

Abstract
This was a retrospective study that evaluated a total of 280 patients who underwent surgery for complete removal of endometriosis to develop and validate the predictive model for stage IV endometriosis. The differences between stage I-III and stage IV endometriosis were performed by logistic regression. A model for the prediction of stage IV endometriosis was constructed, which was subsequently validated. The independent variables were visual analogue scale (VAS)≥4 [3.855, 95% confidence interval (CI): 1.675–8.871, p = 0.002], painful nodularity on uterosacral ligaments (13.954, 95% CI: 1.658–117.423, p = 0.015), and bilateral endometriosis (5.933, 95% CI: 1.931–18.225, p = 0.002). The AUC of the model was 0.777, with a sensitivity of 71.9% and specificity of 76.3% for stage IV endometriosis. Therefore, a complete collection of patient information prior to surgery, asking about pain and VAS scores, careful completion of pelvic examinations, and application of imaging techniques are conducive to better diagnosis and prediction of advanced endometriosis.
What is already known on this subject? Endometriosis, a chronic disease causing pain and infertility, is characterised by endometrial-like tissue outside the uterine cavity, which is often treated via surgery at present. Considering the risks of surgery, it is necessary to identify patients with stage IV endometriosis through non-invasive predictive models for adequate preparation for surgery. However, there is no reliable non-invasive predictive model now, despite utilisation of patient medical history, symptoms especially pain-related ones, pelvic examinations, laboratory examinations, and images in the preoperative diagnosis of endometriosis in the clinic.
What do the results of this study add? A model developed based on three simple, accessible and non-invasive indicators displays good performance in predicting stage IV endometriosis.
What are the implications of these findings for clinical practice and/or further research? It is conducive to diagnosing and predicting advanced endometriosis before surgery, so as to reduce the difficulty and improve the safety of surgery.
IMPACT STATEMENT
Introduction
As a chronic disease characterised by endometrial-like tissue outside the uterine cavity, endometriosis causes pain and infertility and severely affects the quality of life of patients, with a prevalence rate of about 10% (Shafrir et al. Citation2018).
The manifestations of endometriosis are peritoneal endometriosis, ovarian endometrioma (OE), and deep infiltrating endometriosis (DIE). The staging system applied is a revised American Fertility Society (r-AFS) classification system designed by the American Society for Reproductive Medicine (ASRM Citation1997), and endometriosis is classified into four stages: I (minimal), II (mild), III (moderate), or IV (severe) (revised-ASRM classification of endometriosis 1996).
Currently, endometriosis is usually treated through surgery. Patients with stage IV endometriosis may have more pelvic adhesions and extensive lesions, making surgery more difficult. Moreover, for patients with ovarian endometriosis, surgery may result in reduced ovarian reserve (Kasaven et al. Citation2022). The development of non-invasive predictive models for identification of patients with stage IV endometriosis before surgery can help to adequately prepare for surgery, and even guide the preoperative use of gonadotropin-releasing hormone (GnRH) agonists to reduce pelvic congestion, narrow lesions, and reduce the difficulty and improve the safety of surgery.
To date, there is no reliable non-invasive predictive model for preoperative prediction of stage IV endometriosis. Despite many efforts, including many studies about predicting rather than staging endometriosis, no consensus has been reached on the best predictive models for endometriosis due to the diverse study population, different diagnostic criteria, and various predictive factors (Peterson et al. Citation2013, Agarwal et al. Citation2019). Conroy’s studies attempted to find predictors for endometriosis severity in a cohort of women with chronic pelvic pain (CPP) and showed that the only predictor is increasing age (Conroy et al. Citation2021). Guo et al. developed two nomograms to predict any-stage and stage III–IV endometriosis in infertile women and advised using imaging examinations for better diagnosis and prediction of endometriosis (Guo et al. Citation2020). Therefore, it is urgent to establish a preoperative model to predict stage IV endometriosis.
