

Abstract
The current systematic analysis and meta-analysis was aimed to evaluate the association between radiation-induced lymphopenia (RIL) and survival of women with cervical cancer (CC). PubMed, Embase, Web of Science, and Cochrane Library were searched for relevant cohort studies comparing survival between women with CC who developed versus not developed RIL after radiotherapy. We pooled the results using a random-effects model that incorporates heterogeneity. In the meta-analysis, 952 women with CC were included from eight cohort studies. Overall, 378 (39.7%) of them had RIL after radiotherapy. During a median follow-up duration of 41.8 months, pooled results showed that RIL was independently associated with poor overall survival (hazard ratio [HR]: 2.67, 95% confidence interval [CI]: 1.81 to 3.94, p < 0.001; I2 = 20%) and progression-free survival (HR: 2.17, 95% CI: 1.58 to 2.98, p < 0.001; I2 = 0%). Predefined subgroup analyses showed similar results in patients with grade 3-4 and grade 4 RIL, in patients with RIL diagnosed during or after the radiotherapy, and in studies with quality score of seven or eight points (p values for subgroup effect all < 0.05). In conclusion, women with RIL were associated with poor survival after radiotherapy for CC.
Introduction
According to the statistics in 2020, cervical cancer (CC) is the fourth most commonly diagnosed type of cancer and the fourth leading cause of cancer-related mortality in women worldwide (Miller et al. Citation2022). The management of women affected by gynecological cancers needs a particular attention even to the preservation of an appropriate quality of life and sexual function (Fagotti et al. Citation2016, Dessole et al. Citation2018), which risk being severely impaired by surgical/chemo/radio treatments, particularly for those with CC (Lagana et al. Citation2021, Vizzielli et al. Citation2021). Currently, radiotherapy has become a crucial component for the treatment of locally advanced CC (Chargari et al. Citation2022, Mayadev et al. Citation2022). Although the efficacy of radiotherapy for CC has been validated in accumulating studies, this treatment could also lead to toxicities (Cohen et al. Citation2019). One of the main adverse events related to radiotherapy in women with CC is radiation-induced lymphopenia (RIL) (Cesaire et al. Citation2020). The incidence of grade 3-4 RIL in women with CC varies according to previous studies, which could be especially high for women who received concurrent chemoradiotherapy (CCRT) (Lakomy et al. Citation2021). Since lymphocytes have been recognised as main players of the immune systems against the pathogenesis and progression of various cancers (Schreiber et al. Citation2011), RIL has been suggested to correlate with poor survival in patients with cancer (Venkatesulu et al. Citation2018). Although a previous meta-analyses published in 2021 has confirmed that a grade 3-4 RIL was related to poor survival in patients receiving radiotherapy for solid tumours (Damen et al. Citation2021), only two studies were included for women with CC (Wu et al. Citation2016, Onal et al. Citation2018). Accordingly, a subgroup analysis limited to women with CC failed to show a significantly association between severe RIL and poor survival in this meta-analysis (Damen et al. Citation2021). In recent years, several studies have been published to evaluate the influence of RIL on survival in women with CC receiving radiotherapy, and the results of them were not consistent (Cho et al. Citation2016, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022). In view of the limited sample size of these studies (Cho et al. Citation2016, Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022), a meta-analysis is needed to provide a pooled result. Therefore, we performed a systematic review and meta-analysis to comprehensively evaluate the influence of RIL on survival of women with CC who received radiotherapy.
