

Abstract
This study aimed to investigate the predictive value of coagulation, thromboelastography, stress response, and immune function indicators for the occurrence of deep venous thrombosis (DVT) following radical resection of cervical cancer and ovarian cancer. We conducted a prospective, single-centre, case-control study that included 230 cervical cancer patients and 230 ovarian cancer patients. In the testing cohort, the final predictive model for cervical cancer patients was: Logit(P)=9.365–0.063(R-value)−0.112(K value) +0.386(α angle)+0.415(MA)+0.276(FIB)+0.423(D-D)+0.195(IL-6)+0.092(SOD). For ovarian cancer patients, the final model was: Logit(P)= −2.846–0.036(R-value)-0.157(K value) +0.426(α angle) +0.172(MA) +0.221(FIB)+0.375(CRP) −0.126(CD4+/CD8+). In the validation cohort, these models exhibited good predictive efficiency, with a false-positive rate of 12.5% and a false-negative rate of 2.9% for cervical cancer patients, and a false-positive rate of 14.3% and a false-negative rate of 0% for ovarian cancer patients. In conclusion, the risk prediction models developed in this study effectively improve the predictive accuracy of DVT following radical resection of cervical and ovarian cancer.
Graphical Abstract
What is already known on this subject? Nowadays, surgery is currently the primary treatment for gynecological malignant tumours. However, prior to surgery, these tumours often create a hypercoagulable state, which increases the likelihood of deep vein thrombosis (DVT) following the procedure. Reports have shown that the incidence of DVT after surgery for ovarian cancer is the highest among gynecological malignant tumours, ranging from 13.6% to 27%, with lower extremity DVT being the most common. The occurrence of embolic detachment poses the greatest risk of DVT and can lead to fatal pulmonary embolism. Identifying the factors that influence the occurrence of DVT after gynecological malignant tumour surgery is crucial in order to take necessary preventive measures for patients with high-risk factors and reduce the incidence of DVT. This is of great significance in ensuring the quality of surgery and improving the postoperative quality of life for patients.
What do the results of this study add? This prospective, single-centre, case-control study was conducted to investigate the predictive value of coagulation, thromboelastography, stress response, and immune function indicators for the occurrence of deep venous thrombosis (DVT) following radical resection of cervical and ovarian cancer. This study included 230 cervical cancer patients and 230 ovarian cancer patients. Based on our findings, current risk prediction models that incorporate coagulation, thromboelastography, stress response, and immune function laboratory indicators have demonstrated the potential to improve the predictive accuracy of postoperative DVT in patients who have undergone radical resection of cervical and ovarian cancer.
What are the implications of these findings for clinical practice and/or further research? Our study found that the final two regression models had a prediction accuracy of 87.9% and 87.4% for postoperative DVT in patients with cervical and ovarian cancer, respectively, which is a significant improvement. Furthermore, both models demonstrated high specificity of 100%. In addition, the models continued to perform well in terms of predictive efficiency, with a false positive rate of 12.5% and a false negative rate of 2.9% for cervical cancer patients and a false positive rate of 14.3% and a false negative rate of 0% for ovarian cancer patients. Our models are effective in predicting the occurrence of DVT in patients with cervical and ovarian cancer following resection.
Impact statement
Introduction
Cervical cancer and ovarian cancer are among the most common types of tumours affecting the female reproductive system (Bhandari et al. Citation2022, Wang et al. Citation2021). These cancers have high incidence and fatality rates, posing a serious threat to the lives of female patients. Due to the complex anatomy and endocrine function of the female reproductive organs, symptoms of these cancers are often not apparent in the early stages of the disease (James et al. Citation2023). As a result, up to 70% of patients are diagnosed at an advanced stage (James and Georgopoulos Citation2023).
