

Abstract
We evaluated quantitative cervicovaginal foetal-fibronectin as a predictor of cervical ripening and labour duration in late-term pregnant women with an unfavourable cervix. This was an analytical cross-sectional study wherein 152 women, with late-term pregnancy and unfavourable cervix, at 41weeks3days gestational age, had pre-induction quantitative cervicovaginal foetal-fibronectin determined using ELISA. Data were compared in nulliparas and multiparas at a significance level < 0.05. The mean age of late-term pregnant women was 30.4 ± 4.3 years. Median cervicovaginal foetal-fibronectin levels in nulliparous and multiparous women were 45.35 ng/ml and 46.93 ng/ml respectively(p = 0.289). The correlation between foetal-fibronectin levels and cervical ripening duration was poor in nulliparous(r = 0.014) and multiparous(r = 0.024) women. The Youden’s foetal-fibronectin cut-off level had a sensitivity of 53.5% and specificity of 71.6% in predicting cervical ripening duration of > 12 hours in late-term pregnancy with an area under the ROC curve of 0.634. Quantitative cervicovaginal foetal-fibronectin is a poor correlate and predictor of cervical ripening and induced labour duration in late-term pregnancy.
What is already known on this subject? Cervicovaginal foetal fibronectin is useful in the prediction of preterm delivery but its role in prolonged pregnancy is unclear.
What the results of this study add? Cervicovaginal foetal fibronectin is a poor correlate and predictor of cervical ripening and induced labour duration in late-term pregnancy
What the implications are of these findings for clinical practice and/or further research? Cervicovaginal fibronectin should not be used to predict ease and success of cervical ripening and induction of labour in women with late-term pregnancy.
IMPACT STATEMENT
Introduction
Prolonged pregnancy is defined as a pregnancy that has reached 42 completed weeks or more from the first day of the last menstrual period (ACOG Practice Bulletin No. 55 Citation2004, Galal et al. Citation2012). The terminologies ‘post-term’, ‘prolonged’ ‘late-term’ and ‘after the term’ pregnancy are often used synonymously but some authors have suggested that the term ‘‘postdates’’ is not well defined and should be avoided (ACOG Practice Bulletin No. 55 Citation2004, Galal et al. Citation2012). Late-term pregnancy refers to a pregnancy that extends from 41 weeks through to 41 weeks 6 days (Spong Citation2013).
The incidence of prolonged pregnancy ranges from 4–12% of pregnant women (Hussain Citation2011) and it is associated with anxiety, increasing placenta insufficiency resulting in foetal hypoxia, meconium aspiration, oligohydramnios, growth restriction and macrosomia and its attendant complications (Mandruzzato Citation2010, Hussain Citation2011). Post-term births are associated with higher rates of perinatal morbidity and mortality than pregnancies delivered at term, hence induction of labour before 42 weeks is the advocated means of preventing these complications (Galal Citation2012).
One of the main favourable basal characteristics of successful induction of labour is a favourable or ripe cervix (Mackenzie Citation2006, Norman Citation2012). Induction of labour despite an unripe or unfavourable cervix is associated with a higher rate of prolonged labour and eventual Caesarean section (Khan Citation2012). In this circumstance, cervical ripening is necessary and can be artificially initiated, with cervical ripening agents, to improve the favourability of the cervix for induction of labour and thus the chance of vaginal delivery (Khan Citation2012, Wormer et al. Citation2022).
The modified Bishop scoring system, determined on digital pelvic examination, uses the cervical length, station, dilatation, position and consistency and is widely used to determine whether or not a cervix is ‘favourable’ and to assess whether or not cervical ripening is needed (Bishop Citation1964, Wormer et al. Citation2022). The Bishop score is easy to use, cost-effective and predicts vaginal delivery with a sensitivity around 75% (Bishop Citation1964, Wormer et al. Citation2022). However, it is not an objective method, in that; there could be inter-observer differences in cervical assessment (Akyol et al. Citation2007). The sensitivity of the bishop score for vaginal delivery varies widely among studies, also varying among cut-offs and populations. It also lacks good specificity and negative predictive value (Kolkman et al. Citation2013, Hu et al. Citation2022). Furthermore, Meier et al. systematically reviewed the literature to assess published models derived and validated to predict the success of vaginal birth following induction of labour but concluded that ‘no published model can be recommended for use at the bedside to determine the success of vaginal birth after labour induction’ (2019). Hence, a more objective tool could improve the care of women with unfavourable cervix prior to induction of labour.
