

Abstract
This aim of this study was to investigate maternal hematological laboratory parameters of term infants before birth diagnosed with asphyxia compared to mothers of healthy term infants and predict asphyxia by these parameters. This study was conducted on 109 and 192 mothers of the fetus with asphyxia and healthy, respectively. Laboratory parameters of complete blood count, including PDW (platelet distribution width), PCT (procalcitonin) and NLR (neutrophil/lymphocyte ratio), were recorded before birth from pregnant women. PDW and basophil counts were significantly higher in the asphyxia group than healthy group (p: .000). The cut-off level of 19.425 accurately predicted the occurrence of asphyxia (AUC = 0.724 (95% confidence interval 0.65–0.78), p = .000). Basophil count could predict asphyxia, especially the cut-off level of> 0.15(10³/μL) (AUC = 0.67) (95% confidence interval 0.60–0.74, p = .000). To predict asphyxia before labor, a cheap and routine test of PDW can be used after more research in this area.
What is already known on this subject? Asphyxia is still an unsolved problem in neonatal mortality and morbidity, and it is seen in babies of mothers who carry some risks during pregnancy (such as multiple pregnancy, baby of mother with preeclampsia, meconium aspiration, diabetes); however, it is known that it is a subject that is still not fully understood as it can also occur as a result of labor that does not have any risk factors and goes well.
What do the results of this study add? In term fetuses without risk factors, it can be predicted to a certain extent whether the fetus will be diagnosed with asphyxia from the hemogram test that can work from the blood of the mother before birth.
What are the implications of these findings for clinical practice and/or further research? In clinical practice, asphyxia can be estimated with a cheap and simple test, without any extra examination, by looking at the routine blood tests taken from the mother before going into labor.
IMPACT STATEMENT
Introduction
Although delivery in hospitals and quality pregnancy follow-up has increased today, hypoxic-ischemic encephalopathy (HIE)/perinatal asphyxia is still not over in the world. Twenty-five percent of neonatal deaths are caused by perinatal asphyxia (Liu et al. Citation2016). It is still a significant problem, especially for women during pregnancy from disadvantaged homes. However, no test can detect prenatal/intrauterine hypoxia and alert us early in the delivery process. In addition, due to the course of birth of two fetuses with the same characteristics, unpredictable fetal outcomes may occur.
Known risk factors for perinatal asphyxia include maternal anemia, high parity, interventional deliveries and shoulder dystocia (Liljestrom et al. Citation2018). In addition, preterm premature rupture of membranes, amniotic meconium fluid and prolonged labor are among the possible risks. Although neonatal encephalopathy is associated with birth asphyxia, no intrapartum or acute peripartum problems were detected in some newborns with encephalopathy (McIntyre et al. Citation2021). Therefore, the ACOG and AAP defined neonatal asphyxia according to the following criteria: intrapartum or peripartum () (American College of Obstetricians and Gynecologists Citation2014).
Table 1. The definition criteria of neonatal asphyxia.
Still, some of the etiology of fetal asphyxia is unknown. Especially a term fetus, without any risk factors and reassuring labor follow-up sometimes result in asphyxia. In these conditions, whether an unknown intrauterine asphyxia etiology is a question mark. False reactive non-stress tests occur at a rate of four to five per 1000 fetuses in the largest studies (Umana and Siccardi Citation2022). A reactive non-stress test can occur, but the fetal outcome may be asphyxia. So other factors may be involved, and another diagnostic tool may be needed. In the literature, especially placental inflammation was found to be a reason.
It was the first time babies with HIE came from low socioeconomic families compared to healthy term control groups in West Australia and were subsequently confirmed worldwide (Badawi et al. Citation1998). Some studies argue that the cause of HIE in infants of low socioeconomic status mothers may be due to placental inflammation (Vik et al. Citation2018).
Early neutrophilia has been linked to larger infarct sizes on MRI. Early neutrophil infiltration is crucial to the injury process in a newborn animal model of inflammatory mediators hypoxic-ischemic brain injury (Buck et al. Citation2008). In the literature about ischemic lesions of stroke patients, there was an association found between serum inflammatory biomarkers and prognosis after endovascular treatment (Lattanzi et al. Citation2021). Also, the platelet/lymphocyte ratio was used in a study to predict the mortality rate in acute cardiogenic pulmonary edema (Demir et al. Citation2018). The neutrophil/lymphocyte ratio also influences the prognosis of acute intracerebral hemorrhage (Lattanzi et al. Citation2018). Also, this ratio is early in predicting bacteremia in emergency settings (Jager Citation2010). No studies predict fetal intrauterine hypoxia before birth from the maternal hematological tests of maternal inflammation, according to the literature.