Currently, surgical treatment is the main approach for managing cervical and ovarian cancer, and tumour cell reduction is one of the most commonly used means (Mahasa et al. Citation2022; Saenger et al. Citation2004). To achieve satisfactory tumour reduction, surgery is usually expanded as much as possible, sometimes involving the whole abdominal cavity. Therefore, the incidence of postoperative complications and mortality rates are high (Mahasa et al. Citation2022). Several recent studies have examined the predictors of overall and severe complications following surgical treatment for gynecological cancer (D’Oria et al. Citation2022; Giannini et al. Citation2020). Deep venous thrombosis (DVT) is a common complication after tumour cell reduction (Yu et al. Citation2020), and it is associated with a higher risk of fatal pulmonary embolism, increased postoperative treatment costs and hospital stay, and adverse outcomes and quality of life (Cires-Drouet et al. Citation2022; Yasui et al. Citation2022). Recent research suggests that female patients who contract SARS-CoV-2 are at a significantly higher risk of developing venous thromboembolism after surgery (COVID et al. Citation2022). Additionally, patients with malignant diseases have a higher likelihood of experiencing thrombotic events compared to those with benign conditions (Sturlese et al. Citation2017). As a result, more attention is being paid to preventing DVT formation after tumour cell reduction in patients with advanced cancer (Loffredo et al. Citation2022). Currently, there are limited studies analysing the related influencing factors of DVT formation after tumour cell reduction in patients with advanced cervical and ovarian cancer.
In this study, we conducted a single-centre prospective case-control study to develop novel logistic regression models of postoperative DVT in patients who underwent radical resection of cervical and ovarian cancer. Our models were based on laboratory indicators such as coagulation, thromboelastography, stress response, and immune function, and aimed to easily estimate the risk of DVT. We also validated these models in an external validation cohort. This study was conducted in accordance with the TRIPOD guidelines (Supplementary Table 1) (Collins et al. Citation2015).
Table 1. Comparison of patients’ general clinical indicators and surgery-related indicators. (Data were represented as the Mean ± standard deviation (SD) or median [interquartile range, (IQR)] or percentage).
Materials and methods
Institutional review board
This study was under the approval of Medical Ethics Committee, JiangSu XiangShui Hospital of Chinese Medicine (NO.: 2017-07-13. V03), and written informed consent was obtained from all participants.
General information of patients included in this study
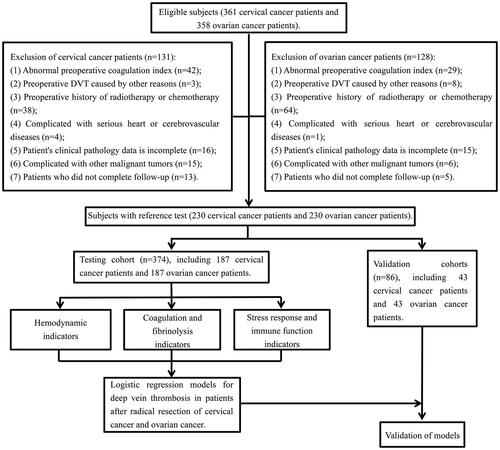
Between June 2017 and February 2019, we included a total of 361 cervical cancer patients and 358 ovarian cancer patients who were diagnosed at the JiangSu XiangShui Hospital of Chinese Medicine. After screening patients according to our inclusion and exclusion criteria, we conducted regular telephone follow-ups (). We excluded patients who were lost to follow-up and ultimately enrolled 230 cervical cancer patients and 230 ovarian cancer patients. General information about the patients is presented in .
Figure 1. The technical route of this study.

Inclusion and exclusion criteria
The inclusion criteria for patients were as follows: (1) Confirmation of advanced cervical cancer or ovarian cancer (stage III-IV) by clinicopathology; (2) Initial tumour cell reduction surgery; (3) Availability of complete relevant information; (4). Informed consent form signed by the patient and their family for the operation. Exclusion criteria were as follows: (1) Abnormal preoperative coagulation index; (2) Preoperative DVT caused by other reasons; (3) Preoperative history of radiotherapy or chemotherapy; (4) Presence of serious heart or cerebrovascular diseases; (5) Complicated with other malignant tumours.
Observation and detection indicators
We collected data on patients’ age, height, weight, preoperative complications, and pathological results. We also collected relevant indicators of patients’ surgery, including anaesthesia type, anaesthesia duration, operation duration, intraoperative blood loss, and length of postoperative hospital stay. The examiners conducted tests on the following samples under single-blind conditions, and analysed the resulting data.
Thromboelastography was performed as described before (Othman and Kaur Citation2017).
The primary evaluation indicators for coagulation and fibrinolysis were the prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), and D-dimer levels (D-D) for both groups, recorded before the operation, 1 day after the operation, and 3 days after the operation. Additionally, we calculated changes in the international normalised ratio (INR) of prothrombin using the INR method.
