and control group. Studies were excluded if (1) they did not present quantitative data; (2) they did not present outcomes relevant to ovarian cancer; and (3) the study population included only special populations (e.g. forensic/prisoner or veteran/military).
2.3. Data extraction
Extraction of study data was undertaken independently by a member of the research team and double-checked by a second reviewer; all disagreements were resolved by consensus through discussion with the third author. Extraction information included the study design, characteristics of the study population (i.e. sample size and follow-up period), the effect size of comparability between the stress group and control group, study measures and type of psychology factor. When analyses involved dividing the samples into three or more psychologic factor levels, we extracted the hazard ratio [HR] or odds ratio [OR] that compared the highest with the lowest (reference group) psychology group. The effect sizes included in this study were obtained after adjusting for confounding factors in the original study, and this study carefully considered the comprehensiveness of the original study by adjusting for confounding factors.
2.4. Quality assessment and publication bias
Studies enrolled in this meta-analysis included cohort studies and case-control studies, and the OTTAWA QUALITY ASSESSMENT SCALE was used to assess the quality of the included studies (Zeng et al. Citation2015). The quality assessment and study search were performed independently by three reviewers (Shuo Geng, Xiaoyu Zhu, and Yewu Sun). Differences in opinion were settled by consensus. The Begg method was used to test for publication bias, and p < 0.05 was considered statistically significant (Begg and Mazumdar Citation1994, Lin and Chu, Citation2018).
2.5. Data synthesis and analysis
Meta-analyses of effect size (HR and OR) were performed using STATA version 12 via the Metan command (Taylor et al. Citation2018). A random-effects model was chosen in advance due to expected differences between studies with respect to psychological factors, measurement of psychological problems and differences in follow-up time. Inconsistency was estimated by calculating the I2 statistic, which describes the proportion of total variance across studies that is due to heterogeneity rather than sampling error (Higgins and Thompson Citation2002, Higgins et al. Citation2003, Taylor et al. Citation2018). An I2 >75% is considered a ‘high’ degree of inconsistency (Higgins et al. Citation2003, Taylor et al. Citation2018). According to the type of study design included, cohort studies and case–control studies were divided into two subgroups to calculate the total effect size separately.
The type of psychological factor and years of follow-up may affect the heterogeneity of the study results. If subgroup analysis failed to clearly explain the source of heterogeneity, the meta-regression command in STATA version 12 was used to analyse the effect of the psychological factor type and follow-up on the results.
3. Result
3.1. Study characteristics
Four studies containing k = 9 independent samples were included in the meta-analysis. A summary of the study characteristics is presented in . All studies employed a longitudinal design with the exception of one case-control study. The included studies addressed the following psychological factors: Berkman-Syme Social Network Index (n = 2), marital status (n = 2), posttraumatic stress disorder (n = 2), depression (n = 2), social support availability of social integration (n = 1), and social support availability of attachment (n = 1). The Berkman-Syme Social Network Index has been widely used in prior research. Marital status was determined by asking if patients were married/partnered, separated/divorced, or widowed. Posttraumatic stress disorder was judged by the number of symbols. Depression was measured by the 5-item Mental Health Index (MHI-5) scale. Social support availability of social integration and social support availability of attachment were measured by SS13.
Table 1. Characteristics of the enrolled studies (n = 10).
3.2. Quality asessment and publication bias
The quality assessment is presented in . Overall, the quality of the enrolled studies was high with respect to the data that were the focus of this review. The included studies are of high quality with respect to case definition, representativeness, selection and definition of controls, comparability of cohorts, selection of exposure, consistent methods of ascertainment, nonresponse rate and explanation. A less obvious problem is that several studies use scales of questionable validity to judge subjects’ psychological distress. Begg’s rank test indicated no significant publication bias (p = 0.788).
Table 2. Quality assessment of cohort and case-control studies included in the meta-analysis using the NOS Quality Assessment Scale.
3.3. Meta-analysis
In initial meta-analyses, psychological stress increased the risk of ovarian cancer overall (effect size = 1.25 95% CI 1.01–1.50). Because the lower confidence interval was close to 1, the results must be interpreted with caution. Inconsistency across the studies, as judged by the I2 statistic, was potentially high (I2 = 66.4%). The use of a random-effects model was adequate for this analysis. In light of the high level of inconsistency, we recommend that readers focus not on the overall effect size but instead on the range provided by the 95% confidence intervals (Taylor et al. Citation2018) ().