Methods
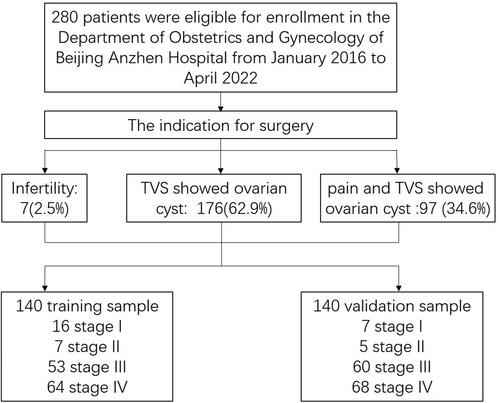
This was a single centre retrospective study in which an assessment was made on a total of 280 patients undergoing surgery for complete removal of endometriosis at the Department of Obstetrics and Gynaecology of Beijing Anzhen Hospital affiliated to Capital Medical University from January 2016 to April 2022. The inclusion criteria were set as follows: patients with endometriosis who needed surgical treatment for various reasons and were definitely diagnosed with endometriosis by postoperative pathology. The indications for surgery were infertility [7 patients (2.5%)], ovarian cysts and highly-suspected endometriosis according to transvaginal ultrasonography (TVS) [176 patients (62.9%)], and pain and ovarian cysts on TVS images [97 patients (34.6%)]. Patients who had pelvic pain and normal TVS findings before surgery but had endometriosis identified at the time of surgery were excluded from this study as such cases are rare.
The exclusion criteria involved patients with a history of endometriosis based on surgical diagnosis, but lack of histological confirmation of endometriosis or those complicated with adenomyosis, hysteromyoma, gynecological malignant tumour, benign ovarian tumour, or pelvic inflammatory disease. None of them received preoperative medication such as GnRH. shows the patient selection flowchart.
Figure 1. Flow chart of the patients included.
All patients underwent a comprehensive preoperative examination, including medical history collection, pelvic examinations, laboratory examinations, and TVS. Endometriosis was diagnosed based on visual evidence under laparoscopy and histological confirmation. Endometriosis was scored and classified into four stages according to the revised ASRM classification. All the operations were completed by three doctors (Zhao-Liang Bao, Jia Kong, and Wei Wei) and their assistants with objective scoring and good quality control.
Clinical data were recorded for each patient, including age at the first visit, previous pregnancies (gravidity and parity), and chief complaint. Pain symptoms included dysmenorrhoea, dyschezia, dyspareunia, and non-cyclic pelvic, or abdominal pain. A visual analogue scale (VAS) was employed to measure pain intensity (from 0 = no pain to 10 = unbearable pain). All patients received pelvic examinations, and fixed uterine (yes/no), fixed ovarian cyst (yes/no), uterosacral ligament nodule with tenderness (yes/no), and rectovaginal septum nodule with tenderness (yes/no) were recorded. The examinations were conducted by two or more doctors at the same level (chief physician or deputy chief physician) together to determine the final result to minimise bias. Carbohydrate antigen 125 (CA125) and hypersensitive C-reactive protein (hsCRP), two proteins commonly used as biomarkers to predict recurrence and assess treatment efficacy, respectively (Chen et al. Citation2021), were measured in blood samples, and their levels revealed the severity of inflammation in patients with endometriosis (Kaya Sezginer et al. Citation2022). The size of lesions was measured by TVS, and the heterogeneity (unilateral/bilateral) and multiplicity (single/multiple) of all lesions were recorded and counted.
A training sample of 140 patients receiving surgery for complete removal of endometriosis from January 2016 to December 2018 was set to develop a clinical predictive model, and 140 patients undergoing surgery for complete removal of endometriosis from January 2019 to April 2022 were set as the validation sample. The baseline characteristics of patients were first compared between training and validation samples. Then, a comparison was made on baseline characteristics of patients with stages I-III and IV endometriosis within the training sample. Next, multivariable logistic regression analysis was conducted to select the best combination of variables included in the final multiple models, which was independently associated with the diagnosis of stage IV endometriosis. Variable selection was completed by a reverse stepwise procedure. The goodness-of-fit of models was assessed using the Hosmer–Lemeshow test. The discriminative power of the resulting multiple logistic model outcome was visualised by a receiver operating characteristics curve (ROC) and assessed by area under the ROC (AUC).