We drew a total of 4 mL of fasting venous blood from patients before the operation and in the morning on the 1st and 3rd days after the operation and placed them in tubes labelled A and B. We centrifuged tube A at 720 × g for 10 min, and stored the supernatant in a refrigerator at −20 °C for later testing. The serum levels of superoxide dismutase (SOD), interleukin 6 (IL-6), and C-reactive protein (CRP) were detected using ELISA kits purchased from Shanghai Enzyme Link Biotechnology Co., Ltd. (Li et al. Citation2020; Sun et al. Citation2021). We used a FACSCalibur flow cytometer from BD Company, USA, to detect CD4+ and CD8+ in tube B and calculate the CD4+/CD8+ ratio.
Testing cohort
Logistic regression prediction models were developed for the testing cohort to predict DVT. The cohort included 187 cervical cancer patients and 187 ovarian cancer patients. The patients’ general information is presented in .
Establishment formula of the logistic regression model
The DVT prediction model was developed using the following formula: Logit (P) =A0+A1B1+A2B2+…+AnBn=ln[p/(1-p)]. In this formula, ‘p’ represents the estimated probability of DVT, ‘A’ represents the coefficient for each indicator, and ‘B’ represents the level of each indicator.
Validation cohort
The logistic regression prediction models were validated in the validation cohort. The validation cohort consisted of 43 cervical cancer patients and 43 ovarian cancer patients. The patients’ general information is presented in .
Statistical analysis
The results are presented as mean ± standard deviation (SD), median [interquartile range, (IQR)], or percentage, as appropriate. Student’s t-test was used to analyse differences between normally distributed numeric variables, while non-normally distributed variables were analysed by Mann-Whitney U-test. One-way ANOVA was used to compare multiple groups if the variance was homogeneous. Non-normally distributed variables were analysed using Kruskal-Wallis variance analysis. Multiple comparisons between groups were performed using the S-N-K method. The receiver operator characteristic (ROC) curve was used to compare the area under the ROC curve (AUC) and the 95% confidence interval (CI) of each index for identifying DVT. Binary logistic regression analysis was used to identify risk factors for DVT after the operation. Variables identified as significant in the univariate logistic regression analysis were included in the multivariate regression analysis. All statistical analyses were performed using SPSS version 19.0 (IBM Corporation). A P-value of less than 0.05 was considered statistically significant.
Results
Technical route
The technical methodology employed in our study is illustrated in . Out of 361 cervical cancer patients and 358 ovarian cancer patients, 259 patients were excluded for not meeting the inclusion criteria. The remaining 230 cervical cancer patients and 230 ovarian cancer patients were randomly allocated to either the testing cohort or the verification cohort. The relevant patient demographics are presented in .
Comparison of coagulation, thromboelastography, stress response, and immune function indicators between the cervical cancer group and ovarian cancer group in the testing cohort
The comparison of the related indicators of coagulation, thromboelastography, stress response, and immune function at different times between the two groups was shown in . There was no significant difference in PT and INR values between the two groups at the same time point before and after the operation (all p > 0.05, ). However, compared with the same group before the operation, the other indicator levels significantly changed at 1 and 3 days after the operation (all p < 0.05, ). Additionally, we conducted a pairwise comparison between groups. Interestingly, we found that in the cervical cancer group, the changes in the patient’s indicators were the most significant the 1 day after surgery, while the ovarian cancer group had the most significant changes in the indicators the 3 days after the surgery (all p < 0.05, ).
Table 2. Comparison of changes of thromboelastography, coagulation, stress response, and immune function indicators at different time points before and after operation in the testing cohort (n = 374). (Data were represented as the Mean ± standard deviation (SD)).
Comparison of the incidence of DVT between the cervical cancer group and ovarian cancer group in the testing cohort
DVT occurred in 36 patients in the cervical cancer group and 22 patients in the ovarian cancer group. In the testing cohort, the incidence of DVT was higher in the cervical cancer group (19.3%) compared to the ovarian cancer group (11.8%, χ2=4.000, p = 0.046).
