

Introduction
Endometriosis is an estrogen-sensitive gynecological disorder with lasting implications for many women’s fertility, body health and general quality of life (Smarr et al. Citation2016). It occurs in about 10% of women of reproductive age, and this rate rises to 50% in infertile people (Goksever Celik et al. Citation2019). Extrapelvic endometriosis most commonly develops in the abdominal wall and rarely in the perineum, umbilicus, pleura, kidneys, lungs and liver (Chen et al. Citation2012).
The etiopathogenesis of subcutaneous endometriosis is hypothesized to occur after abdominal or pelvic surgical procedures as result of the implantation of endometrial tissue into the skin (Raffi et al. Citation2019). The implantation of endometrial cells into cutaneous sites during surgical procedures creates cells that proliferate and shed during the menstrual cycle, behaving similarly to endometrial cells of the uterus. Its incidence is 0.03–0.4%. The clinical presentation varies according to the depth and localization of the lesion. It may not always be symptomatic, making the diagnosis challenging. However, the most common symptom is cyclic pain, and the patient’s history of abdominal surgery may be a clue for the correct diagnosis (Ozel et al. Citation2012).
Nonsteroidal anti-inflammatory drugs can be used for pain management. The hormonal therapy includes the use of GnRh, danazol and oral contraceptives. The recurrence rate is very rare with complete surgical excision. It increases if incomplete excision is performed (Purvis and Tyring Citation1994)
In this case report, two cases with a history of previous cesarean section and a body mass index of above 30 were presented, in whom excision was performed by injecting methylene blue into the lesion using preoperative ultrasound guidance to provide complete and easy surgical resection of subcutaneous endometriotic foci.
Case 1
A 36-year-old patient applied with the complaint of severe pain in the cesarean section incision area during menstrual periods. The patient’s BMI was 36.73, and she had a history of two cesarean sections and three curettages. The physical examination revealed no mass lesion with palpation on the cesarean scar line. A pelvic MRI was performed after detecting a suspicious endometriotic nodule of approximately 25 mm in the suprapubic region close to the rectus muscle in the transabdominal ultrasound. The MRI result was reported as ‘a soft tissue lesion (endometriosis) with a 26 mm diameter, slightly irregular contour, hypointense in T1AG, markedly hypointense in T2AG, showing weak diffusion restriction, adjacent to the right rectus abdominis muscle at the suprapubic level’, and endometriotic nodule excision was planned for the patients.
Case 2
A 26-year-old patient presented to the outpatient clinic with severe dysmenorrhea and pain in the cesarean scar region during menstrual periods. The patient had a normal physical examination and a BMI of 32. After a 13 × 8.5 mm lesion with irregular contours on the left side of the incision line was observed in the superficial tissue USG, excision of the endometriotic nodule was planned.
A novel technique
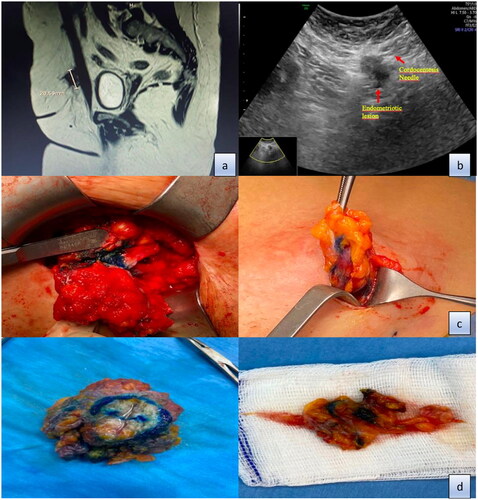
After cleaning the suprapubic regions of the patients and covering them with sterile drapes just before starting the operation, the lesion was reached with a 20 gauge cordocentesis needle under ultrasound guidance (). The procedure was terminated by injecting approximately 2 ccs of methylene blue into the central part of the lesion, and the patients were taken into operation. In the operations, approximately 3 cm incision was made to exclude the skin-subcutaneous fat tissue, endometriotic foci stained with methylene blue were reached in the adjacency of the rectus abdominis, and the lesion was excised containing 1 cm of intact tissue around it (). Since the foci were observed to invade the fascia during excision, the fascia adjacent to the associated rectus abdominis was also excised, and the resulting fascia defect was primarily repaired. Afterward, the operations were terminated after suturing subcutaneous tissue and skin. No intraoperative complications developed. No recurrence or complication was observed in the one-year follow-up of the patients. Pathology results of both patients were reported as endometriosis externa.