Descriptive analyses were performed using frequencies and percentages for qualitative variables and mean ± standard deviations (SD) for quantitative variables. Categorical characteristics were compared using Pearson’s correlation coefficient (χ2 test), and quantitative variables were compared using the Student’s t-test. p < 0.05 was considered statistically significant. The statistical analyses were conducted using SPSS 25.0.0.1 for Windows (SPSS, Chicago, IL, USA).
This study was approved by the Ethics Committee of the Beijing Anzhen Hospital affiliated with Capital Medical University (2022061X), and informed consent was obtained from all participants enrolled in this study. This study was registered with the Chinese Clinical Trial Registry (Registration number: ChiCTR2200058414).
Results
Baseline characteristics
The training sample consisted of 140 selected patients, including 16 cases of stage I endometriosis, 7 cases of stage II endometriosis, 53 cases of stage III endometriosis, and 64 cases of stage IV endometriosis. The validation sample included 140 selected patients, among which 7 had stage I endometriosis, 5 had stage II endometriosis, 60 had stage III endometriosis, and 68 had stage IV endometriosis. Patient characteristics are summarised in , showing no significant difference between the two samples.
Table 1. Clinical characteristics of training and validation samples.
Predictors of stage IV endometriosis
The baseline characteristics in the training sample are summarised in . No significant differences were found in age, sterility, previous pregnancy, CA125, and hsCRP between patients with stage I-III endometriosis and those with IV endometriosis. The following eight variables were significantly different between patients with stage I-III endometriosis and those with IV endometriosis: VAS ≥ 4 (p = 0.000), fixed uterine (p = 0.001), fixed ovarian cyst (p = 0.000), uterosacral ligament nodule with tenderness (p = 0.000), rectovaginal septum nodule with tenderness (p = 0.003), bilateral endometriosis (p = 0.000), the sum of sizes of endometriosis (p = 0.002), and indication for surgery (p = 0.002).
Table 2. Clinical characteristics of training samples.
These eight variables were included in the model, and a forward stepwise selection procedure was performed. According to the estimation using the odds ratio (OR), VAS ≥ 4 (3.855, 95% CI: 1.675–8.871, p = 0.002), painful nodularity on uterosacral ligaments (13.954, 95% CI: 1.658–117.423, p = 0.015), and bilateral endometriosis (5.933, 95% CI: 1.931–18.225, p = 0.002) were significantly associated with stage IV endometriosis. The result of the multivariate logistic regression analysis of the training sample is shown in .
Table 3. Multivariate logistic regression analysis of training sample.
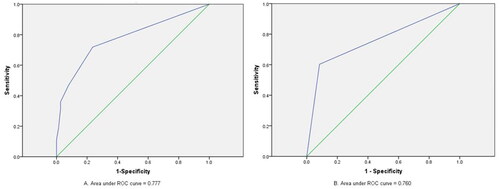
In the training sample, the model had an AUC of 0.777, a sensitivity of 71.9%, a specificity of 76.3%, and a correct classification rate of 74.3% for stage IV endometriosis. The ROC curve is indicated in . The final model was retested in the validation sample, and the AUC obtained was 0.760 (95% CI: 0.677–0.842), with a sensitivity of 87.2% and specificity of 71.0% for stage IV endometriosis.
Figure 2. ROC curve to predict stage IV endometriosis in training sample (A) and validation sample (B).
Discussion
It is well known that for endometriosis, laparoscopy is costly and undoubtedly risky. Unconsidered surgery may result in damage and missed opportunities for advanced interventions to improve surgical outcomes. Patient medical history, symptoms especially pain-related ones, pelvic examinations, laboratory examinations, and images are employed for the preoperative diagnosis of endometriosis in the clinic (Agarwal et al. Citation2019), but the role of these variables in predictive models or in determining the stage of endometriosis has rarely been analysed. In this study, therefore, an easy model for reliably predicting stage IV endometriosis was proposed with three clinical markers: VAS score, painful nodularity on uterosacral ligaments in pelvic examinations, and bilateral lesions on TVS images.