3.4. Moderators of effect size
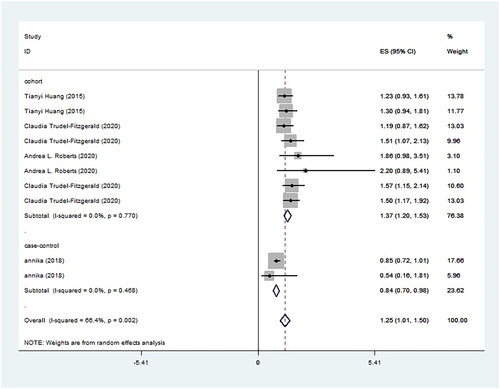
presents forest graphs as a subgroup of the study design (cohort and case-control). In the cohort study subgroup, psychological stress significantly increased the risk of ovarian cancer (effect size = 1.37 95% CI 1.20–1.53). In the case-control subgroup, psychological stress did not appear to increase the risk of ovarian cancer and may exhibit a protective factor for ovarian cancer (effect size = 0.84 95% CI 0.70–0.98). Inconsistency as judged by the I2 statistic in the two subgroups was 0. This suggests that the heterogeneity stems from differences in results due to study design. There is no clear time series in case-control studies, which may lead to misinterpretation because patients with ovarian cancer are more likely to have long-term psychological problems that have not been previously diagnosed.
Figure 3. Subgroup classification criteria by study design and meta-analysis.
4. Discussion
This review assessed recent studies of psychological factors and ovarian cancer risk, including a total of 10 sets of data from four articles. We determined that overall, psychological factors increase the risk of ovarian cancer, with the exception of in case-control studies. Stress may promote high-risk behaviours, such as smoking, poor diet, lack of exercise, obesity, excessive alcohol consumption, poor sleep and lower treatment adherence (van Tuijl et al. Citation2021). Additionally, psychological factors may impact biological mechanisms, which in turn promote malignant growth. Psycho-social processes initiate a cascade of information-processing pathways in the central nervous system and periphery, thereby impacting hormonal secretion (, Glaser and Kiecolt-Glaser, Citation2005, Charmandari et al. Citation2005, Antoni et al. 2006). These changing hormones could modulate the activity of multiple components of the tumour microenvironment (Antoni et al. Citation2006, Chida et al. Citation2008). According to the enrolled cohort study data, the researchers attempted to avoid the influence of confounding factors such as behavioural factors other than psychology and adjusted for smoking, physical activity, nutrition, and other potential confounders. The results nonetheless suggest a higher risk of ovarian cancer in people with psychological distress, which we cautiously interpret as evidence that psychological stress increases the risk of ovarian cancer.
The case-control studies included in this meta-analysis suggest that psychological factors may not be a risk factor for ovarian cancer. Self-perceived social support on the day of participation does not necessarily reflect the true availability of social support, according to Annika Idahl (Idahl et al. Citation2018). High scores on the AVSI and AVAT may not indicate low stress and well-being (Idahl et al. Citation2018). The results differ from cohort studies due the social support evaluation criteria.
A primary limitation is that this meta-analysis is based on the literature, which is not aimed at a specific psychological problem. For example, the included studies assessed social support, depression, and PTSD. However, only one article is available for each psychological problem, which is potentially misleading. The present study did not record the original effect size of unadjusted confounders and conducted a meta-analysis directly, which may affect the accuracy of the results secondary to different confounders with each article. The strength of this study is that it is the first meta-analysis to specifically analyse whether psychological factors increase the incidence of ovarian cancer through the integration of current prospective studies in this field.
Currently, there is a lack of replicated cohort studies for a specific psychological problem, potentially leading to bias. In addition, the specific mechanism by which psychological factors influence the incidence of ovarian cancer is unknown. Psychological stress is believed to impair the immune response and increase the risk of cancer (Reiche et al. Citation2004). However, not ever cancer increases in incidence due to psychological stress (Chida et al. Citation2008, van Tuijl et al. Citation2021). Psychosocial factors contribute to cancer genesis as well as progression; conversely, cancer leads to many psychosocial challenges (Lang-Rollin and Berberich Citation2018). Extensive oncological surgery for ovarian cancer can negatively impact mental health, despite prolonging survival (Gueli Alletti et al. Citation2016, Dessole et al. Citation2018). The damage to mental health from gynaecologic cancer treatment may be due to the simultaneous loss of fertility in women of childbearing age (Vitale et al. Citation2017, Vitale et al. Citation2018). The emerging discipline of psycho-oncology is working towards a solution to this problem. Increased attention to the mental health of gynaecologic cancer patients is important. This study provides new evidence of risk factors for ovarian cancer, suggesting that more attention should be given to mental health to reduce the risk of cancer. The specific impact of various psychological problems on ovarian cancer specifically and on cancer more broadly requires further in-depth research. Future research on this topic may be directed at whether early psychological counselling can reduce the incidence of gynaecologic cancers and whether psychological counselling can improve the prognosis or mental health of gynaecologic cancer survivors.
Conclusion
Psychological stress increases the risk of ovarian cancer, and this is the first meta-analysis to assess the impact of psychological stress on ovarian cancer incidence.