In our study, we aimed to study maternal hematological laboratory parameters of term infants diagnosed with neonatal encephalopathy compared to mothers of healthy term infants and investigated whether there was actual inflammation in mothers of infants with HIE.
Material and method
The newborns with a diagnosis of stage 3 hypoxic-ischemic encephalopathy(HIE) with the ICD code of asphyxia, who were hospitalized in the neonatal intensive care unit of Şanliurfa Training and Research Hospital between January 2017 and January 2022, were found and the complete blood count parameters of their mothers when they entered labor were recorded.
There were two groups as group 1 (asphyxia group) and group 2 as control group. Group 2, as the control group, were selected retrospectively with simple random sampling from the babies who were followed up with their mothers after birth as term, healthy babies without any anomaly, and the demographic characteristics of the mothers, baby’s gender, birth weight, type of birth and presence of risk factors before birth were similar to group 1 and the maternal hematological parameters before the birth were recorded. Our study was a retrospective study consisting of asphyxia and control groups. Group 1 consisted of asphyxia fetuses selected according to the study criteria from the neonatal intensive care unit as stage 3 HIE according to (Mrelashvili et al. Citation2020) Sarnat and Sarnat classification, while group 2, the control group, term babies selected according to the study criteria from the mother side, healthy babies without a fetal anomaly.
Inclusion criteria for the study; infants who were born at ≥37 gestational weeks in our hospital and hospitalized in the neonatal intensive care unit with the diagnosis of stage 3 HIE (Mrelashvili et al. Citation2020), and mothers whose maternal complete blood count before birth and files were available. The definition of neonatal asphyxia is taken from the ACOG and AAP, as mentioned above.
Exclusion criteria were the babies born at and less than 37 weeks, lethal fetal anomaly and congenital infections, outdoor births and births with breech presentation. Pregnant with hematological disorders such as myeloproliferative disorders and Hodgkin disease and infectious/inflammatory disorders such as colitis, pneumonia, acute infection, steroid usage and psychological diseases were excluded from all groups due to the effect of hematological parameters. Asphyxia caused by interventional deliveries, shoulder dystocia, preterm premature rupture of membranes, prolonged labor and acute intrapartum event as uterine rupture or umbilical cord prolapse were excluded from the asphyxia group.
Anticoagulated whole blood from all groups was processed on Sysmex XE2100 [TOA Medical Electronics, Kobe, Japan], Advia 2120 (Bayer Diagnostics, Tarritown, NY, USA), DXH800 (Beckman Coulter, Miami, FL USA), Cell-Dyn Sapphire (Abbott Diagnostics Santa Clara, CA, USA) for the determination of the complete blood cell counts and differential counts of leukocytes. In laboratory parameters, hemogram, hematocrit, mean corpuscular volume (MCV), red cell width(RDW), platelet corpuscular volume(PCV), platelet distribution width(PDW), neutrophil, lymphocyte, basophil and eosinophil counts, neutrophil/lymphocyte ratio and platelet/lymphocyte ratio was investigated.
The data were evaluated in the SPSS 26.0 statistics program, and the percentages were calculated for the mean, standard deviations and categorical data. The normal distribution of values was examined using visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov test). Student’s T-Test was used for the variables with normal distribution to evaluate the statistical significance between the two independent groups. While the t-test was used to compare means between groups, the chi-square test was used for categorical data. If the values were not normally distributed, non-parametric tests were used. Correlation analysis was performed for the significant means. ROC curves were drawn. For the level of significance, p < .05 was accepted.
Permission was obtained from the Harran University Ethics Committee for the study permit (HRU/22.09.09).
Results
A total of 302 patients, 109 asphyxia (group 1) and 192 healthy (group 2) were included in this study. In our hospital, patients with low socioeconomic status and Syrians living in the province of Şanliurfa were giving birth, and the patients with the low socioeconomic group were significantly higher in the asphyxia group than in the healthy group(p<.05).
Mean maternal age in asphyxia and healthy groups were 25.80 ± 6.82 and 26.80 ± 6.01 years, respectively. Mean gravida in asphyxia and healthy groups were; 2.86 ± 2.21 and 3.84 ± 2.36, and mean birth weight was 3246.37 ± 435.57 and 3222.51 ± 373.64 g. According to mother age, gravida and birth weight, no significant differences between groups were discovered (p>.05).