Materials and methods
According to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al. Citation2021a, Citation2021b) and the Cochrane Handbook (Higgins et al. Citation2021) guideline, this meta-analysis was designed, performed, and reported
Literature retrieving
A search was conducted in the PubMed, Embase, Web of Science, and Cochrane Library for relevant cohort studies from the inception of the databases to November 21, 2022. The following combined search strategy was used: (1) ‘lymphopenias’ OR ‘lymphocytopenia’ OR ‘lymphocytopenias’ OR ‘lymphopenia’ OR ‘RIL’ OR ‘lymphocytop*’ OR ‘lymphocytop*’; (2) ‘radiotherapy’ OR ‘radiation’ OR ‘radiochemotherapy’ OR ‘chemoradiotherapy’; (3) cervical’ OR ‘cervix’; and (4) ‘cancer’ OR ‘carcinoma’ OR ‘tumour’ OR ‘neoplasm’ OR ‘malignancy’. The detailed search strategy for each database is shown in the Supplemental Material. We only considered clinical studies published as full-length articles in English in peer-reviewed journals. A manual review of citations of relevant original articles and reviews was conducted to supplement our search.
Study selection
For this study, an inclusion criteria based on PICOS was applied.
P (patients): An adult population with a confirmed diagnosis of CC who received radiotherapy, regardless of the stage or histology type of the cancer.
I (exposure): Women with CC who developed RIL during or after the radiotherapy.
C (control): Women with CC who did not develop RIL during or after the radiotherapy.
O (outcomes): The overall survival (OS) and/or progression-free survival (PFS) were compared between those with versus without RIL. In general, OS refers to the interval between the beginning of treatment and the date on which the patient ultimately dies, while PFS is the interval between the beginning of treatment and the date on which the patient recurrences or develops a progressive disease.
S (study design): Prospective or retrospective studies.
For the studies included in this meta-analysis, the diagnosis of RIL was consistent with the criteria used in the original studies. Reviews, preclinical studies, studies enrolling women with other cancers rather than CC, studies that did not evaluate RIL, or studies that did not report the survival outcomes were excluded from the meta-analysis.
Data collection and quality assessment
Two authors separately carried out literature searches, data collection, and quality assessments. If discrepancies occurred, a third author was consulted. In order to analyse the association between RIL and survival outcomes in women with CC, data of study information, patient and cancer characteristics, main anticancer treatment modalities, definition and timing for the diagnosis of RIL, number of women with RIL, durations of follow-up, outcomes evaluated and variables adjusted in the regression model were collected. A Newcastle-Ottawa Scale (NOS) (Wells et al. Citation2010) was used to assess study quality based on criteria for participant selection, comparability of groups, and validity. According to the study quality system, a study that has more stars is considered to be of higher quality.
Statistical analyses
The main objective was to determine the risks of OS and PFS comparing between CC patients with high versus without RIL after radiotherapy, which were presented as hazard ratios (HRs) and the confidence intervals (CIs). By using 95% CIs or p-values, HRs and standard errors (SEs) could be calculated, and a subsequent logarithmical transformation kept the variance stabilised and normalised. Cochran Q test and I2 statistics were used to estimate study heterogeneity (Higgins and Thompson Citation2002), and the significant heterogeneity is reflected by an I2 > 50%. The results were combined using a random-effects model incorporating heterogeneity’s influence (Higgins et al. Citation2021). A sensitivity analysis that omitted one study at a time was conducted to observe what effect each study has on the overall results (Patsopoulos et al. Citation2008). In addition, subgroup analyses were conducted to examine how study characteristics influenced the results. An estimate of publication bias was made by constructing funnel plots and applying Egger’s regression asymmetry test to the visual judgement of their symmetry (Egger et al. Citation1997). These analyses were achieved using RevMan (version 5.1; Cochrane Collaboration, Oxford, UK) and Stata (version 12.0; Stata Corporation, College Station, TX).