Author contributions
All authors contributed to the study's conception and design. Material preparation, data collection and analysis were performed by Shuo Geng, Xiaoyu Zhu and Yadi Wang. Expertise in psychology was provided by Xu Zhang. Statistical technical support was provided by Yingchen Wang. The first draft of the manuscript was written by Shuo Geng, and all authors commented on previous versions of the manuscript. Manuscript organisation was performed by Yingchen Wang. All authors read and approved the final manuscript.
Declarations
This manuscript was written according to the meta-analysis writing guidelines PRISMA.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Antoni, M. H., et al., 2006. The influence of bio-behavioural factors on tumour biology: pathways and mechanisms. Nature Reviews. Cancer, 6 (3), 240–248.
- Begg, C. B. and Mazumdar, M., 1994. Operating characteristics of a rank correlation test for publication bias. Biometrics, 50 (4), 1088–1101.
- Benedetti Panici, P., et al., 2020. Lymphadenectomy in Ovarian Cancer: Is It Still Justified? Current Oncology Reports, 22 (3), 22.
- Charmandari, E., Tsigos, C. and Chrousos, G., 2005. Endocrinology of the stress response. Annual Review of Physiology, 67, 259–284.
- Chida, Y., et al., 2008. Do stress-related psychosocial factors contribute to cancer incidence and survival? Nature Clinical Practice. Oncology, 5 (8), 466–475.
- Dessole, M., et al., 2018. Quality of life in women after pelvic exenteration for gynecological malignancies: a multicentric study. International Journal of Gynecological Cancer, 28 (2), 267–273.
- Glaser, R. and Kiecolt-Glaser, J. K., 2005. Stress-induced immune dysfunction: implications for health. Nature Reviews. Immunology, 5 (3), 243–251.
- Gueli Alletti, S., et al., 2016. Minimally invasive interval debulking surgery in ovarian neoplasm (MISSION trial-NCT02324595): a feasibility study. American Journal of Obstetrics and Gynecology, 214 (4), 503.e1-503–e6.
- Higgins, J. P. T. and Thompson, S. G., 2002. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21 (11), 1539–1558.
- Higgins, J. P. T., et al., 2003. Measuring inconsistency in meta-analyses. BMJ (Clinical Research ed.), 327 (7414), 557–560.
- Huang, T., et al., 2015. Depression and risk of epithelial ovarian cancer: Results from two large prospective cohort studies. Gynecologic Oncology, 139 (3), 481–486.
- Hunn, J. and Rodriguez, G. C., 2012. Ovarian cancer: etiology, risk factors, and epidemiology. Clinical Obstetrics and Gynecology, 55 (1), 3–23.
- Idahl, A., Hermansson, A. and Lalos, A., 2018. Social support and ovarian cancer incidence - A Swedish prospective population-based study. Gynecologic Oncology, 149 (2), 324–328.
- Lang-Rollin, I. and Berberich, G., 2018. Psycho-oncology. Dialogues in Clinical Neuroscience, 20 (1), 13–22.
- Lin, L. and Chu, H., 2018. Quantifying publication bias in meta-analysis. Biometrics, 74 (3), 785–794.
- Musella, A., et al., 2017. Bevacizumab in ovarian cancer: state of the art and unanswered questions. Chemotherapy, 62 (2), 111–120.
- Poole, E. M., et al. 2016. A prospective study of phobic anxiety, risk of ovarian cancer, and survival among patients. Cancer Causes & Control : CCC, 27 (5), 661–668.
- Reiche, E. M., Nunes, S. O. and Morimoto, H. K., 2004. Stress, depression, the immune system, and cancer. Lancet Oncology., 5 (10), 617–625.
- Roberts, A. L. and Huang, T., 2019. Posttraumatic stress disorder is associated with increased risk of ovarian cancer: a prospective and retrospective longitudinal cohort study. Cancer Research, 79 (19), 5113–5120.
- Sung, H., et al. 2021. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: a Cancer Journal for Clinicians, 71 (3), 209–249.
- Taylor, P. J., et al. 2018. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. Journal of Affective Disorders, 227, 759–769.
- Trudel-Fitzgerald, C., et al. 2019. Social Integration, Marital Status, and Ovarian Cancer Risk: A 20-Year Prospective Cohort Study. Psychosomatic Medicine, 81 (9), 833–840.
- VAN Tuijl, L. A., et al. 2021. Psychosocial factors and cancer incidence (PSY-CA): Protocol for individual participant data meta-analyses. Brain and Behavior, 11 (10), e2340.
- Vitale, S. G., et al. 2018. Fertility preservation in women with gynaecologic cancer: the impact on quality of life and psychological well-being. Human Fertility (Cambridge, England), 21 (1), 35–38.
- Vitale, S. G., et al. 2017. The Importance of Fertility Preservation Counseling in Patients with Gynecologic Cancer. J Reprod Infertil, 18, 261–263.
- Zeng, X., et al. 2015. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. Journal of Evidence-Based Medicine, 8 (1), 2–10.