Ninety out of 302 patients had nulliparous, and there was a significant relationship between asphyxia and primiparity (p:.00). In the asphyxia group, there were considerably more male newborns than in the healthy group (p: .03). Compared to the healthy group, the hypoxia group had a significantly higher rate of vaginal births (p:.01). While nine patients in the asphyxia group had a risk factor of preeclampsia, diabetes, epilepsy and meconium amniotic fluid, in the healthy group, there were five patients (p>.05).
Hematological parameters according to groups are in . According to these hematologic parameters, PDW and basophil count were higher in the asphyxia group (p:.000). PDW and basophil count values were higher in the asphyxia group than in the healthy group, regardless of parity, maternal age and birth weight.
Table 2. Hematological parameters according to the study groups.
Table 3. Area under the curve for PDW and basophil for asphyxia group.
Discussion
Our hospital is a tertiary center for obstetrics and newborns and is the 1st in Turkey in the number of births, with a total number of births close to 36.000 per year. Between January 2017 and January 2022, 152.695 deliveries occurred in our hospital. Between 109 and 109 newborns who were intubated with the diagnosis of stage 3 asphyxia in the newborn were included in the study. All of these newborns had therapeutic hypothermia due to the suitability of newborn hypothermia treatment in asphyxia (Mosalli Citation2012).
Considering the newborns hospitalized with the diagnosis of asphyxia in our study, it is not a critical prenatal risk factor in infants and consists of term babies. Our study aims to determine whether these babies will have asphyxia, one of the markers in the mother’s blood, and to deliver by cesarean section if necessary. Because as will be evident from our results, the number of babies born with vaginal delivery in the asphyxia group is significantly different from the healthy group. Nevertheless, it should be discussed whether taking a cesarean section just because of asphyxia will save the situation. Because as we will talk about, some blood parameters were significantly different in the asphyxia group compared to the healthy group. In other words, some babies may have asphyxia before they are born.
Although maternal anemia is a risk factor for asphyxia in the literature [2], no significant difference was found in our study’s healthy and asphyxia groups. Due to the low socioeconomic level of the patients we live with, we keep hemoglobin levels at an optimal level until the time of delivery with iron supplement/transfusion required by our hospital and public health for maternal anemia during pregnancy follow-ups.
In our study, all of our patients came from low socioeconomic families. In some studies, it is argued that the cause of asphyxia in infants of low socioeconomic status mothers may be due to placental inflammation (Vik et al. Citation2018). Early neutrophilia has been linked to larger infarct sizes on MRI. Early neutrophil infiltration is crucial to the injury process in a newborn animal model of inflammatory mediators hypoxic-ischemic brain injury (Buck et al. Citation2008). No studies in the literature demonstrate a connection between fetal intrauterine hypoxia and maternal inflammation by complete blood count.
A study by Cappelletti et al. (Citation2016, p. 15) explained that this mentioned placental inflammation comes from histological chorioamnionitis, and neutrophil/lymphocyte ratio (NLR) can be a predictor of it. Regarding acute asphyxia, maternal NLR at delivery is more diagnostic than CRP. It can serve as a helpful marker in identifying histological chorioamnionitis without umbilical cord infection. According to NLR, there was no significant difference between the groups in our investigation. Despite this, in a study by Ozel et al. (Citation2020). 16, at a cut-off level of 5.14, NLR accurately predicted the occurrence of neonatal sepsis (AUC = 0.717 (95% confidence interval 0.610–0.824), p = .001) and in our study in both of groups mean NLR were 4.36 ± 3.02 and 4.28 ± 2.49 respectively. Although there was no difference between groups, these values were close to the level of inflammation. Due to our patients’ low socioeconomic status, maternal inflammation may be understandable by high NLR.
According to recent publications in the literature, platelets have been found to play a role in inflammation as well as hemostasis (Kurban et al. Citation2021). In patients with preterm labor caused by inflammation, it has been discovered that platelet activation indices such as MPV and PDW fluctuate more than in controls. In a study (Artunc Ulkumen et al. Citation2014), PDW values were higher in the preterm labor group than in the healthy group. The increased PDW levels, especially > 16.15, may alert the obstetrician to the risk of preterm delivery.
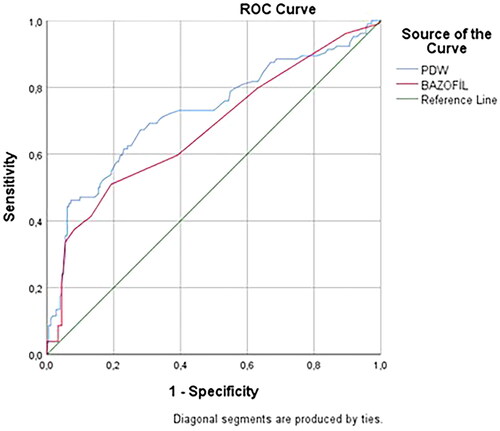
In our study, there was no difference according to MPV values, but PDW values were higher in the asphyxia group than in the healthy group. The cut-off level of 19.425 accurately predicted the occurrence of asphyxia (AUC = 0.724 (95% confidence interval 0.65–0.78), p = .000). PDW may be a good marker regardless of platelet count in asphyxia prediction.