Results
Studies obtained
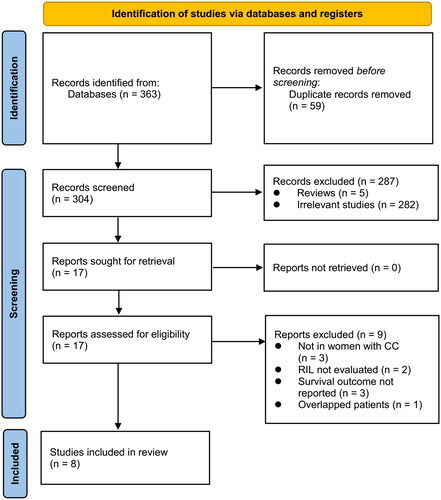
As shown in , 363 articles were found during the initial search, and 304 remained after excluding duplicate records. In addition, we excluded 287 articles from the meta-analysis because their titles and abstracts did not relate to the topic, leaving 17 studies for full-text analysis. A full-text review had excluded nine studies, leaving eight eligible studies (Cho et al. Citation2016, Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022) for the meta-analysis. The reasons for removing the 25 studies are shown in .
Figure 1. A summary of the literature search and study identification process.
Characteristics of the included studies
As shown in , eight retrospective cohort studies (Cho et al. Citation2016, Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022) involving 952 women with CC who underwent radiotherapy were included in the meta-analysis. These studies were published between 2016 and 2022, and located in Korea, the United States, Turkey, France, Japan, and China. The sample size of each study varied from 71 to 168. The mean ages of the women ranged from 45 to 64 years. Six of the studies included women with stage I-IV CC (Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Xu et al. Citation2022, Yang et al. Citation2022), while the other two included women with stage I-III CC (Cho et al. Citation2016, Shi et al. Citation2022). As for the histology of CC, squamous cell carcinoma was the dominant type, which accounted for 90.5% (862/952) of the patients. In general, RIL was defined as any lymphopenia (ALC < 1000/ul) in one study (Holub et al. Citation2020), as severe lymphopenia (ALC < 600/ul) in one study (Taguchi et al. Citation2020), as grade 3-4 lymphopenia (ALC < 500/ul) in three studies (Wu et al. Citation2016, Onal et al. Citation2018, Yang et al. Citation2022), and as grade 4 lymphopenia (ALC < 200/ul) in the other three studies (Cho et al. Citation2016, Shi et al. Citation2022, Xu et al. Citation2022). Among them, RIL was diagnosed during radiotherapy in four studies (Cho et al. Citation2016, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022), and after radiotherapy in the other four studies (Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020). Overall, 378 (39.7%) of the patients had RIL after radiotherapy. The median follow-up durations varied from 26 to 68 months. The outcome of OS was reported in seven studies (Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022), and the outcome of PFS was also reported in seven studies (Cho et al. Citation2016, Wu et al. Citation2016, Onal et al. Citation2018, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022). A multivariate approach was used to study the association between RIL and survival outcomes of women with CC in all of the included studies, and confounding factors such as age, tumour stage, histology type, anticancer treatments, dose and duration of radiotherapy etc. were adjusted to varying degrees. Studies included in this review received NOS on a scale between 7 and 8, suggesting generally good study quality ().
Table 1. Study characteristics.
Table 2. Study quality evaluation via the Newcastle-Ottawa Scale.