Many previous studies have attempted to find predictors of preoperative endometriosis severity. In a multicentre study (Nnoaham et al. Citation2012), a model based on menstrual dysphasia and a history of benign ovarian cysts strongly predicts stage III and IV endometriosis (AUC = 84.9, sensitivity =82.3% and specificity =75.8% at an optimal cut-off value of 0.24), which facilitates to prioritise women for surgical investigations in clinical practice and contributes to reducing time to diagnosis, coinciding with the findings of this study. However, this research is more comprehensive compared with theirs due to the additional components of pelvic examinations, laboratory examinations and TVS. In this situation, the gynaecologist can perform an appropriate and comprehensive preoperative assessment to develop the optimal therapeutic scheme, decide whether surgery is necessary and plan a suitable surgical approach.
In this study, VAS was adopted for patients’ self-evaluation for the different types of pain, integrating all types of pain common in endometriosis in a single variable and contributing to the quantitative comparison between patients with stage I–III endometriosis and those with stage IV endometriosis. The VAS score was different between patients with stage I-III endometriosis and those with stage IV endometriosis. The mean VAS score was (3.7 ± 2.8) and (2.0 ± 2.2) points for stage IV and stage I-III endometriosis patients, respectively. 34patients experienced moderate-severe pelvic pain (VAS from 4 to 10) cases of stage IV (53.1%) and 14 cases of stage I–III (18.4%) endometriosis, suggesting that the likelihood of stage IV endometriosis increases with increasing VAS scores. There are consistent findings in the literature, where it is confirmed that there is a correlation between endometriosis stage and severity of symptoms of dysmenorrhoea and non-menstrual pain (Vercellini et al. Citation2007). As to the pathogenesis of pain symptoms, chronic inflammation seems to be the basis (Signorile et al. Citation2022), with the growth of new nerve fibres, peritoneal fluid, stress axis, and psychological factors (Coxon et al. Citation2018). In addition, pelvic adhesions may be more important than cyst diameter as a cause of pain (Kaya et al. Citation2005), reminding us that serious adhesions may be accompanied by severe chronic inflammation, difficult surgical operations or advanced (stage IV) endometriosis. Nonetheless, other studies have only demonstrated that the presence of symptoms is associated with advanced endometriosis, whereas the association between pelvic pain intensity and severity of endometriosis has not been proven (Guo et al. Citation2020, Apostolopoulos et al. Citation2016). These findings urge us to explore the relationship between the symptoms and endometriosis continuously. Besides, Studies show fish oil may have a positive effect on reducing endometriosis-related pain, and they bring the gospel of non-surgical treatment to patients with pain (Habib et al. Citation2022).
Another indicator of stage IV endometriosis was observed in patients with uterosacral ligament nodules with tenderness in pelvic examinations. Currently, there are few studies on the relationship between pelvic examinations and endometriosis staging. There are some studies on whether preoperative prediction of DIE can be achieved by pelvic examinations (Zheng et al. Citation2020). DIE is one of the pathological types of endometrioses with the most aggressive presentation and invading the peritoneal surface by more than 5 mm. It is a multifocal disease primarily affecting the posterior area, frequently involving the uterosacral ligaments and the torus uterinus, as well as the posterior vaginal and anterior rectal walls (Perelló et al. Citation2017). This may be related to the theory of implantation. Because the posterior pelvic cavity is the lowest point of the abdominal cavity, returning menstrual blood is more likely to collect there. Coupled with the anatomical characteristics of the sigmoid colon, the chance of ectopic endometrial implantation increases. As the disease progresses, superficial endometriosis lesions gradually infiltrate deeper, causing tissue adhesions and atrophy. DIE lesions develop in the uterus, ovary, vagina, rectum, ureter and other organs under prolonged inflammatory stimulation, which is the reason why patients with DIE, usually with occlusion of the pouch of Douglas (POD), are detected (Zheng et al. Citation2020). Once POD occlusion is observed, the case is defined as stage IV endometriosis according to the revised ASRM classification of endometriosis 1996. Therefore, patients with DIE or severe endometriosis are prone to some positive signs such as fixed uterine, uterosacral ligament nodule with tenderness and rectovaginal septum nodule with tenderness. Meanwhile, pelvic examinations offer a non-invasive opportunity to detect endometriosis by palpation and to assess sites of pain and organ mobility. Pelvic examinations performed by adequately-trained clinicians are economically feasible and timely (Pascoal et al. Citation2022). Thus, high priority should be given to cases of uterosacral ligament nodules with tenderness as it may serve as a positive sign for patients with stage IV endometriosis.
