

Abstract
This study assessed the efficacy and safety between broad spectrum penicillin (P2) with or without beta-lactamase inhibitors (P2+) versus first and second generation cephalosporins (C1&C2) in the prevention of post-cesarean infections. Relevant randomized controlled trials (RCTs) were searched in English and Chinese databases: nine RCTs were involved. Six trials compared P2+ vs C1&C2, no differences were found between interventions for endometritis, wound infection, urinary tract infection, febrile morbidity and maternal rashes. Four trials compared P2 vs C1&C2, no differences were found between interventions for endometritis, febrile morbidity, wound infection and urinary tract infection. Postoperative hospitalization was longer for women in P2 than C1&C2. Based on these results, P2/P2+ and C1&C2 may have similar efficacy on postoperative infections after cesarean section, there is no data on infant outcomes. PROSPERO Registration Number: CRD42022345721.
Introduction
Cesarean section is a routine surgery in critical obstetric cases. With the development of cesarean section, the rate of cesarean delivery continues to increase worldwide (Abdel Jalil et al. Citation2017). However, cesarean section is considered to be a clean-contaminated procedure and one of the most important risk factors for postpartum infection, with a global infection range of 2.5%–20.5% (Conroy et al. Citation2012), the risk of infections is 5–20-fold higher for women who have a cesarean delivery than for vaginal births (Van Schalkwyk and Van Eyk Citation2017). Good surgical technique is important for reducing infections. Additionally, guidelines of the American College of Obstetricians and Gynecologists (Committee on Practice Bulletins-Obstetrics Citation2018) recommend that the use of prophylactic antibiotics before cesarean section to reduce postoperative endometritis, wound infection, fever and severe infectious complications including pelvic abscess, bacteremia and sepsis, these more serious complications can lead to maternal deaths. Prophylactic antibiotics can decrease the risk of postoperative infections by >50% (Lamont et al. Citation2011). However, antibiotics can have adverse effects on the mother and infant. Antibiotics administered to women during delivery may have a direct impact on the offspring’s microbiota and interfere with the development of the infant’s immune system (Mutic et al. Citation2017, Stinson et al. Citation2018). Therefore, the selection of effective and safe prophylactic antibiotics is particularly important.
During cesarean section, prophylactic antibiotics should be effective against the following pathogens: skin colonizers, primarily gram-positive cocci, particularly including Staphylococcus aureus and Streptococci; and vaginal colonizers, including anaerobes and, gram-negative bacilli (Gyte et al. Citation2014). Furthermore, such a ideally prophylactic antibiotics should be: (1) unrelated to the development of antimicrobial resistance; (2) able to attain adequate serum and tissue levels throughout the procedure; (3) lower cost and be well-tolerated. Currently, guidelines for the clinical application of antimicrobial therapy in China recommend C1&C2 with or without metronidazole as prophylactic antibiotics (National Health and Family Planning Commission of China Citation2015). The American College of Obstetricians and Gynecologists and the Canadian Society of Obstetrics and Gynaecology (Van Schalkwyk and Van Eyk Citation2017, Committee on Practice Bulletins-Obstetrics Citation2018) have recommended C1 such as cefazolin as the first choice for prophylaxis. Despite there being clear guidelines regarding the recommendation of prophylactic antibiotics, differences in clinical practices remain: there are many interfering factors depending on variability in local policies or an obstetrician’s preference. Several clinical studies (Gyte et al. Citation2014) have also reported the use of P2 or P2+ (eg ampicillin and ampicillin/sulbactam) as prophylaxis. Although P2 are similar in antibacterial spectrum to C1&C2, the use of P2 for antibiotic prophylaxis remains questionable, considering that ampicillin is prone to resistant to betalactamase-producing Staphylococcus, resulting in its ineffectiveness, and allergic reactions to penicillin under anesthesia are difficult to identify (Obstetrics and Gynecology Pharmacy Group, Hospital Pharmaceutical Committee, Chinese Pharmaceutical Association et al. Citation2021). Compared with C1&C2, the antimicrobial combination of ampicillin/sulbactam has a broader antibacterial spectrum including anaerobic bacteria and Enterococci (Dervisoglou et al. Citation2006).
It is not clear whether any one particular antibiotic is superior, and antibiotics given perinatally can also adversely affect the newborn’s developing immune system and microbiome. Therefore, the aim of this study was to determine the efficacy and safety of the P2/P2+ vs C1&C2 in reducing postoperative infections in women and to investigate their adverse effects on mother and infant based on the best available evidence.