Logistic regression analyses and ROC analyses of coagulation, thromboelastography, stress response, and immune function indicators in the testing cohort
Given the significant difference in the incidence of DVT between the cervical cancer group and the ovarian cancer group, we performed univariate and multivariate logistic regression analyses for each group. The logistic regression analysis results are presented in Supplementary Table 2 and Supplementary Table 3. For cervical cancer patients, the levels of R-value, K value, α angle, MA, FIB, D-D, IL-6, and SOD 1 day after the operation were identified as independent factors for DVT (Supplementary Table 2). For ovarian cancer patients, the levels of R-value, K value, α angle, MA, FIB, CRP, and CD4+/CD8+ 3 days after the operation were identified as independent factors for DVT (Supplementary Table 3).
Table 3. The calculated performance values for different indicators in the testing cohort.
We further analysed the independent factors from the multivariate logistic regression analyses using the ROC method to predict the occurrence of DVT after radical resection of cervical and ovarian cancers. For cervical cancer, the AUC values of R-value, K value, α angle, MA, FIB, D-D, IL-6, and SOD were 0.835, 0.792, 0.917, 0.843, 0.797, 0.773, 0.715, and 0.747, respectively ( and ). For ovarian cancer, the AUC values of R-value, K value, α angle, MA, FIB, CRP, and CD4+/CD8+ were 0.807, 0.877, 0.867, 0.710, 0.787, 0.833, and 0.826, respectively ( and ).
Figure 2. ROC analysis of coagulation, thromboelastography, stress response, and immune function laboratory indicators to predict the occurrence of DVT after radical resection of cervical cancer and ovarian cancer in the testing cohort. (A) Radical resection of cervical cancer (n = 187). (B) Radical resection of ovarian cancer (n = 187). ROC: receiver operator characteristic; DVT: deep venous thrombosis.

Novel risk prediction models for DVT based on the testing cohort
The study employed the aforementioned indicators in logistic regression models to predict the occurrence of DVT after radical resection. For cervical cancer, the final model predicting DVT occurrence (1 day after operation) was Logit(P)=9.365–0.063(R-value) −0.112(K value) +0.386(α angle)+0.415(MA)+0.276(FIB)+0.423(D-D)+0.195(IL-6)+0.092(SOD). This model demonstrated high accuracy in identifying the occurrence of DVT after radical resection of cervical cancer, with an AUC of 0.934 (, Supplementary Table 2, and Supplementary Table 4). The estimated probability was 0.806, indicating that patients with a probability lower than 0.806 would be classified as at high risk of DVT. For ovarian cancer, the final model predicting DVT occurrence (3 days after the operation) was Logit(P)=−2.846–0.036(R-value) −0.157(K value) +0.426 (α angle) +0.172(MA) +0.221(FIB)+0.375(CRP)-0.126(CD4+/CD8+). This model also demonstrated high accuracy in identifying the occurrence of DVT after radical resection of ovarian cancer, with an AUC of 0.941 (, Supplementary Table 3, and Supplementary Table 4). The estimated probability was 0.697, indicating that patients with a probability lower than 0.697 would be classified as at high risk of DVT.
Validation of the logistic regression models
We evaluated the validity of our logistic regression models in a validation cohort. The data for the subjects are presented in and Supplementary Table 4. The validation cohort consisted of 43 cervical cancer patients and 43 ovarian cancer patients.
For cervical cancer, we classified patients into two groups based on their estimated probability scores: the group with estimated probability scores <0.806 (n = 8) and the group with estimated probability scores ≥0.806 (n = 35). The results are presented in . Patients in the group with estimated probability scores <0.806 had a significantly higher rate of DVT compared to those in the group with estimated probability scores ≥0.806 (χ2=43.165, P < 0.001). By applying the formula, we found that 7 out of 8 cervical cancer patients had estimated probability scores lower than 0.806, while 34 out of 35 cervical cancer patients had estimated probability scores higher than 0.806. The sensitivity and specificity of the model for predicting DVT occurrence after radical resection of cervical cancer were 87.5% and 97.1%, respectively (Supplementary Figure 1(A)).
Figure 3. Validation of the logistic regression models in the validation cohort. (A) Comparison of the incidence of DVT between the group of estimated probability ≥0.806 and the group of estimated probability <0.806 in the radical resection of cervical cancer group. (B) Comparison of the incidence of DVT between the group of estimated probability ≥0.697 and the group of estimated probability <0.697 in the radical resection of ovarian cancer group. DVT: deep venous thrombosis.