Cervicovaginal foetal fibronectin is one of the biochemical markers of cervical changes that may subsequently result in labour and delivery (Lockwood et al. Citation1994, Sciscione et al. Citation2005, Adeniji et al. Citation2006, Heng et al. Citation2015). Several studies among Caucasians have assessed the role of cervicovaginal foetal fibronectin in predicting which patient will have shorter and easier induction of labour and lower Caesarean section rates with conflicting results (Lockwood et al. Citation1991, Garite et al. Citation1996, Crane Citation2006). Few studies have been done on Blacks and one study in South-west Nigeria reported that foetal fibronectin was useful in predicting cervical ripening duration (Adeniji Citation2006).
Due to the conflicting results of these studies and the paucity of data on this subject of research in West Africa, this study was designed to evaluate for an association between quantitative foetal fibronectin and cervical ripening and labour duration in women with late-term pregnancy and its possible predictive role. The use of an objective and reliable tool to predict cervical ripening and labour duration, in late-term pregnancy, would remarkably improve decision-making. This implies that the cohort of women, predicted to have prolonged cervical ripening duration, may benefit from possible outpatient cervical priming measures prior to admission with attendant potential clinical and resource benefits by deferring cervical ripening when safely possible.
Materials and methods
This was a prospective analytical cross-sectional study in which 152 consenting pregnant women with late-term pregnancy and unfavourable cervix, scheduled for induction of labour at a gestational age of 41 weeks and 3 days, were consecutively recruited over a 5-month duration (October 2013 to February 2014) at the obstetrics department of the Lagos State University Teaching Hospital, Lagos, Nigeria.
The study inclusion criteria consisted of consenting women with late-term pregnancy scheduled for induction of labour at a gestational age of 41 weeks and 3 days calculated from the last menstrual period (LMP) or early scan date for women unsure of their LMP; women with a singleton pregnancy, cephalic presentation, intact foetal membranes, modified Bishop score less than or equal to 6 and a reactive non-stress test.
Pregnant women with any of the following conditions were excluded from the study: gestational age less than 41 weeks (WHO Citation2011) or greater than 42 weeks, preceding coitus or douching within 24 hours of admission for induction of labour, multiple pregnancies, malpresentation, malposition, ruptured foetal membranes, antepartum haemorrhage, modified Bishop score greater than 6, features suggestive of foetal compromise, previous uterine scar and medical conditions like hypertension, diabetes, sickle cell disease, chronic renal disease etc and other contraindications to vaginal delivery.
A structured proforma was completed for each consenting pregnant woman eligible for the study. It was used to obtain detailed information from the study participants’ medical records and subsequently, information pertaining to labour induction and delivery. Some of this information included the maternal age, parity, estimated gestational age, assay for the quantity of foetal fibronectin in cervicovaginal secretions and the pre-cervical ripening modified Bishop score.
Foetal fibronectin sample collection
The consenting study participants were placed in a dorsal position, ensuring privacy, the presence of a female chaperone and adequate illumination. An appropriate size sterile Cusco speculum was inserted into the vagina following vulvar cleaning with normal saline. The Rapid fFN Test Specimen Collection Kit (Hologic, Inc., Sunnyvale, CA, USA) was used to collect specimens for foetal fibronectin assay. A Dacron polyester-tipped swab, a constituent of this collection kit was placed into the posterior vaginal fornix for 10 seconds to ensure saturation of the applicator with the cervicovaginal secretion. The swab was thereafter placed in the tube of the buffer provided with the specimen collection device for each patient after its removal from the vagina. The tube was labelled with the serial number allocated to each patient as in their proforma. The cervicovaginal samples were thereafter transported to the laboratory in ice packs. They were received by the laboratory scientist who stored the samples at a temperature of −70 °C or frozen and assayed them within three (3) months to avoid degradation of the analyte. Quantitative laboratory analysis of foetal fibronectin was done using the quantitative Rapid fFN 10Q analyser (Hologic) according to the manufacturer’s instructions.