According to the American College of Obstetricians and Gynaecologists (ACOG) (Kor et al. Citation2020), TVS is the first method to study endometriosis and has been reported to have good sensitivity and excellent specificity in diagnosing endometriosis and reliably predict stage III-IV endometriosis (Guo et al. Citation2020). TVS is regarded as the first-line diagnostic tool for endometriosis, especially DIE (Aas-Eng et al. Citation2020). TVS is easily available, low cost, and readily accepted by women with endometriosis. This study proved the importance of the laterality of lesions of endometriosis on TVS as a variable in predicting stage IV endometriosis. Scoring bilateral lesions according to the revised ASRM classification of endometriosis 1996 increases the likelihood of higher scores and advanced stage. Despite the absence of ultrasound in predicting stage IV endometriosis, the ovarian fixation on TVS images is significantly associated with the presence of ipsilateral ovary endometriosis, POD occlusion, pelvic deep infiltrating endometriosis nodules, and stage III/IV (moderate/severe) endometriosis (Rao et al. Citation2022). The lesion presentation on TVS was not used as a variable in this study, hence more research should be conducted on the relationship between TVS lesion characteristics and endometriosis staging.
Moreover, it is acknowledged that women with endometriosis are more likely to have pelvic floor dysfunction (Faubion et al. Citation2012). In Raimondo’s research, women with DIE have a smaller levator hiatal area at rest (p = 0.03) and during Valsalva manoeuvre (p < 0.01) evaluated by 3D and 4D transperineal ultrasound compared with that in the control group. This shows that 3D and 4D transperineal ultrasound is an objective and non-invasive method for DIE diagnosis (Raimondo et al. Citation2017). Meanwhile, Raimondo’s team also found that women with chronic constipation and endometriosis have sonographic signs of pelvic floor muscle hypertonia in comparison with women with no chronic constipation (Raimondo et al. Citation2022). Therefore, predicting the severity of endometriosis by preoperative ultrasound examination of patients’ pelvic floor function is also a topic that can be further studied.
The optimisation of treatment options for endometriosis remains a challenge in clinical practice. Therapeutic approaches, both surgical and pharmacological, have their own advantages and disadvantages. The combination of surgery and medical therapy appears to be beneficial (Somigliana et al. Citation2017), while the optimal protocol for maximising treatment response lacks clarity. Some studies have attempted to find the appropriate timing of pharmacological treatment in relation to surgery, but the result only indicates that postsurgical medical therapy may be beneficial, while there is insufficient evidence for hormonal suppression therapy at other time points in relation to surgery (Chen et al. Citation2020). It must be admitted that for surgical treatment, the duration and difficulty of surgery increase accordingly with progressive disease stage (Bhatti et al. Citation2018). At present, there is no treatment plan to minimise the risk of intraoperative bleeding and side injury of advanced endometriosis in stage III-IV patients. Keiko et al. reported a patient with a history of recurrent pelvic abscesses who presented with lower abdominal pain and suspected endometriosis. They treated her with GnRH agonists for 3 months to relieve symptoms, making it easier to perform laparoscopic appendectomy in the presence of dense adhesions (Shichiri et al. Citation2021). This provides strong evidence for preoperative medical therapy. We look forward to more research about the best timing of medical therapy in the perioperative period.