Figure 1. (a) MRI imaging of subcutaneous endometriotic lesion. (b) Administering methylene blue to the lesion with the help of a cordocentesis needle under the guidance of transabdominal USG. (c) Detection of lesions stained with methylene blue. (d) Image of endometriotic lesions after removal with 1 cm of intact tissue.
Discussion–conclusion
Subcutaneous endometriosis is a dynamic but not fully understood issue that needs a multidisciplinary approach. Its incidence has increased due to increased obstetric and gynecological procedures. The clinical presentation is a palpable mass and local cyclic pain in the abdominal wall or cesarean scar. Imaging techniques such as ultrasound or magnetic resonance may be helpful in diagnosis, but a definitive diagnosis is based on the postoperative histopathological report. In a 2017 meta-analysis including 11 studies, the combined relative risk of endometriosis was reported as 0.67 (95% CI: 0.53, 0.84) for each 5 kg/m2 increase in current body mass index, with statistically significant heterogeneity in studies (p < .001). This study suggested that higher body mass index may be associated with lower risk of endometriosis (Liu and Zhang Citation2017). Treatment of endometriosis can be medical, surgical, or combined therapy. Oral contraceptives and progestins combined with various routes of administration are generally safe, effective and well-tolerated methods in treating endometriosis and should constitute the first-line treatment in symptomatic women who do not want to have children (Vercellini et al. Citation2009). It is known that distant lesions usually lose their hormonal receptors and do not respond to medical treatment (Ueki Citation1991). Hormonal therapy has been shown to provide reasonable symptom control in some case reports (Mignemi et al. Citation2012). Surgical removal of the implant is currently considered the most effective method known (Carsote et al. Citation2020).
To the best of our knowledge, no similar technique has been used in the surgical removal of subcutaneous endometriotic nodules before in the literature. Intraoperatively detecting and completely excising deeply located subcutaneous endometriotic nodules in patients with high BMI is challenging and time-consuming. The prolongation of the operation period also brings many complications. We think that our technique is very useful in shortening the operation time and in the complete removal of the endometriotic focus with intact surgical margins, especially in patients with high BMI.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Carsote, M., et al., 2020. Abdominal wall endometriosis (a narrative review). International Journal of Medical Sciences, 17 (4), 536–542.
- Chen, N., et al., 2012. The clinical features and management of perineal endometriosis with anal sphincter involvement: a clinical analysis of 31 cases. Human Reproduction (Oxford, England), 27 (6), 1624–1627.
- Goksever Celik, H., et al., 2019. Abdominal wall endometriosis: a monocentric continuous series and review of the literature. Journal of Endometriosis and Pelvic Pain Disorders, 11 (2), 95–101.
- Liu, Y. and Zhang, W., 2017. Association between body mass index and endometriosis risk: a meta-analysis. Oncotarget, 8 (29), 46928–46936.
- Mignemi, G., et al., 2012. A case report of nasal endometriosis in a patient affected by Behcet’s disease. Journal of Minimally İnvasive Gynecology, 19 (4), 514–516.
- Ozel, L., et al., 2012. Abdominal wall endometriosis in the cesarean section surgical scar: a potential diagnostic pitfall. The Journal of Obstetrics and Gynaecology Research, 38 (3), 526–530.
- Purvis, R.S. and Tyring, S.K., 1994. Cutaneous and subcutaneous endometriosis. Surgical and hormonal therapy. The Journal of Dermatologic Surgery and Oncology, 20 (10), 693–695.
- Raffi, L., et al., 2019. Cutaneous endometriosis. International Journal of Women’s Dermatology, Dec5 (5), 384–386.
- Smarr, M.M., Kannan, K., and Buck Louis, G.M., 2016. Endocrine disrupting chemicals and endometriosis. Fertility and Sterility, 106 (4), 959–966.
- Ueki, M., 1991. Histologic study of endometriosis and examination of lymphatic drainage in and from the uterus. American Journal of Obstetrics and Gynecology, 165 (1), 201–209.
- Vercellini, P., et al., 2009. Endometriosis: current therapies and new pharmaco-logical developments. Drugs, 69 (6), 649–675.