RIL and OS of women with CC
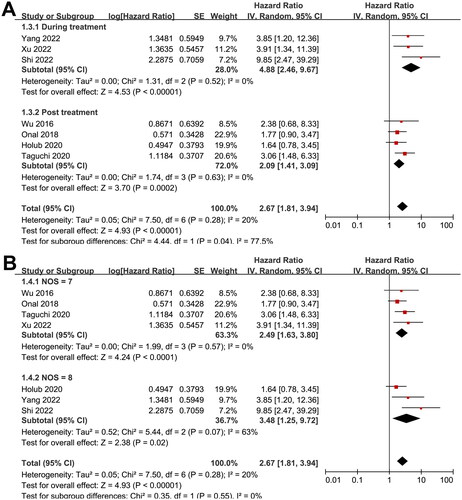
Seven studies (Wu et al. Citation2016, Onal et al. Citation2018, Holub et al. Citation2020, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022) reported the association between RIL and OS. Pooled results showed that RIL was independently associated with a poor OS in women with CC (HR: 2.67, 95% CI: 1.81 to 3.94, p < 0.001; ) with no significant heterogeneity (p for Cochran Q test = 0.28, I2 = 20%). Sensitivity analysis by excluding one study at a time showed consistent results (RR: 2.36 to 3.00, p all < 0.05). Predefined subgroup analyses showed consistent results in patients with grade 3-4 (RR: 2.19, 95% CI: 1.29 to 3.71, p = 0.004; I2 = 0%) and grade 4 RIL (RR: 5.57, 95% CI: 2.31 to 13.43, p < 0.001; I2 = 7%; ), in patients with RIL diagnosed during (RR: 4.88, 95% CI: 2.46 to 9.67, p < 0.001; I2 = 0%) or after radiotherapy (RR: 2.09, 95% CI: 1.41 to 3.09, p < 0.001; I2 = 0%; ), and in studies with quality score of seven (RR: 2.49, 95% CI: 1.63 to 3.80, p < 0.001; I2 = 0%) or eight points (RR: 3.48, 95% CI: 1.25 to 9.72, p = 0.02; I2 = 63%; ). Examination for subgroup difference suggested a stronger relationship of RIL diagnosed during radiotherapy than RIL diagnosed after during radiotherapy with OS (p for subgroup difference = 0.04).
Figure 2. Forest plots for the meta-analyses regarding the association between RIL and OS in women with CC. A, overall meta-analysis; and B, subgroup analysis according to grade of RIL.
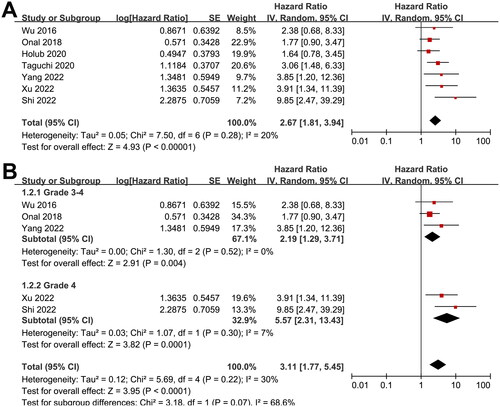
Figure 3. Forest plots for the subgroup-analyses regarding the association between RIL and OS in women with CC. A, subgroup analysis according to the timing of RIL diagnosis; and B, subgroup analysis according to the study quality scores.
RIL and PFS of women with CC
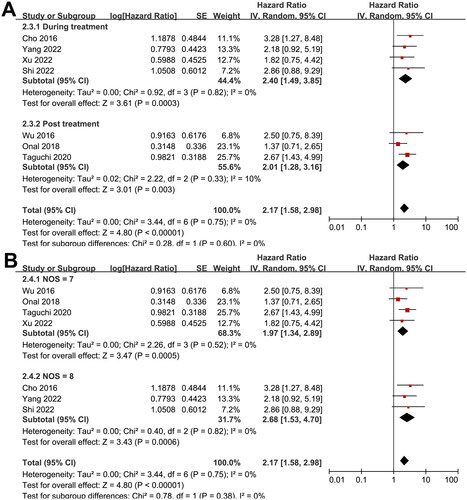
Meta-analysis with seven studies (Cho et al. Citation2016, Wu et al. Citation2016, Onal et al. Citation2018, Taguchi et al. Citation2020, Shi et al. Citation2022, Xu et al. Citation2022, Yang et al. Citation2022) demonstrated that RIL was associated with a poor PFS in women with CC (HR: 2.17, 95% CI: 1.58 to 2.98, p < 0.001; I2 = 0%; ). By omitting one study at a time, sensitivity analysis retrieved similar results (RR: 2.02 to 2.49, p all < 0.05). Predefined subgroup analysis also showed consistent results in patients with grade 3-4 (RR: 1.74, 95% CI: 1.07 to 2.81, p = 0.02; I2 = 0%) and grade 4 RIL (RR: 2.50, 95% CI: 1.41 to 4.40, p = 0.002; I2 = 0%; ), in patients with RIL diagnosed during (RR: 2.40, 95% CI: 1.49 to 3.85, p < 0.001; I2 = 0%) or after radiotherapy (RR: 2.01, 95% CI: 1.28 to 3.16, p = 0.003; I2 = 10%; ), and in studies with quality score of seven (RR: 1.97, 95% CI: 1.34 to 2.89, p < 0.001; I2 = 0%) or eight points (RR: 2.68, 95% CI: 1.53 to 4.70, p < 0.001; I2 = 63%; ). No significant differences were detected between these subgroups (p for subgroup difference = 0.34, 0.60, and 0.38, respectively).