Procedure of cervical ripening
A digital vaginal examination for the cervical assessment using the modified Bishop score was done immediately after obtaining the swab sample for foetal fibronectin. Only patients with a score of 6 or less, as stated in the inclusion criteria, were eligible to continue in the study. The patients were placed in a lithotomy position and the vagina was cleaned with an aseptic solution (chlorhexidine). A sterile Cusco speculum was inserted in the vagina to visualise the cervix. A size 22 Foley’s catheter was gripped with the sponge forceps and advanced up the endocervical canal through to the internal cervical os under aseptic conditions. The balloon of the catheter was inflated with 30 ml of sterile water. Thereafter, gentle traction was applied to the catheter and strapped down to the inner aspect of the woman’s thigh with adhesive tape. After the 24-hour period, the catheter is expected to have fallen out spontaneously or be removed with gentle traction. Hence, the cervix was reassessed with the Modified Bishop Scoring system (Wormer et al. Citation2022). Induction of labour was commenced when the modified Bishop score was > 6. On the other hand, women who remained with an unfavourable cervix after 24 hours had a new catheter replaced for another 24-hour period. Women who had unfavourable cervix despite 48-hours attempts at cervical ripening exited the study to allow for alternative means of cervical ripening according to the study hospital labour ward protocol.
Procedure of induction of labour
The method of induction of labour was by synchronous amniotomy with oxytocin infusion when bishop score was greater than 6. The labour ward staff (Midwife, Registrar, Senior Registrar and Consultant) on duty managed all parturients using the study hospital labour ward protocol. Oxytocin administration was by intravenous infusion, commencing at 5miliunit/minute (mU/min) in nulliparous women and 2.5 mU/min in multiparous women and escalating at 5mU/min every 30 minutes until adequate uterine contractions of 3 in 10 minutes each lasting 60 seconds were achieved or to a maximum of 30 mU/min.
During the labour process, adequate feto-maternal monitoring was carried out by monitoring the maternal pulse rate, blood pressure and urinalysis. Intermittent foetal heart rate auscultation using the sonicaid was done as well. Digital vaginal examination for cervical assessment was done four hours till the mother expressed the urge to bear down. The charting of the labour progress was done on a modified WHO partograph (Yisma et al. Citation2013). Failed induction was defined in this study as the inability to achieve vaginal delivery.
The study sample size was determined using a sample size calculator for a comparative study (Dhand and Khatkar Citation2014). Assuming a pooled standard deviation of 220 minutes (Sciscione et al. Citation2005) and a design effect of 2, the study required a total sample size of 136 to achieve a power of 80% and a level of significance of 5% (two-sided), for detecting a true difference (–150) in means of duration of cervical ripening between the foetal fibronectin positive (229 ± 220 minutes) and foetal fibronectin negative (379 ± 193 minutes) group in a similar study (Sciscione et al. Citation2005). A 10% attrition rate was factored in to obtain a minimum sample size of (136 + 14) 150.
Data analysis
The data obtained were entered and analysed using the statistical package for social sciences (SPSS), version 19. The respondents were categorised into nulliparous and multiparous. Percentages, mean and median of quantitative variables were determined. Chi-Square test was used to determine the association of categorical variables. Mann–Whitney U test was used to compare the median of two numerical variables. The correlation was evaluated using Pearson’s correlation. A predictive cut-off of foetal fibronectin was determined using Youden’s test. Sensitivity, specificity and negative predictive and positive predictive values were determined using 2 by 2 contingency tables and the receiver’s operating characteristic curve. For all statistical tests, a confidence level of 95% was used with p < 0.05 significance.
Ethical consideration
Informed written consent was obtained from all the study participants prior to enrolment. Ethical approval was obtained from Lagos State University Teaching Hospital (LASUTH) Ethical Review Committee before the commencement of the study.
Results
A total of 152 late-term pregnant women with unfavourable cervix had cervical ripening with transcervical catheter and subsequent induction of labour with oxytocin infusion. The numbers of women ineligible to continue in the study due to the presence of a favourable cervix at recruitment and women who needed to use alternative cervical ripening methods due to failure to achieve cervical ripening after 48 hours of trans-cervical Foley’s catheterisation were not noted.
The mean age of the late-term, pregnant women in the study was 30.4 ± 4.3 years. There was no difference in the age of nulliparous women compared to multiparous women (p = 0.117). More than three-fourths (78.2%) of nulliparous women and 61.9% of multiparous women in the study had cervical ripening duration of greater than 12 hours (p = 0.042) (). The total duration of labour was less than or equal to 24 hours in 78 (70.9%) nulliparas and 31 (73.8%) multiparas (p = 0.723). The Caesarean section rate was 34.5% among nulliparous women and 4.8% among multiparous women (p = 0.000) (). Of those who had an emergency caesarean section, the indications were for foetal distress, cervical stasis and cephalopelvic disproportion.