Materials and methods
Protocol and registration
The protocol for this review is registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the number CRD42022345721.
Literature search
We selected RCTs by searching English databases (Cochrane Library, PubMed and Embase) and Chinese databases (CNKI, CSTJ, Wanfang Literature Data). The English search terms included ‘Ampicillin’, ‘Cefazolin’, ‘Cefuroxime’, ‘Cephalosporins’ and ‘caesarean section’. The Chinese search terms were ‘Anbianxilin’, ‘Toubaozuolin’, ‘Toubaojunsu’, ‘Pougongchan’ and others. The database was collected up to January 2022. In addition, we manually screened references of studies and review articles for relevant studies.
Eligibility criteria
Studies fulfilling the following criteria were included: (1) Type of study: RCTs; (2) Participants: pregnant women undergoing cesarean section, both elective and non-elective; (3) Intervention: the comparison of P2+ vs C1&C2; the comparison of P2 vs C1&C2. Exclusion criteria: (1) Non-RCTs; (2) Studies that were incomplete, outcome effects that were unclear, or data that could not be extracted. Main outcomes: endometritis, febrile morbidity, wound infection, urinary tract infection, maternal rashes and length of hospital stay.
Data collection and risk of bias assessment
Two investigators (Song and Yan) independently selected the literature according to the pre-established eligibility criteria, carried out data extraction using a standardized tool and assessed the risk of bias for each study using criteria outlined in the Cochrane Handbook. If there were discrepancies, they were resolved with a third investigator (Bu). Evaluation included random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other possible biases.
Statistical analysis
Meta-analysis was performed using Rev Man 5.4 software. Enumeration data of outcome evaluation were statistically analyzed using the relative risk (RR). Continuous data were analyzed using mean difference (MD). The 95% confidence interval (95% CI) was used for interval estimation. Heterogeneity was assessed using the I2 test. If I2 <50%, the fixed-effect model was used. If I2 >50%, it indicated that there was statistical heterogeneity between trials. If there was no clinical or methodological heterogeneity, the random-effect model was preferred.
Results
Search results
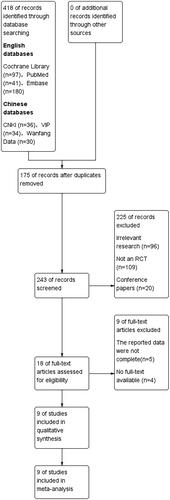
The database searches retrieved 418 records and 243 studies were retained after duplicates were removed, then 225 studies were excluded because the title/abstract did not meet the inclusion criteria or satisfied one of the exclusion criteria. After reading the full text, 9 articles were excluded and the final 9 RCTs were included ().
Figure 1. Study flow diagram.
Characteristics of included studies
Nine RCTs involving 1998 pregnant women were eligible in the meta‐analysis. Six studies compared P2+ vs C1&C2 (Bracero Citation1997, Noyes et al. Citation1998, Busowski et al. Citation2000, Spinnato et al. Citation2000, Jyothi et al. Citation2010, Ziogos et al. Citation2010) and four studies compared P2 to C1&C2 (Spinnato et al. Citation2000, Zhang et al. Citation2010, Mivumbi et al. Citation2014, Fang Citation2021). Characteristics of the nine included studies are shown in .
Table 1. Characteristics of the nine studies included in the systematic review.
Risk of bias assessment
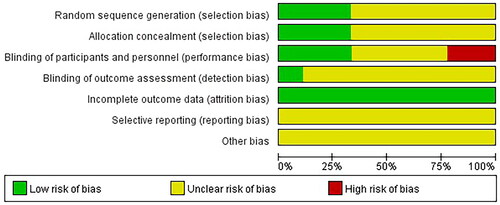
Among the nine studies, three (Bracero Citation1997, Busowski et al. Citation2000, Spinnato et al. Citation2000) were randomized double-blind studies, two (Ziogos et al. Citation2010, Mivumbi et al. Citation2014) were randomized single-blind studies and four (Noyes et al. Citation1998, Jyothi et al. Citation2010, Zhang et al. Citation2010, Fang Citation2021) were described as RCTs. We assessed the included studies for risk of bias according to the Cochrane Handbook. Risk of bias of eligible studies is presented in and .