Figure 4. Forest plots for the meta-analyses regarding the association between RIL and PFS in women with CC. A, overall meta-analysis; and B, subgroup analysis according to grade of RIL.
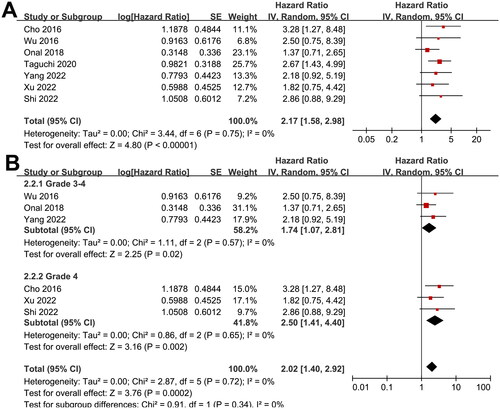
Figure 5. Forest plots for the subgroup-analyses regarding the association between RIL and PFS in women with CC. A, subgroup analysis according to the timing of RIL diagnosis; and B, subgroup analysis according to the study quality scores.
Publication bias
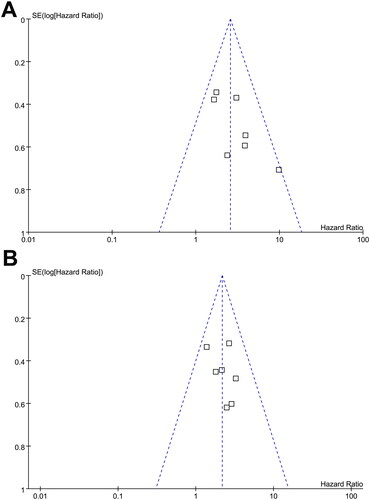
According to , funnel plots for OS and PFS outcomes show symmetry, indicating low risks of publication bias. In addition, Egger’s regression tests indicated low risk of publication bias in meta-analyses analysing RIL with OS and PFS in women with CC (p = 0.41 and 0.55, respectively).
Figure 6. Funnel plots for the publication bias underlying the meta-analyses; A, funnel plots for the meta-analysis of OS; and B, funnel plots for the meta-analysis of PFS.
Discussion
In this systematic review and meta-analysis, we pooled the results of eight eligible observational studies, and the results showed that in women with CC receiving radiotherapy, RIL was associated with poor survival outcomes during follow-up of up to 41.8 months. The results were consistent for outcomes of OS and PFS. Moreover, similar results were obtained in sensitivity analyses by excluding one study at a time, and in subgroup analysis in patients with grade 3-4 and grade 4 RIL, in patients with RIL diagnosed during and after the radiotherapy, and in studies with different quality scores. Based on these findings, it could be concluded that RIL may be an independent risk factor of poor survival of women with CC receiving radiotherapy.