Table 1. Clinical Characteristics of Study Participants.
The median cervicovaginal foetal fibronectin value was 45.35 ng/ml and 46.93 ng/ml in nulliparous and multiparous women respectively (p = 0.289) (). The median duration of cervical ripening, duration of labour after cervical ripening and total duration of labour induction were 15.3 hours, 7.10 hours and 22.05 hours in nulliparous; and 14.3 hours, 6.45 hours and 20.02 hours in multiparous women respectively ().
Table 2. Comparison of median values of clinical characteristics based on parity.
Among nulliparous study participants, 55.5% had cervicovaginal foetal fibronectin levels less than Youden’s cut-off (9.975 ng/ml) while 44.5% of them were above the cut-off (p = 0.002), while 59.5% and 40.5% of multiparous women had their foetal fibronectin levels less than and greater than the Youden’s cut-off respectively (p = 0.075) ().
Table 3. Association between fibronectin level and duration of cervical ripening and labour.
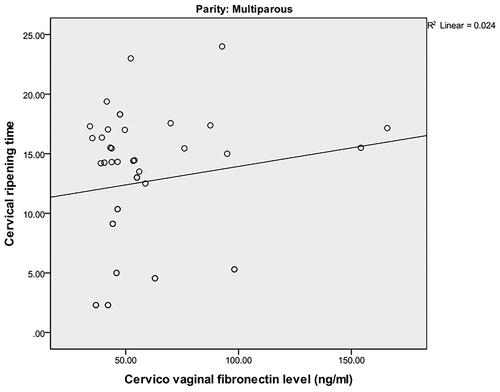
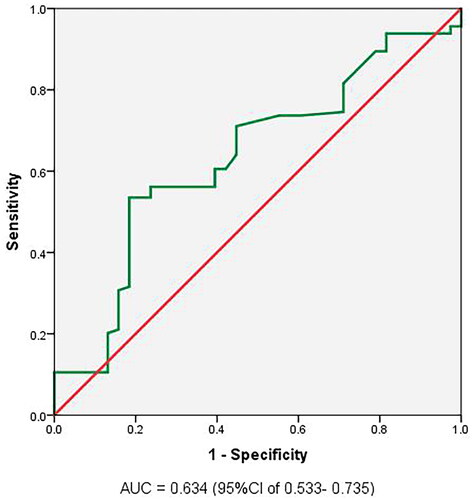
The correlation of quantitative cervicovaginal foetal fibronectin and cervical ripening duration in nulliparous was 0.014 () and in multiparous women, 0.024 (). Foetal fibronectin levels less than <9.975 (determined using Youden’s index), had a sensitivity of 53.3%, specificity of 71.6%, positive predictive values of 65.3% and negative predictive values of 60.6% in predicting cervical ripening duration of >12 hours in late-term pregnancy (Table S1). Foetal fibronectin levels less than <8.425 (determined using Youden’s index), had a sensitivity of 87.5%, specificity of 66.9%, positive predictive values of 72.7% and negative predictive values of 84.3% in predicting labour duration of >12 hours in induced late-term pregnancy (Table S2).
Figure 1. Scatter plot showing correlation between cervicovaginal foetal fibronectin level and duration of cervical ripening in nulliparous women.
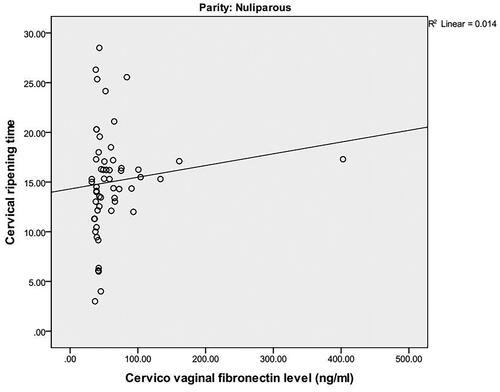
Figure 2. Scatter plot showing correlation between cervicovaginal foetal fibronectin level and duration of cervical ripening in multiprous women.