This study did have some limitations. First, retrospective studies by their nature have potential limitations and subjective bias. For the research aimed at establishing the predictive model, expansion and external validation are required. Second, in recent years, additional factors not covered in this study have been identified to predict the severity of endometriosis before surgery. For instance, direct analysis of native IgG rockweed glycosylation in serum could be a useful diagnostic tool, convenient and affordable, for differentiating patients with advanced endometriosis (Sołkiewicz et al. Citation2022). A study suggested rising suspicion in patients with migraine because they are more likely to have severe endometriosis (Wu et al. Citation2022). In addition, MRI is considered highly accurate and therefore is often performed in cases of suspected complex endometriosis or before surgery (Pascoal et al. Citation2022). Nevertheless, it was not employed in this study because it is expensive and difficult to be popularised. Third, it was found that not all stage IV patients had typical symptoms that could make them be identified accurately before surgery. Among stage IV patients, there are many young patients without fertility requirements, which were not addressed to ovarian cysts but were identified as having severe endometriosis during surgery. It is difficult to identify these patients in advance. Hopefully, more research will help optimise diagnosis and treatment in the future. Third, at baseline examinations, nearly all patients were automatically diagnosed with stage III or IV endometriosis as long as the endometrioma was at least 1 cm in size, but this did not affect the progress of the study because the objective of this study to predict stage IV from stage III. Finally, the model had an AUC of 0.777, a sensitivity of 71.9%, a specificity of 76.3%, and a correct classification rate of 74.3% for stage IV endometriosis. This result is not perfect and may be related to the reasons mentioned above. We hope that a preoperative predictive model will help to identify and treat patients with severe endometriosis and that the achievement of this study will be useful in the preoperative identification of stage IV endometriosis.
In conclusion, the predictive model for stage IV endometriosis constructed based on three simple, accessible and non-invasive indicators performs better in predicting stage IV endometriosis. Therefore, a complete collection of patient information before surgery, asking about pain and VAS scores, careful completion of pelvic examinations, and application of imaging techniques are suggested for better diagnosis and prediction of advanced endometriosis.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Beijing Anzhen Hospital affiliated to Capital Medical University (2022061X), and informed consent was obtained from all participants involved in this study. This study was registered with the Chinese Clinical Trial Registry (Registration number is ChiCTR2200058414). All methods were performed in accordance with relevant guidelines and regulations. All information obtained from study participants was kept confidential, names or personal identifiers were not included in the study. The medical record number was used to trace back the participants if needed.
Author contributions
ZJ and ZH designed the study. ZJ, ZH, BZL, KJ, WW and GJQ acquired the data. BZL, KJ, WW their assistants completed the operation and scoring. ZH performed the statistical analyses. ZH wrote the manuscript and submitted the manuscript. ZJ revised the paper. All authors approved the final version.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used and analysed during the current study are not publicly available due to the privacy protection of the subjects, but are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Aas-Eng, M.K., et al., 2020. Transvaginal sonographic imaging and associated techniques for diagnosis of ovarian, deep endometriosis, and adenomyosis: A comprehensive review. Seminars in Reproductive Medicine, 38 (2–03), 216–226.
- Agarwal, S.K., et al., 2019. Clinical diagnosis of endometriosis: a call to action. American Journal of Obstetrics and Gynecology, 220 (4), 354.e1–354.e12.
- Apostolopoulos, N.V., et al., 2016. Association between chronic pelvic pain symptoms and the presence of endometriosis. Archives of Gynecology and Obstetrics, 293 (2), 439–445.
- ASRM 1997. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and Sterility, 67, 817–821.
- Bhatti, M., et al., 2018. Pelvic examination may be meaningfully taught to novices and be used to predict operating times for laparoscopic excision of endometriosis in one surgical procedure. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 58 (2), 239–246.
- Chen, I., et al., 2020. Pre - and postsurgical medical therapy for endometriosis surgery. The Cochrane Database of Systematic Reviews, 11 (11), CD003678.
- Chen, T., et al., 2021. The diagnostic value of the combination of hemoglobin, CA199, CA125, and HE4 in endometriosis. Journal of Clinical Laboratory Analysis, 35 (9), e23947.
- Conroy, I., et al., 2021. Pelvic pain: What are the symptoms and predictors for surgery, endometriosis and endometriosis severity. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 61 (5), 765–772.
- Coxon, L., Horne, A.W. and Vincent, K., 2018. Pathophysiology of endometriosis-associated pain: A review of pelvic and central nervous system mechanisms. Best Practice & Research. Clinical Obstetrics & Gynaecology, 51, 53–67.
- Faubion, S.S., Shuster, L.T. and Bharucha, A.E., 2012. Recognition and management of nonrelaxing pelvic floor dysfunction. Mayo Clinic Proceedings, 87 (2), 187–193.
- Guo, Z., et al., 2020. Developing preoperative nomograms to predict any-stage and stage III-IV endometriosis in infertile women. Frontiers in Medicine, 7, 570483.