For ovarian cancer, we classified patients into two groups based on their estimated probability scores: the group with estimated probability scores <0.697 (n = 7) and the group with estimated probability scores ≥0.697 (n = 36). The results are presented in . Patients in the group with estimated probability scores <0.697 had a significantly higher rate of DVT compared to those in the group with estimated probability scores ≥0.697 (χ2=49.568, p < 0.001). By applying the formula, we found that 6 out of 7 ovarian cancer patients had estimated probability scores lower than 0.697, while 36 out of 36 ovarian cancer patients had estimated probability scores higher than 0.697. The sensitivity and specificity of the model for predicting DVT occurrence after radical resection of ovarian cancer were 85.7% and 100.0%, respectively (Supplementary Figure 1(B)).
Discussion
Tumour cell reduction is one of the main approaches in the clinical treatment of ovarian cancer and cervical cancer. However, due to the hypercoagulable state of most patients before surgery, the incidence of postoperative DVT increases under the influence of surgical stress (Deitcher Citation2003). Studies have demonstrated that among gynecological malignancies, ovarian cancer exhibits the highest probability of postoperative DVT, with rates ranging from 13.6% to 27.0%, and the lesions are predominantly located in the lower extremities (Basaran et al. Citation2021). DVT is a venous disorder caused by abnormal clotting of blood in deep veins. This mechanism may be attributed to surgical trauma leading to a significant release of prothrombin, which can influence blood agglutination (Zhao et al. Citation2022). Moreover, the decrease in antithrombin levels and other anticoagulant substances in patients’ bodies after surgery, and changes in blood cells and plasma proteins, further exacerbate the hypercoagulable state of blood and promote thrombosis (Sone et al. Citation2022). Embolus detachment poses the greatest risk of postoperative DVT, which can lead to fatal pulmonary embolism, impair patient’s quality of life, and even result in death. Even when the embolus does not detach, it can cause sequelae such as venous ulcer, pain, and edoema, which require treatment with an embolus screen that is expensive and significantly increases the economic burden of patients (Peng et al. Citation2021).
Previous studies have identified three main factors that contribute to the formation of DVT: venous blood flow stagnation, venous endothelial damage, and blood hypercoagulability (Line Citation2001; Ogoh et al. Citation2020; Yu et al. Citation2011). Hemodynamic factors, such as R-value, K value, α angle, and MA, are often associated with venous blood flow (Ogoh et al. Citation2020), while stress response and immune function are linked to venous endothelial damage (Line Citation2001; Yu et al. Citation2011). Blood hypercoagulability can be assessed through coagulation (PT and APTT) and fibrinolytic (FIB and D-D) functions (Ogoh et al. Citation2020). In addition, during the resection of cervical and ovarian cancer, the establishment of a pneumoperitoneum is crucial for creating a surgical field and facilitating the procedure. However, recent studies have shown that the establishment of CO2 pneumoperitoneum, along with the duration of the surgery and the patient’s position during laparoscopic surgery, can significantly affect hemodynamic and coagulation function, potentially leading to the formation of thrombosis (Donmez et al. Citation2016; Loffredo et al. Citation2022; Sharma et al. Citation2016; Tian and Li Citation2021). The establishment of CO2 pneumoperitoneum has been shown to significantly increase the inner diameter of the femoral vein and decrease the blood flow velocity in the lower extremity veins (Tian and Li Citation2021). Furthermore, the pneumoperitoneum can compress the inferior vena cava and bilateral iliac veins, resulting in increased venous blood flow resistance, reduced blood flow, and obstruction of venous blood return (Donmez et al. Citation2016). The elevation of the diaphragm and subsequent increase in intrathoracic pressure caused by pneumoperitoneum can also result in decreased diastolic ventricular filling and increased resistance of the inferior vena cava (Sharma et al. Citation2016). These factors can cause direct or indirect obstruction of venous blood in the lower limbs, impeding blood return. However, the detailed predictive value of coagulation, thromboelastography, stress response, and immune function indicators for the occurrence of DVT after radical resection of cervical cancer and ovarian cancer has not been extensively studied.