To the best of our knowledge, meta-analyses focussing on the potential prognostic significance of RIL in women with CC receiving radiotherapy are rare. Although two previous meta-analyses have suggested the potential role of RIL as a predictor of poor prognosis of patients with solid cancers (Damen et al. Citation2021, El Houat et al. Citation2023), few studies in women with CC were included. In addition, although a subgroup analysis was performed in one of the previous meta-analyses to evaluate the influence of RIL on survival of women with CC, only two studies were included, and the pooled results failed to show a significant influence of RIL on OS in these patients (Damen et al. Citation2021). Several methodological strengths should be mentioned before the results of the meta-analysis were interpreted. First, an extensive literature search was performed in four electronic databases to obtain the up-to-date literatures regarding the association with RIL with survival in women with CC. Overall, eight studies were included in this meta-analysis, and five of them were published after 2020. Secondly, only cohort studies were considered, which therefore could indicate a longitudinal relationship between RIL and poor survival of women with CC after radiotherapy. Moreover, multivariate analyses were adopted in all of the included studies when the association between RIL and survival outcomes of women with CC was estimated, which therefore could derive a potential independent association between RIL and poor survival. Finally, the robustness of the finding was further validated in sensitivity analysis and multiple predefined subgroup analysis. Particularly, we found both the grade 3-4 and grade 4 RIL, and RIL diagnosed during or after the radiotherapy were associated with poor survival outcomes in women with CC. These findings further confirmed the adverse influence of severe RIL (grade 3-4) on prognosis of women with CC receiving radiotherapy, which was not only significant during radiotherapy, but still remarkable after the radiotherapy.
The potential mechanisms underlying the adverse influence of RIL on survival of women with CC are likely to be similar to the mechanisms for other solid tumours. In view of the important role of lymphocytes as active components of immune system, RIL may lead to poor prognosis of women with CC by mediating decreased anti-cancer immunity and increased infection risk (Terrones-Campos et al. Citation2019). These hypotheses could also be supported by previous studies which showed that a low absolute lymphocyte count before the treatment could also predict the poor survival of women with CC (Chen et al. Citation2015). In addition, these results were consistent with the findings of a recent study, which showed that patients with aggressive CC can be differentiated from non-aggressive ones by using the exponential slope of changes of absolute lymphocyte counts during CCRT (Cho et al. Citation2022). In addition, a recent clinical studies failed to show that positron emission tomography-based bone marrow-sparing image-guided intensity modulated radiation therapy (IMRT) was superior to standard IMRT in improving the survival of women with locally advanced, although the grade ≥ 3 neutropenia was reduced but the incidence of RIL was not changed. These findings may further reflect the close relationship between RIL and poor survival of women with CC (Williamson et al. Citation2022). Taken together, results of the meta-analysis and the above studies highlight the importance of identification and correction of RIL for women with CC receiving radiotherapy, which may be important to improve the survival of patients with CC. With regard to ways of reducing the risk of lymphopenia or restoration of the number of lymphocytes in the peripheral blood, several measures can be attempted. For example, for patients at higher risk of severe RIL, measures can be taken before, during and after radiation treatment, such as close monitoring of peripheral lymphocyte count, adjustment the treatment strategies of chemoradiotherapy to reduce the risk of RIL, and concomitant use of agents that stimulating the generation of peripheral lymphocytes etc. (Cesaire et al. Citation2020). However, to the best of our knowledge, no relevant clinical trials have observed if effectively prevention or correction of RIL could improve the survival of women with CC. Studies are urgently needed in this regard.
Our study also has limitations. Firstly, only eight studies were included in the meta-analysis. According to the Cochrane Handbook, the test of publication bias using funnel plot and Egger’s test should be interpret cautiously when the number of studies less than 10. Therefore, we could not completely exclude the possibility of publication bias. In addition, although the statistical heterogeneity was not significant among the meta-analysis, clinical heterogeneity may remain. We were unable to determine whether age, comorbidities, and ethnicity of the patients may affect the association between RIL and poor survival of women receiving CC. Moreover, all of the included studies were of retrospective design, which may expose to recall and selection biases. The results of the meta-analysis should better be validated in large-scale prospective studies. Furthermore, immunotherapy was not included in either of the studies in the meta-analysis. Theoretically, the efficacy of immunotherapy could be compromised by reduced absolute lymphocyte counts. In view of the increasing use of immunotherapy for women with CC, studies are needed to determine the influence of RIL on survival in these patients. Finally, as a meta-analysis of observational studies, we could not determine the causative relationship between RIL and poor prognosis of women with CC on the basis of current findings. As mentioned previously, clinical trials are needed to determine if effective preventative strategies for RIL could improve the survival of women with CC.