Although the function of basophils is not fully known, new studies in the literature have shown that they are markers of inflammation. In our study, in the asphyxia group, basophil counts were higher than in the healthy group (p:.000). In addition, NLR values were both compatible with inflammation, and both patients were in the lower socioeconomic group; basophil counts could predict asphyxia, especially the cut- off the level of >0,15 (10³/μL) (AUC = 0.67) (95% confidence interval 0.60–0.74, p=.000) ().
This study is the first to predict asphyxia in term and risk-free newborns by using a cheap, routine blood test before labor. As the studies and this study show, an inflammation (placental/maternal systemic) starts in asphyxia before labor occurs. Animal studies could be done to explain the pathophysiology.
This study’s limitation is that the hospital population was of low socioeconomic status. Therefore, this study can be done in various groups of different populations.
In conclusion, more research is required despite PDW and basophil count that might seem to predict asphyxia in term and risk-free fetuses before labor.
Figure 1. ROC curve for PDW and basophil count in fetal asphyxia.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- American College of Obstetricians and Gynecologists, 2014. Neonatal encephalopathy and neurologic outcome, second edition report of the American College of Obstetricians and gynecologists’ Task Force on neonatal encephalopathy. Obstetrics & Gynecology, 123 (4), 896–901.
- Artunc Ulkumen, B., et al., 2014. Platelet distribution width (PDW): a putative marker for threatened preterm labour. Pakistan Journal of Medical Sciences, 30 (4), 745–748.
- Badawi, N., et al., 1998. Antepartum risk factors for newborn encephalopathy: the Western Australian case-control study. BMJ (Clinical Research Ed.), 317 (7172), 1549–1553.
- Buck, B.H., et al., 2008. Early neutrophilia is associated with volume of ischemic tissue in acute stroke. Stroke, 39 (2), 355–360.
- Cappelletti, M., et al., 2016. Inflammation and preterm birth. Journal of Leukocyte Biology, 99 (1), 67–78.
- Demir, M., et al., 2018. Platelet to lymphocyte ratio on admission and prognosis in patients with acute cardiogenic pulmonary edema. The Journal of Emergency Medicine, 55 (4), 465–471.
- Jager, C.P.C, et al., 2010. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Critical Care, 14 (5), R192.
- Kurban, Y., et al., 2021. Investigation of neutrophil/lymphocyte ratio and mean platelet volume in patients diagnosed with preterm labor. Paediatric Respiratory Reviews, 40, 39–43.
- Lattanzi, S., et al., 2018. Neutrophil-to-lymphocyte ratio improves outcome prediction of acute intracerebral hemorrhage. Journal of the Neurological Sciences, 387, 98–102.
- Lattanzi, S., et al., 2021. Systemic ınflammatory response ındex and futile recanalization in patients with ıschemic stroke undergoing endovascular treatment. Brain Sciences, 11 (9), 1164.
- Liljestrom, L., Wikstrom, A., and Jonsson, M., 2018. Obstetric emergencies as antecedents to neonatal hypoxic ischemic encephalopathy, does parity matter? Acta Obstetricia Et Gynecologica Scandinavica, 97 (11), 1396–1404.
- Liu, L., et al., 2016. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the sustainable development goals. Lancet, 388 (10063), 3027–3035.
- McIntyre, S., et al., 2021. Neonatal encephalopathy: focus on epidemiology and underexplored aspects of etiology. Seminars in Fetal & Neonatal Medicine, 26 (4), 101265.
- Mosalli, R., 2012. Whole body cooling for infants with hypoxic-ischemic encephalopathy. Journal of Clinical Neonatology, 1 (2), 101–106.
- Mrelashvili, A., et al., 2020. The Sarnat score for neonatal encephalopathy: looking back and moving forward. Pediatric Research, 88 (6), 824–825.
- Ozel, A., et al., 2020. How do platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio change in women with preterm premature rupture of membranes, and threaten preterm labour? Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 40 (2), 195–199.
- Umana, O.D. and Siccardi, M.A., 2022. Prenatal non-stress test. Treasure Island, FL: StatPearls.
- Vik, T., et al., 2018. The placenta in neonatal encephalopathy: a case control study. The Journal of Pediatrics, 202, 77–85 e3.