In this study, the most significant indexes were included in the establishment of the logistic regression model based on the comparison of the changes of laboratory indexes before surgery, 1 day, and 3 days after surgery. We found that the prediction accuracy of the final two regression models for postoperative DVT in patients with cervical cancer and ovarian cancer was 87.9% and 87.4%, respectively, and the specificity of the two models was 100%. In addition, we validated these models in a validation cohort. The results showed that both models still explored good predictive performance (for cervical cancer, the false positive rate was 12.5%, the false negative rate was 2.9%; for ovarian cancer, false positive rate: 14.3%, false negative rate: 0%), indicating that our model can effectively predict DVT in patients with cervical and ovarian cancer after resection. This study utilises a novel combination of coagulation, thromboelastography, stress response, and immune function indicators to predict the risk of developing DVT after radical resection of cervical and ovarian cancer. This approach has the potential to uncover the underlying mechanisms of DVT development in these patients. DVT is a severe and potentially life-threatening complication in cancer patients who undergo surgery, and identifying patients at high risk for DVT can help clinicians take preventive measures to reduce the risk of this complication. Notably, we have included a relatively large sample size of 460 patients, which may enhance the statistical power and generalisability of the results. Moreover, the risk prediction system we have constructed relies on a series of non-invasive and convenient detection methods that are easier for patients to accommodate. Therefore, our risk prediction models provide additional theoretical support for intervening in patients with a higher risk of developing DVT after cervical and ovarian cancer surgery.
Our study has several limitations. Firstly, it was conducted in a single centre in China, which may restrict the generalisability of the results to other populations or healthcare settings. Secondly, the predictive models developed in this study were not validated in an external, independent cohort, which may reduce the reliability and generalisability of the results. Thirdly, certain data on potential risk factors for DVT, such as smoking status and family history of thrombosis, were not collected, which may hinder a comprehensive assessment of the predictors of DVT. Fourthly, our study failed to detect other stress biomarkers, such as MDA, catalase, and nitric oxide, which is another limitation. Therefore, high-quality randomised controlled trials are still needed in the future to provide a theoretical basis for clinical interventions for postoperative DVT in cervical and ovarian cancer.
In summary, current risk prediction models that incorporate coagulation, thromboelastography, stress response, and immune function laboratory indicators may be more effective in enhancing the predictive accuracy of postoperative DVT in patients who have undergone radical resection for cervical and ovarian cancer.
Ethical approval
This study was under approval of Medical Ethics Committee, JiangSu XiangShui Hospital of Chinese Medicine (NO.: 2017-07-13.V03).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Download Zip (474.6 KB)Acknowledgements
As authors, we would like to express our gratitude to the individuals who willingly participated in this research. We would also like to extend our thanks to the Laboratory Medicine Department of JiangSu XiangShui Hospital of Chinese Medicine for their valuable support and guidance on the detection of all indicators in this study.
Disclosure statement
The authors report there are no competing interests to declare.
Data availability statement
Data available within the article.
Additional information
Funding
References
- Basaran, D., et al., 2021. Risk of venous thromboembolism in ovarian cancer patients receiving neoadjuvant chemotherapy. Gynecologic Oncology, 163 (1), 36–40.
- Bhandari, M., et al., 2022. Bibliometric analysis on exploitation of biogenic gold and silver nanoparticles in breast, ovarian and cervical cancer therapy. Frontiers in Pharmacology, 13, 1035769.
- Cires-Drouet, R.S., et al., 2022. Prevalence and clinical outcomes of hospitalized patients with upper extremity deep vein thrombosis. Journal of Vascular Surgery. Venous and Lymphatic Disorders, 10 (1), 102–110.
- Collins, G.S., et al., 2015. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ (Clinical Research ed.), 350, g7594.
- Collaborative; GlobalSurg Collaborative, C., 2022. SARS-CoV-2 infection and venous thromboembolism after surgery: an international prospective cohort study. Anaesthesia, 77 (1), 28–39.
- D’Oria, O., et al., 2022. The role of preoperative frailty assessment in patients affected by gynecological cancer: a narrative review. Italian Journal of Gynaecology and Obstetrics, 34 (02), 76–83.
- Deitcher, S.R., 2003. Cancer-related deep venous thrombosis: clinical importance, treatment challenges, and management strategies. Semin Thromb Hemost, 29, 247–258.
- Donmez, T., et al., 2016. Is there any effect of pneumoperitoneum pressure on coagulation and fibrinolysis during laparoscopic cholecystectomy? PeerJ., 4, e2375.