Conclusions
In conclusion, results of the meta-analysis indicate that RIL may be independently associated with poor survival of women with CC after radiotherapy. Although large-scale prospective studies are needed for further validation, results of the meta-analysis highlight the importance to determine whether effective prevention of RIL could improve the prognosis of women with CC.
Author contributions
Hongming Cao and Baihui Gu conceived the study. Hongming Cao and Haiyan Yan performed literature search, study identification, quality evaluation, and data collection. Hongming Cao and Shoumin Bai performed statistical analyses and interpreted the results. Hongming Cao and Baihui Gu drafted the manuscript. All authors revised the manuscript and approved the submission.
Supplemental Material
Download MS Word (17.1 KB)Acknowledgements
All procedures carried out in studies involving human participants are in accordance with the ethical standards of institutions and/or national research councils, as well as with the 1964 Helsinki Declaration and its subsequent revisions or similar ethical standards. Formal consent is not required for this type of research.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data used in this paper are from published articles.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Cesaire, M., et al., 2020. [Mechanisms of radiation-induced lymphopenia and therapeutic impact]. Bulletin du Cancer, 107 (7-8), 813–822.
- Chargari, C., et al., 2022. Radiotherapy of cervical cancer. Cancer Radiotherapie: Journal de la Societe Francaise de Radiotherapie Oncologique, 26 (1-2), 298–308.
- Chen, L., et al., 2015. Decreased pretreatment lymphocyte/monocyte ratio is associated with poor prognosis in stage Ib1-IIa cervical cancer patients who undergo radical surgery. OncoTargets and Therapy, 8, 1355–1362.
- Cho, O., Chun, M. and Chang, S.J., 2022. Exponential slope from absolute lymphocyte counts during radio-chemotherapy can predict an aggressive course of cervical cancer. Cancers, 14, 5109.
- Cho, O., et al., 2016. Prognostic value of severe lymphopenia during pelvic concurrent chemoradiotherapy in cervical cancer. Anticancer Research, 36 (7), 3541–3547.
- Cohen, P.A., et al., 2019. Cervical cancer. Lancet, 393 (10167), 169–182.
- Damen, P.J.J., et al., 2021. The influence of severe radiation-induced lymphopenia on overall survival in solid tumors: a systematic review and meta-analysis. International Journal of Radiation Oncology, Biology, Physics, 111 (4), 936–948.
- Dessole, M., et al., 2018. Quality of life in women after pelvic exenteration for gynecological malignancies: a multicentric study. International Journal of Gynecological Cancer, 28 (2), 267–273.
- Egger, M., et al., 1997. Bias in meta-analysis detected by a simple, graphical test. BMJ, 315 (7109), 629–634.
- El Houat, Y., et al., 2023. Meta-analysis and critical review: association between radio-induced lymphopenia and overall survival in solid cancers. Advances in Radiation Oncology, 8 (2), 101038.
- Fagotti, A., et al., 2016. Phase III randomised clinical trial comparing primary surgery versus neoadjuvant chemotherapy in advanced epithelial ovarian cancer with high tumour load (SCORPION trial): Final analysis of peri-operative outcome. European Journal of Cancer, 59, 22–33.