There was no significant difference in foetal fibronectin level of women that had a delivery through caesarean section and spontaneous vertical delivery (p-value = 0.331) However, among multiparous women, the foetal fibronectin level was significantly higher in women that had a delivery through caesarean section due to cephalo-pelvic disproportion than those that had spontaneous vaginal delivery and caesarean section irrespective of indication (p-value = 0.017) (Table S3). Post Hoc Test identified significant differences in foetal fibronectin between pregnant women with caesarean section due to cephalo-pelvic disproportion and those with caesarean section irrespective of its indication, and those with spontaneous vaginal delivery (Table S3). The ROC curve is slightly above the reference. The area under the curve was 0.634 which shows that foetal fibronectin had a weak predictive value in the prediction of the duration of cervical ripening in women with post-date pregnancy ().
Figure 3. Receiver Operating Characteristics curve for cervicovaginal fibronectin as a predictor of cervical ripening duration >12 hours.
Discussion
The ages of the study participants ranged between 21 and 43 years with a mean age of 30.4 ± 4.3 years. Women who had late-term pregnancies were majorly nulliparous (72.4%) as against multiparous women accounted for 27.6%. This finding is in sync with reports of other studies that suggest nulliparity as a predisposition to prolonged pregnancy (Tam et al. Citation1999, Ojutiku et al. Citation2002). It took longer than 12 hours (a duration determined arbitrarily) to achieve cervical ripening in 78.2% of nulliparous women and 61.9% of multiparous women in this study. This indicates that nulliparity also predisposes to prolonged cervical ripening as in other similar reports (Blanch et al. Citation1996, Teixeira et al. Citation2012). Cervical ripeness is known to exert a significant influence on induced labour outcomes (Wormer et al. Citation2022).
A recourse to caesarean delivery occurred in 34.5% of nulliparous and 4.8% of multiparous women. The combined caesarean section rate, following induction of labour, of 26.3% in this study is comparable to 24.1% reported by Osaheni et al. (Citation2014) in a similar study in Southern Nigeria A study in the United States reported a failed induction rate of 29.7% (Pennell et al. Citation2009) while Ekele and Isah (Citation2002) reported 9% in Northern Nigeria. In the study by Ekele et al. (2002) the Foley’s catheters for cervical ripening were left in-situ until they were expelled spontaneously and their study population had various indications for induction of labour at varying gestational ages.
Conflicting reports have been observed using cervicovaginal foetal fibronectin as an objective marker as a predictor of successful labour induction. Ahner et al. (Citation1995) reported a correlation between foetal fibronectin results with successful labour induction. They noted that fibronectin-positive patients had shorter intervals of delivery than fibronectin-negative patients in a qualitative assessment of foetal fibronectin in the cervicovaginal sample and in women at term but with varying gestational ages and indications for induction of labour. In as much as the Blanch et al. (Citation1996) study did agree with the Ahner et al. (Citation1995) findings, their opinion was different when multiparas were analysed separately.
Studies in Nigeria found that foetal fibronectin is expected to be present in the cervicovaginal sample at term (Blanch et al. Citation1996, Tam et al. Citation1999, Ojutiku et al. Citation2002, Adeniji et al. Citation2006). A quantitative assessment in this study observed a range of 32−402.40 ng/ml with a median value of 45.35 ng/ml and 46.93 ng/ml in the cervicovaginal samples for the nulliparous and multiparous women respectively.
We observed that foetal fibronectin levels were similar in women who achieved vaginal delivery compared to women who had a caesarean delivery. Furthermore, when indications for caesarean delivery were considered, women who had caesarean section due to cervical stasis had similar cervicovaginal foetal fibronectin levels when compared with values of women who had a vaginal delivery. This implies that pre-induction cervicovaginal fibronectin may not be of value in determining women with late-term pregnancy who would likely achieve vaginal delivery following cervical ripening and induction of labour.
In this study, foetal fibronectin values above the cut-off (9.975 ng/ml), determined by Youden’s index, were considered as high foetal fibronectin levels in the cervicovaginal samples; while low levels were values below the Youden’s cut-off for the duration of cervical ripening. The cut-off value 9.975 ng/ml was identified as the best predictor of cervical ripening duration. Late-term pregnant women with values less than 9.975 ng/ml were more likely to have cervical ripening duration greater than 12 hours. On the other hand, pregnant women with values higher than 9.975 ng/ml were more likely to have a cervical ripening duration of fewer than 12 hours. Foetal fibronectin levels less than 9.975 ng/ml, had a sensitivity of 53.5% and specificity of 71.6%, positive predictive values of 65.3% and negative predictive values of 60.6% in predicting cervical ripening duration of > 12 hours in women with late-term pregnancy, irrespective of parity. Adeniji et al. (Citation2006) also observed that positive foetal fibronectin predicted shorter cervical ripening time. However, this result was common for the patients in the misoprostol group regardless of their parity and gestational age at term (Adeniji et al. Citation2006). Misoprostol was not used for cervical ripening in this study.