- Giannini, A., et al., 2020. Predictors of postoperative overall and severe complications after surgical treatment for endometrial cancer: the role of the fragility index. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 148 (2), 174–180.
- James, L.M. and Georgopoulos, A.P., 2023. Immunogenetic profiles and associations of breast, cervical, ovarian, and uterine cancers. Cancer Informatics, 22, 11769351221148588.
- Li, S., et al., 2020. Effects of choline supplementation on liver biology, gut microbiota, and inflammation in Helicobacter pylori-infected mice. Life Sciences, 259, 118200.
- Line, B.R., 2001. Pathophysiology and diagnosis of deep venous thrombosis. Seminars in Nuclear Medicine, 31 (2), 90–101.
- Loffredo, L., et al., 2022. Asymptomatic and symptomatic deep venous thrombosis in hospitalized acutely ill medical patients: risk factors and therapeutic implications. Journal of Thrombosis and Haemostasis, 20, 72.
- Mahasa, K.J., et al., 2022. A combination therapy of oncolytic viruses and chimeric antigen receptor T cells: a mathematical model proof-of-concept. Mathematical Biosciences and Engineering, 19 (5), 4429–4457.
- Ogoh, S., et al., 2020. Arterial and venous cerebral blood flow responses to long-term head-down bed rest in male volunteers. Experimental Physiology, 105 (1), 44–52.
- Othman, M. and Kaur, H., 2017. Thromboelastography (TEG). Methods in Molecular Biology, 1646, 533–543.
- Peng, M., et al., 2021. Solid tumor complicated with venous thromboembolism: a 10-year retrospective cross-sectional study. Clinical and Applied Thrombosis/Hemostasis: Official Journal of the International Academy of Clinical and Applied Thrombosis/Hemostasis, 27, 1076029620975484.
- Saenger, J., et al., 2004. Chemoembolization of rat liver metastasis with irinotecan and quantification of tumor cell reduction. Journal of Cancer Research and Clinical Oncology, 130 (4), 203–210.
- Sharma, A., et al., 2016. Effect of various pneumoperitoneum pressures on femoral vein hemodynamics during laparoscopic cholecystectomy. Updates in Surgery, 68 (2), 163–169.
- Sone, K., et al., 2022. Transiently elevated D-dimer levels post-concentrated ascites reinfusion therapy cannot be used to predict deep vein thrombosis-pulmonary embolism. The Journal of Obstetrics and Gynaecology Research, 48 (3), 817–823.
- Sturlese, E., et al., 2017. Thromboembolism prophylaxis in laparoscopic surgery for gynecologic benign diseases. Results of a single center experience in 922 procedures. Ann Ital Chir, 88, 342–347.
- Sun, Y., et al., 2021. The low expression of long non-coding RNA Linc00638 contributes to rheumatoid arthritis progression by regulating inflammation and oxidative stress. Nan Fang Yi Ke Da Xue Xue Bao, 41 (7), 965–971.
- Tian, Q. and Li, M., 2021. Risk factors of deep vein thrombosis of lower extremity in patients undergone gynecological laparoscopic surgery: what should we care. BMC Womens Health, 21, 130.
- Wang, Z., et al., 2021. Trends and age-period-cohort effects on mortality of the three major gynecologic cancers in China from 1990 to 2019: Cervical, ovarian and uterine cancer. Gynecologic Oncology, 163 (2), 358–363.
- Yasui, M., et al., 2022. Risk factors for postoperative proximal deep vein thrombosis and pulmonary embolism after laparoscopic colorectal cancer surgery: analysis of a multicenter randomized controlled trial. Surgery Today, 52 (6), 881–888.
- Yu, F.T., et al., 2011. A local increase in red blood cell aggregation can trigger deep vein thrombosis: evidence based on quantitative cellular ultrasound imaging. Journal of Thrombosis and Haemostasis, 9 (3), 481–488.
- Yu, R., et al., 2020. Efficiency and safety evaluation of prophylaxes for venous thrombosis after gynecological surgery. Medicine, 99 (25), e20928.
- Zhao, H., et al., 2022. Prevalence and treatment of venous thromboembolism in patients with solid tumors. Experimental and Therapeutic Medicine, 24 (6), 743.