Figure 2. Risk of bias summary.
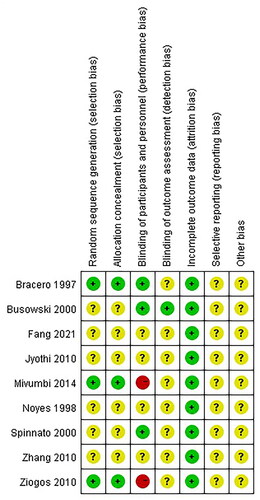
Figure 3. Risk of bias graph.
Main outcomes
P2+ vs C1&C2-outcome1: endometritis
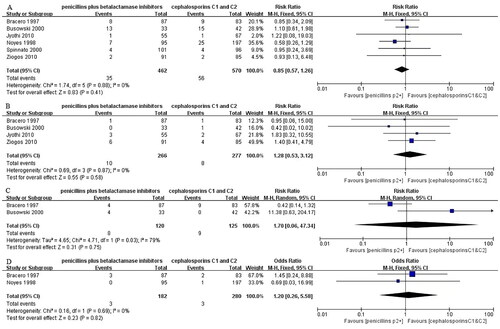
Endometritis was reported in six studies (Bracero Citation1997, Noyes et al. Citation1998, Busowski et al. Citation2000, Spinnato et al. Citation2000, Jyothi et al. Citation2010, Ziogos et al. Citation2010) with 1032 women were included in the meta‐analysis. There was no significant difference between groups for post-cesarean endometritis (RR 0.85, 95% CI 0.57–1.26, I2=0.0%) ().
Figure 4. Forest plots of the incidence of endometritis (A), wound infection (B), urinary tract infection (C) and maternal rashes (D) comparing P2+ with C1&C2.
P2+ vs C1&C2-outcome2: wound infection
Wound infection was reported in four studies (Bracero Citation1997, Busowski et al. Citation2000, Jyothi et al. Citation2010, Ziogos et al. Citation2010) involving 543 women were included in the meta-analysis. There was no evident difference between groups concerning postoperative wound infection (RR 1.28, 95% CI 0.53–3.12, I2=0.0%) ().
P2+ vs C1&C2-outcome3: urinary tract infection
Urinary tract infection was reported in two studies (Bracero Citation1997, Busowski et al. Citation2000) involving 245 women were included in the meta‐analysis. There was no clear difference in postoperative urinary tract infection between groups (RR 1.70, 95% CI 0.06–47.34, I2=79%) ().
P2+ vs C1&C2-outcome4: febrile morbidity
Only one RCT (Bracero Citation1997) reported the incidence of febrile morbidity in pregnant women. There was no important difference between groups regarding post-cesarean febrile morbidity (RR 0.95, 95% CI 0.32–2.84).
P2+ vs C1&C2-outcome5: maternal rashes
Maternal rashes was reported in two studies (Bracero Citation1997, Noyes et al. Citation1998) involving 462 women were included in the meta‐analysis. There was no significant difference for postpartum rashes between P2+ and C1&C2 (RR 1.20, 95% CI 0.26–5.58, I2=0.0%) ().
P2 vs C1&C2-outcome1: endometritis
Endometritis was reported in two studies (Spinnato et al. Citation2000, Mivumbi et al. Citation2014) involving 329 women were included in the meta-analysis. There was no significant difference between groups concerning post-cesarean postoperative endometritis (RR 3.22, 95% CI 0.45–22.89, I2=64%) ().
Figure 5. Forest plots of the incidence of endometritis (A), febrile morbidity (B) and wound infection (C) comparing P2 with C1&C2.
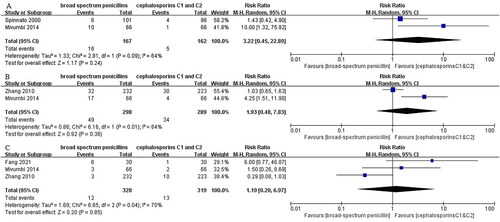
P2 vs C1&C2-outcome2: febrile morbidity
Febrile morbidity was reported in two studies (Zhang et al. Citation2010, Mivumbi et al. Citation2014) involving 329 women were included in the meta‐analysis. There was no evident difference between groups for postoperative febrile morbidity (RR 1.93, 95% CI 0.48–7.83, I2=84%) ().