- Habib, N., et al., 2022. Impact of lifestyle and diet on endometriosis: a fresh look to a busy corner. Przeglad Menopauzalny = Menopause Review, 21 (2), 124–132.
- Kasaven, L.S., et al., 2022. Study protocol for a randomised controlled trial on the use of intraoperative ultrasound-guided laparoscopic ovarian cystectomy (UGLOC) as a method of fertility preservation in the management of benign ovarian cysts. BMJ Open, 12 (7), e060409.
- Kaya, H., et al., 2005. Does the diameter of an endometrioma predict the extent of pelvic adhesions associated with endometriosis? The Journal of Reproductive Medicine, 50 (3), 198–202.
- Kaya Sezginer, E., et al., 2022. Analysis of changes in serum levels and gene expression profiles of novel adipocytokines (omentin, vaspin, irisin and visfatin) and their correlation with serum C-reactive protein levels in women diagnosed with endometriosis. Turkish Journal of Pharmaceutical Sciences, 19 (1), 48–53.
- Kor, E., et al., 2020. Relationship between the severity of endometriosis symptoms (dyspareunia, dysmenorrhea and chronic pelvic pain) and the spread of the disease on ultrasound. BMC Research Notes, 13 (1), 546.
- Nnoaham, K.E., et al., 2012. Developing symptom-based predictive models of endometriosis as a clinical screening tool: results from a multicenter study. Fertility and Sterility, 98 (3), 692–701.e5.
- Pascoal, E., et al., 2022. Strengths and limitations of diagnostic tools for endometriosis and relevance in diagnostic test accuracy research. Ultrasound in Obstetrics & Gynecology, 60, 309–327.
- Perelló, M., et al., 2017. Markers of deep infiltrating endometriosis in patients with ovarian endometrioma: a predictive model. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 209, 55–60.
- Peterson, C.M., et al., 2013. Risk factors associated with endometriosis: importance of study population for characterizing disease in the ENDO Study. American Journal of Obstetrics and Gynecology, 208 (6), 451.e1–11–451.11.
- Raimondo, D., et al., 2022. Pelvic floor dysfunction at transperineal ultrasound and chronic constipation in women with endometriosis. International Journal of Gynaecology and Obstetrics , 159 (2), 505–512.
- Raimondo, D., et al., 2017. Pelvic floor muscle dysfunction on 3D/4D transperineal ultrasound in patients with deep infiltrating endometriosis: a pilot study. Ultrasound in Obstetrics & Gynecology, 50 (4), 527–532.
- Rao, T., Condous, G. and Reid, S., 2022. Ovarian immobility at transvaginal ultrasound: An important sonographic marker for prediction of need for pelvic sidewall surgery in women with suspected endometriosis. Journal of Ultrasound in Medicine, 41 (5), 1109–1113.
- Shafrir, A.L., et al., 2018. Risk for and consequences of endometriosis: A critical epidemiologic review. Best Practice & Research Clinical Obstetrics & Gynaecology, 51, 1–15.
- Shichiri, K., et al., 2021. Preoperative hormonal therapy for a patient with appendiceal endometriosis. BMJ Case Reports, 14, e245667.
- Signorile, P.G., et al., 2022. Endometriosis: A Retrospective analysis of clinical data from a cohort of 4,083 patients, with focus on symptoms. In Vivo, 36 (2), 874–883.
- Sołkiewicz, K., et al., 2022. The alterations of serum IgG Fucosylation as a potential additional new diagnostic marker in advanced endometriosis. Journal of Inflammation Research, 15, 251–266.
- Somigliana, E., et al., 2017. Postoperative hormonal therapy after surgical excision of deep endometriosis. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 209, 77–80.
- Vercellini, P., et al., 2007. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Human Reproduction, 22, 266–271.
- Wu, Y., et al., 2022. Migraine is more prevalent in advanced-stage endometriosis, especially when co-occuring with adenomoysis. Frontiers in Endocrinology, 12, 814474.
- Zheng, Y.M., et al., 2020. Incidence of deeply infiltrating endometriosis among 240 cases of pelvic endometriosis and analysis of its clinical and pathological characteristics. Zhonghua Fu Chan Ke Za Zhi, 55, 384–389.