This cut-off value of 9.975 ng/ml is much lower than the median foetal fibronectin levels of 45.35 ng/ml and 46.93 ng/ml observed in nulliparous and multiparous women in this study. These median foetal fibronectin levels and cut-off values of 50 ng/ml, used by numerous studies (Kiss et al. Citation2000, Uygur et al. Citation2016, Grab et al. Citation2022) in either predicting labour duration or successful induced labour outcome, were not near the best predictor value determined by Youden’s statistics among women in this study. This marked difference may be because we evaluated the predictor of cervical ripening duration while most other related studies predicted vaginal delivery or overall labour duration of less than 24 hours following cervical ripening and induction of labour.
Many other non-cervical related factors; such as the moulding capability of the presenting part, foetal attitude and the pelvic type and give, are involved in the mechanics and eventual outcome of labour. As cervicovaginal foetal fibronectin is a proven marker of cervical changes, an objective marker of possible cervical changes, cervical ripening duration - was our primary study outcome measure. We believe that pregnant women with late-term pregnancies predicted to have prolonged cervical ripening duration may benefit from possible outpatient cervical priming measures prior to admission with attendant potential clinical and resource benefits by deferring cervical ripening when safely possible.
With respect to the duration of labour, there was no significant relationship or correlation with cervicovaginal foetal fibronectin levels. The findings of this study are similar to the work carried out by Ojutiku et al. (Citation2002). They found no relationship between the foetal fibronectin and the variables - latent phase, length of labour and induction-delivery interval; and concluded that the modified Bishop score was reliable and better as a predictive tool (Ojutiku et al. Citation2002). Some other studies that used transcervical catheter as the ripening method though noticed a shorter induction-delivery interval with positive foetal fibronectin women, there was no appreciable differences between the negative and positive foetal fibronectin women regarding labour duration and outcome of labour (Sciscione et al. Citation2005).
A limitation of this study is that factors; such as the moulding capability of the presenting part, foetal attitude, pelvic compliance and pliability, which could influence labour duration and outcome were not assessed. Furthermore, excluding women who did not achieve cervical ripening in 48 hours, to allow for the possible use of another cervical ripening method; and management according to the study hospital protocol, may have introduced some bias.
In conclusion, pre-cervical ripening quantitative cervicovaginal foetal fibronectin levels insignificantly and very weakly correlates with cervical ripening and labour duration. It is also a poor predictor of short cervical ripening duration in women with late-term pregnancies.
Supplemental Material
Download Zip (37.4 KB)Declaration of interest
No potential conflict of interest was reported by the author(s).
Data availability statement
Study data not available.
Additional information
Funding
References
- Adeniji, A.O., et al., 2006. Cervicovaginal foetal fibronectin: a predictor of cervical response at pre-induction cervical ripening. West African Journal of Medicine, 24 (4), 334–337.
- Ahner, R., et al., 1995. Fetal fibronectin as a selection criterion for induction of term labor. American Journal of Obstetrics and Gynecology, 173 (5), 1513–1517.
- Akyol, A. et al., 2007. The role of Bishop score for successful labour induction. Perinatal Journal, 15 (1), 1.
- American College of Obstetricians and Gynecologists Practice Bulletin No. 55. 2004. Management of postterm pregnancy. Obstetrics & Gynecology, 104 (3), 639–646.
- Bishop, E.H., 1964. Pelvic scoring for elective induction. Obstetrics & Gynecology, 24, 266–268.
- Blanch, G., Oláh, K. S. and Walkinshaw, S., 1996. The presence of fetal fibronectin in cervicovaginal secretions of women at term–its role in the assessment of women before labour induction and in the investigation of the physiologic mechanism of labour. American Journal of Obstetrics and Gynecology, 174 (1 Pt 1), 262–266.
- Crane, J.M., 2006. Factors predicting labor induction success: a critical analysis. Clinical Obstetrics and Gynecology, 49 (3), 573–584.