P2 vs C1&C2-outcome3: wound infection
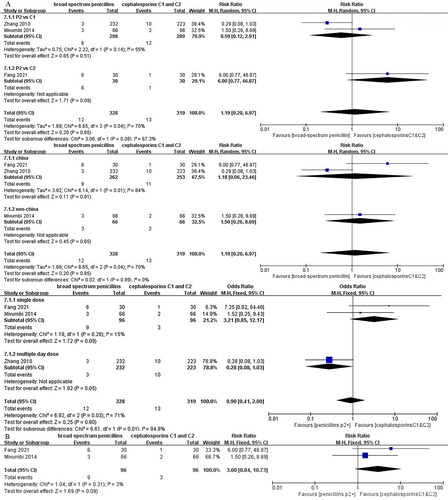
Wound infection was reported in three studies (Zhang et al. Citation2010, Mivumbi et al. Citation2014, Fang Citation2021) involving 647 women were included in the meta-analysis. There was no evident difference in postoperative wound infection between groups (RR 1.19, 95% CI 0.20–6.97, I2=70%) (). Owing to the heterogeneity, subgroup analyses were carried out according to the subclasses of cephalosporins, region and dosage regimen (). A forest plot was obtained after the removal of one article from heterogeneous sources ().
Figure 6. Subgroup analysis of the incidence of wound infection comparing P2 with C1&C2 according to subclasses of cephalosporins, region, dosage regimen (A) and a forest plot was obtained after the removal of one article from heterogeneous sources (B).
P2 vs C1&C2-outcome4: urinary tract infection
Only one RCT (Mivumbi et al. Citation2014) reported the incidence of urinary tract infection in pregnant women. There was no important difference between groups in postoperative urinary tract infection (RR 9.00, 95% CI 0.49–163.90).
P2 vs C1&C2-outcome5: length of postoperative hospitalization
Only one RCT (Mivumbi et al. Citation2014) reported length of postoperative stay in pregnant women. An increase was observed regarding length of postoperative stay in women who received P2 to C1 (MD 1.50, 95% CI 0.54–2.46).
Discussion
During cesarean section, causative agents that colonize the vagina and cervix may be transferred into the uterine cavity. Postoperative uterine tissue trauma, bleeding and exudate are also conducive to the generation of pathogens. Additionally, the surgical procedure changes the normal bacterial flora of the genital tract, resulting in an imbalance of the ratio of anaerobes to aerobes, which can lead to maternal infections when the postoperative immunity is decreased. Therefore, the use of prophylactic antibiotics is recommended for all patients undergoing cesarean section. Clinical research practice has indicated (Committee on Practice Bulletins-Obstetrics Citation2018) that there is no significant difference between C1&C2 in reducing the post-cesarean infections, and a single dose regimen is usually recommended.
The most common pathogens isolated from wound infection included Ureaplasma, Staphylococcus and Enterococcus, these can contaminate the myometrium, uterine blood vessels and lymphatic vessels, leading to infections including endometritis during surgery (Jaiyeoba Citation2012). C1&C2 have been widely used as preventive measures in obstetrics and gynecology surgery. However, they are naturally resistant to Enterococcus but stable to the betalactamase-producing Staphylococci (Bratzler et al. Citation2013, García-Solache and Rice Citation2019). It is reported that Enterococcus are the most common pathogens in cases of endometritis following cephalosporins prophylaxis (Newton and Wallace Citation1998). Compared with C1&C2, P2 is effective against Enterococcus and other gram-negative bacteria, but not against Staphylococci. P2+ have a broader antimicrobial spectrum than C1&C2 and are active against gram-positive, gram-negative and anaerobic bacteria, including S.aureus, Enterococci, Streptococci, many Enterobacterales and Bacteroides spp. The aim of the present analysis was to evaluate the efficacy of P2/P2+ which are routinely used clinically vs C1&C2 which are the first choices as prophylactic antibiotics during cesarean delivery.