- Higgins, J., et al., 2021. Cochrane Handbook for Systematic Reviews of Interventions version 6.2. The Cochrane Collaboration. www.training.cochrane.org/handbook
- Higgins, J.P. and Thompson, S.G., 2002. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21 (11), 1539–1558.
- Holub, K., Vargas, A. and Biete, A., 2020. Radiation-induced lymphopenia: the main aspects to consider in immunotherapy trials for endometrial and cervical cancer patients. Clinical & Translational Oncology, 22 (11), 2040–2048.
- Lagana, A.S., et al., 2021. Vaginal stenosis after cervical cancer treatments: challenges for reconstructive surgery. Journal of Investigative Surgery: The Official Journal of the Academy of Surgical Research, 34 (7), 754–755.
- Lakomy, D.S., et al., 2021. Immune correlates of therapy outcomes in women with cervical cancer treated with chemoradiotherapy: A systematic review. Cancer Medicine, 10 (13), 4206–4220.
- Mayadev, J.S., et al., 2022. Global challenges of radiotherapy for the treatment of locally advanced cervical cancer. International Journal of Gynecological Cancer, 32 (3), 436–445.
- Miller, K.D., et al., 2022. Cancer treatment and survivorship statistics, 2022. CA: A Cancer Journal for Clinicians, 72 (5), 409–436.
- Onal, C., et al., 2018. The utility of pretreatment and posttreatment lymphopenia in cervical squamous cell carcinoma patients treated with definitive chemoradiotherapy. International Journal of Gynecological Cancer, 28 (8), 1553–1559.
- Page, M.J., et al., 2021a. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 372, n71.
- Page, M.J., et al., 2021b. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ, 372, n160.
- Patsopoulos, N.A., Evangelou, E. and Ioannidis, J.P., 2008. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. International Journal of Epidemiology, 37 (5), 1148–1157.
- Schreiber, R.D., Old, L.J. and Smyth, M.J., 2011. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science, 331 (6024), 1565–1570.
- Shi, F., et al., 2022. Impact of hematologic toxicities during concurrent chemoradiation for cervical cancer. Obstetrics & Gynecology Science, 65 (2), 176–187.
- Taguchi, A., et al., 2020. Postradiotherapy persistent lymphopenia as a poor prognostic factor in patients with cervical cancer receiving radiotherapy: a single-center, retrospective study. International Journal of Clinical Oncology, 25 (5), 955–962.
- Terrones-Campos, C., et al., 2019. Lymphocyte count kinetics, factors associated with the end-of-radiation-therapy lymphocyte count, and risk of infection in patients with solid malignant tumors treated with curative-intent radiation therapy. International Journal of Radiation Oncology, Biology, Physics, 105 (4), 812–823.
- Venkatesulu, B.P., et al., 2018. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Critical Reviews in Oncology/Hematology, 123, 42–51.
- Vizzielli, G., et al., 2021. Is a vaginectomy enough or is a pelvic exenteration always required for surgical treatment of recurrent cervical cancer? a propensity-matched study. Annals of Surgical Oncology, 28 (6), 3281–3290.
- Wells, G.A., et al., 2010. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- Williamson, C.W., et al., 2022. Positron emission tomography-guided bone marrow-sparing radiation therapy for locoregionally advanced cervix cancer: final results from the INTERTECC Phase II/III trial. International Journal of Radiation Oncology, Biology, Physics, 112 (1), 169–178.
- Wu, E.S., et al., 2016. Lymphopenia and its association with survival in patients with locally advanced cervical cancer. Gynecologic Oncology, 140 (1), 76–82.
- Xu, Z., et al., 2022. A machine learning model for grade 4 lymphopenia prediction during pelvic radiotherapy in patients with cervical cancer. Frontiers in Oncology., 12, 905222.
- Yang, L., et al., 2022. Early onset of severe lymphopenia during definitive radiotherapy correlates with mean body dose and predicts poor survival in cervical cancer. Cancer Biomarkers: Section A of Disease Markers, 34 (1), 149–159.