Cesarean section is the most important risk factor for postpartum endometritis (Olsen et al. Citation2010). The incidence of postoperative endometritis as high as 70% before prophylactic antibiotic therapy became standard practice (Pierson et al. Citation2018). This was especially common in pregnant women with high risk factors of infection, such as rupture of membranes, excessive vaginal examinations before cesarean section, maternal anemia, obesity and poor hygiene, the use of prophylactic antibiotics can reduce the incidence of endometritis (Leth et al. Citation2009, Valent et al. Citation2017). The results revealed that there was no significant difference between P2/P2+ and C1&C2 for postoperative endometritis. In terms of P2 vs C1&C2, however, our results were inconsistent with a review by Cochrane (Alfirevic et al. Citation2010), which indicated that P2 were more effective than C1&C2 in preventing post-cesarean endometritis (RR 2.18, 95% CI 1.30 to 3.66). The source of difference owing to the inclusion of a recent RCT (Mivumbi et al. Citation2014), which reported a significant difference in the incidence of endometritis between the ampicillin and the cefazolin (15.2% vs 1.5%; p = .009), where cephalosporins were more effective in preventing endometritis.
Wound infection refers to infection of the skin and subcutaneous tissue at the surgical site that can complicate cesarean section (Scholz et al. Citation2021). In addition, wound infection at the surgical site will result in therapeutic antibiotic use, prolonged hospital stay, higher hospitalization costs and burden to health care system (Blumenfeld et al. Citation2015). The results showed that there was no difference between P2/P2+ and C1&C2 for postoperative wound infection. Concerning the comparison of P2+ vs C1&C2, there was only one study (Jyothi et al. Citation2010) comparing amoxycillin/clavulanic acid (AMX/CL) with cefazolin and there was no significant difference between the two groups in preventing wound infection. Although AMX/CL had activity against potential pathogens, it was not superior to cefazolin in preventing infection. Regarding the cost, the use of AMX/CL was more expensive. Furthermore, RCOG guidelines had indicated that AMX/CL is not recommended owing to the increased risk of necrotizing enterocolitis (National Collaborating Centre for Women's and Children's Health (UK) Citation2011). Because of a substantial heterogeneity in P2 group, the three articles, we according to the subclasses of cephalosporins, region, dosage regimen subgroup analyses, the results showed: (1) the comparison of P2 versus C1 remained heterogeneous, the comparison of P2 versus C2 is too few to analyze, and the subclasses of cephalosporins may not have been a source of heterogeneity; (2) the region was not a source of heterogeneity; (3) the studies of Mivumb et al. (Citation2014) and Fang (Citation2021) were single-dose regimens, while only one study (Zhang et al. Citation2010) was a multiple-day dose regimen. Depending on the results, the dosage regimen may be a source of heterogeneity. In support of our hypothesis, the study of Zhang was removed, leaving two studies with homogeneity. We conducted a meta-analysis on the remaining two articles (). Although there was no statistical difference, C1&C2 were slightly superior to P2 in preventing wound infection (RR 3.00, 95% CI 0.84–10.73, I2=3.0%, p = .09). At present, it is generally accepted that a single-dose regimen is better utilized for prevention.
The results showed that there were no differences between the P2/P2+ and C1&C2 for preventing post-cesarean urinary tract infection and febrile morbidity. Concerning postpartum urinary tract infection, in addition to the prophylactic antibiotics, post-cesarean bacteriuria may be further reduced by avoiding routine catheterization.
In terms of safety, two articles (Bracero Citation1997, Noyes et al. Citation1998) reported the events of maternal rashes, there was no evident difference between groups regarding antibiotic-related rashes. Three patients were found in the ampicillin/sulbactam group and one in the cefotetan group. Patients developed a rash that resolved following two doses of diphenhydramine hydrochloride. Based on the available evidence, the safety of drugs in each group was good. However, we have no data on late infections (up to 30 days) in the mother, which is important gap in the evidence that warrant further investigate.
Intrapartum antibiotics exposure may adversely affect the newborn’s developing immune system and microbiome. Studies have shown that antibiotics can cross the placenta and impact the newborn even short courses of intrapartum antibiotics (Zachariassen et al. Citation2016). In perioperative animal models, O’Connor’s et al. (Citation2021) team observed that early life exposure to maternal antibiotics (a single, low-dose penicillins) led to persistent alterations in anxiety, sociability and cognitive behaviors. They suggest that change in the gut microbiome is a potential mechanism for behavioral and physiological changes. Additionally, antibiotics in the perinatal period may be a factor that contributes to the association of cesarean delivery with childhood infection, allergy, inflammatory bowel disease and respiratory problems (Stinson et al. Citation2017, Auger et al. Citation2021). This evidences support the view that there are potential long-term detrimental consequences of maternal antibiotic use in the perinatal period. Nevertheless, unfortunately, no neonatal adverse effects nor any longer-term effects on children were reported in the included studies, we suggest that this information needs to be assessed by collecting long-term data. So far, there is relatively little research in this area, these are important evidence for evaluating antibiotic safety that warrant further research.
Limitations of this analysis: (1) some of the studies lacked information on study design which may have increased the risk of deviation; (2) some outcome indicators were reported in only one study that was not available for meta-analysis; (3) earlier trials in this study administered antibiotics at or immediately after the umbilical cord clamping, with a difference in timing from the currently supported administration prior to skin incisions, so the results may influence the recommendations for prophylaxis.
Conclusions
This meta-analysis included relatively new, comprehensive studies that provide a more appropriate recommendation for the prophylactic use of antibiotics during cesarean section. P2/P2+ and C1&C2 may have similar efficacy in the prevention of post-cesarean infections. P2 such as ampicillin and C1&C2 are good choices as prophylactic antibiotics for cesarean section, they were found to be equally effective, safe and inexpensive. However, the use of a wider spectrum of antimicrobials, including ampicillin/sulbactam, was not superior to the narrower spectrum C1&C2, and may promote antimicrobial resistance. Impact on newborns need to be assessed through the collection of long-term data and the late maternal infections warrants further study, which are important evidence for assessing antibiotic safety.
Authors’ contributions
Qianqian Song: project development, data collection, data analysis, manuscript writing. Jingjing Yan: project development, data collection, data analysis. Na Bu: project development, revision of the manuscript. Ying Qian: revision of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data in relation to this study are presented in this manuscript.
Additional information
Funding
References
- Abdel Jalil, M.H., et al., 2017. Surgical site infections following caesarean operations at a Jordanian teaching hospital: frequency and implicated factors. Scientific Reports, 7 (1), 12210.
- Alfirevic, Z., Gyte, G.M., and Dou, L., 2010. Different classes of antibiotics given to women routinely for preventing infection at caesarean section. Cochrane Database of Systematic Reviews, 6 (10), CD008726.
- Auger, N., et al., 2021. Association of caesarean delivery with childhood hospitalization for infections before 13 years of age. Journal of Pediatrics., 231, 178–184.
- Blumenfeld, Y.J., et al., 2015. Risk factors for prolonged postpartum length of stay following caesarean delivery. American Journal of Perinatology, 32 (9), 825–832.
- Bracero, L.A., 1997. Ampicillin/sulbactam versus cefotetan for the prevention of infection following caesarean delivery in high-risk patients: a randomized double-blind trial. Gynecologic and Obstetric Investigation, 44 (1), 21–25.
- Bratzler, D.W., et al., 2013. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surgical Infections, 14 (1), 73–156.
- Busowski, J.D., et al., 2000. Antibiotic prophylaxis for caesarean delivery: a randomized trial of cefotetan, ampicillin-sulbactam and ciprofloxacin. Prenatal and Neonatal Medicine, 5, 357–362.
- Committee on Practice Bulletins-Obstetrics. 2018. ACOG practice bulletin no. 199: use of prophylactic antibiotics in labor and delivery. Obstetrics & Gynecology, 132 (3), e103–e119.
- Conroy, K., et al., 2012. Infectious morbidity after caesarean delivery: 10 strategies to reduce risk. Reviews in Obstetrics and Gynecology, 5 (2), 69–77.
- Dervisoglou, A., et al., 2006. The value of chemoprophylaxis against Enterococcus species in elective cholecystectomy: a randomized study of cefuroxime vs ampicillin-sulbactam. Archives of Surgery, 141 (12), 1162–1167.
- Fang, C.F., 2021. Study on the effect of cefuroxime sodium in anti infection treatment of caesarean section. Capital Food Medicine, 28 (8), 74–76.
- García-Solache, M. and Rice, L.B., 2019. The enterococcus: a model of adaptability to its environment. Clinical Microbiology Reviews, 32 (2), e00058–e00118.
- Gyte, G.M., Dou, L., and Vazquez, J.C., 2014. Different classes of antibiotics given to women routinely for preventing infection at caesarean section. Cochrane Database of Systematic Reviews, 2014 (11), CD008726.
- Jaiyeoba, O., 2012. Postoperative infections in obstetrics and gynecology. Clinical Obstetrics and Gynecology, 55 (4), 904–913.
- Jyothi, S., et al., 2010. Antibiotic prophylaxis for hysterectomy and caesarean section: amoxicillin-clavulanic acid versus cefazolin. Journal of Obstetrics and Gynecology of India, 60 (5), 419–423.
- Lamont, R.F., et al., 2011. Current debate on the use of antibiotic prophylaxis for caesarean section. BJOG, 118 (2), 193–201.
- Leth, R.A., et al., 2009. Risk of selected postpartum infections after caesarean section compared with vaginal birth: a five-year cohort study of 32,468 women. Acta Obstetricia et Gynecologica Scandinavica, 88 (9), 976–983.
- Mivumbi, V.N., et al., 2014. Prophylactic ampicillin versus cefazolin for the prevention of post-caesarean infectious morbidity in Rwanda. International Journal of Gynaecology & Obstetrics, 124 (3), 244–247.
- Mutic, A.D., et al., 2017. The postpartum maternal and newborn microbiomes. MCN: The American Journal of Maternal/Child Nursing, 42 (6), 326–331.
- National Collaborating Centre for Women’s and Children’s Health (UK), 2011. Caesarean section. London: RCOG Press.
- National Health and Family Planning Commission of China, 2015. Guidelines for clinical application of antimicrobial therapy. People’s Medical Publishing House.
- Newton, E.R. and Wallace, P.A., 1998. Effects of prophylactic antibiotics on endometrial flora in women with postcaesarean endometritis. Obstetrics & Gynecology, 92 (2), 262–268.
- Noyes, N., et al., 1998. Incidence of postpartum endomyometritis following single-dose antibiotic prophylaxis with either ampicillin/sulbactam, cefazolin, or cefotetan in high-risk caesarean section patients. Infectious Diseases in Obstetrics and Gynecology, 6 (5), 220–223.
- Obstetrics and Gynecology Pharmacy Group, Hospital Pharmaceutical Committee, Chinese Pharmaceutical Association, et al., 2021. Recommendations for clinical prophylactic antibiotics in obstetrics and gynecology during perioperative period. Chinese Pharmaceutical Journal, 56 (3), 250–256.
- O’Connor, R., et al., 2021. Maternal antibiotic administration during a critical developmental window has enduring neurobehavioural effects in offspring mice. Behavioural Brain Research, 404, 113156.
- Olsen, M.A., et al., 2010. Risk factors for endometritis after low transverse caesarean delivery. Infection Control & Hospital Epidemiology, 31 (1), 69–77.
- Pierson, R.C., et al., 2018. A review of post-caesarean infectious morbidity: how to prevent and treat. Journal of Obstetrics and Gynaecology, 38 (5), 591–597.
- Scholz, R., et al., 2021. A multifaceted surgical site infection prevention bundle for caesarean delivery. American Journal of Perinatology, 38 (7), 690–697.
- Spinnato, J.A., et al., 2000. Antibiotic prophylaxis at caesarean delivery. Journal of Maternal-Fetal Medicine, 9 (6), 348–350.
- Stinson, L.F., Payne, M.S., and Keelan, J.A., 2017. Planting the seed: origins, composition, and postnatal health significance of the fetal gastrointestinal microbiota. Critical Reviews in Microbiology, 43 (3), 352–369.
- Stinson, L.F., Payne, M.S., and Keelan, J.A., 2018. A critical review of the bacterial baptism hypothesis and the impact of caesarean delivery on the infant microbiome. Frontiers in Medicine, 5, 135.
- Valent, A.M., et al., 2017. Effect of post-caesarean delivery oral cephalexin and metronidazole on surgical site infection among obese women: a randomized clinical trial. Journal of the American Medical Association, 318 (11), 1026–1034.
- Van Schalkwyk, J. and Van Eyk, N., 2017. SOGC reaffirmed guidelines no.247-antibiotic prophylaxis in obstetric procedures. Journal of Obstetrics and Gynaecology Canada, 39 (9), e293–e299.
- Zachariassen, G., et al., 2016. The half-life and exposure of cefuroxime varied in newborn infants after a caesarean section. Acta Paediatrica, 105 (9), 1074–1078.
- Zhang, X.J., et al., 2010. Resonable selection of antibiotics during perioperative period in caesarean section. Journal of Practical Obstetrics and Gynecology, 26 (2), 128–130.
- Ziogos, E., et al., 2010. Ampicillin/sulbactam versus cefuroxime as antimicrobial prophylaxis for caesarean delivery: a randomized study. BMC Infectious Disease, 10, 341.