- Dhand, N.K., Khatkar, M.S., 2014. Statulator: an online statistical calculator. sample size calculator for comparing two independent means. Avaialbe at: http://statulator.com/SampleSize/ss2M.html [Accessed 12 February 2023].
- Ekele, B.A. and Isah, A.Y., 2002. Cervical ripening: how long can the Foley catheter safely remain in the cervical canal? African Journal of Reproductive Health, 6 (3), 98–102.
- Galal, M., et al., 2012. Postterm pregnancy. Facts Views Vis Obgyn, 4 (3), 175–187.
- Garite, T.J., et al., 1996. Fetal fibronectin: a new tool for the prediction of successful induction of labor. American Journal of Obstetrics and Gynecology, 175 (6), 1516–1521.
- Grab, D., et al., 2022. Fetal fibronectin and cervical length as predictors of spontaneous onset of labour and delivery in term pregnancies. Healthcare, 10 (7), 1349.
- Heng, Y.J., et al., 2015. Human cervicovaginal fluid biomarkers to predict term and preterm labor. Frontiers in Physiology, 6, 151.
- Hu, T., et al., 2022. Establishment of a model for predicting the outcome of induced labor in full-term pregnancy based on machine learning algorithm. Scientific Reports, 12 (1), 19063.
- Hussain, A.A., et al., 2011. Elective Induction for systematic review with meta-analysis. BMC Public Health, 11 (S3), S5.
- Khan, N.B., et al., 2012. Factors associated with failed induction of labour in a secondary care hospital. J Pak Med Assoc, 62, 6–10.
- Kiss, H., et al., 2000. Fetal fibronectin as a predictor of term labor: a literature review. Acta Obstetricia et Gynecologica Scandinavica, 79 (1), 3–7.
- Kolkman, D.G., et al., 2013. The Bishop score as a predictor of labor induction success: a systematic review. American Journal of Perinatology, 30 (8), 625–630.
- Lockwood, C.J., et al., 1994. Low concentrations of vaginal fetal fibronectin as a predictor of deliveries occurring after 41 weeks. American Journal of Obstetrics and Gynecology, 171 (1), 1–4.
- Lockwood, C.J., et al., 1991. Fetal fibronectin in cervical and vaginal secretions defines a patient population at high risk for preterm delivery. New England Journal of Medicine, 325 (10), 669–674.
- Mackenzie, Z.I., 2006. Induction of labour at the start of the new millennium. Reproduction (Cambridge, England), 131 (6), 989–998.
- Mandruzzato, G., et al., 2010. Guidelines for the management of postterm pregnancy. J Perinat Med, 38 (2), 111–119.
- Norman, J. E., 2012. Induction and Augmentation of labour. In: D.K. Edmonds, ed. Dewhurst’s textbook of Obstetrics & Gynaecology. 8th ed. Hoboken, United States: Wiley-Blackwell.
- Ojutiku, D., Jones, G. and Bewley, S., 2002. Quantitative foetal fibronectin as a predictor of successful induction of labour in post-date pregnancies. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 101 (2), 143–146.
- Osaheni, L.L., et al., 2014. Obstetric outcome and significance of labour induction in a health resource poor setting. Obstetrics and Gynecology International, 2014, 1–5.
- Pennell, C., et al., 2009. Induction of labour in nulliparous women with an unfavourable cervix: a randomised controlled trial comparing double and single balloon catheters and PGE2 gel. BJOG : An International Journal of Obstetrics and Gynaecology, 116 (11), 1443–1452.
- Sciscione, A., et al., 2005. Fetal fibronectin as a predictor of vaginal birth in nulliparas undergoing preinduction cervical ripening. Obstetrics and Gynecology, 106 (5 Pt 1), 980–985.
- Spong, C. Y., 2013. Defining ‘term’ pregnancy: recommendations from the defining ‘term’ pregnancy workgroup. JAMA, 309 (23), 2445–2446.
- Tam, W.H., Tai, S.M.B. and Rogers, M.S., 1999. Prediction of cervical response to prostaglandin E2 using feta; fibronectin. Acta Obstetricia et Gynecologica Scandinavica, 78 (10), 861–865.
- Teixeira, C., et al., 2012. The Bishop score as a determinant of labour induction success: a systematic review and meta-analysis. Archives of Gynecology and Obstetrics, 286 (3), 739–753.
- Uygur, D., et al., 2016. Fetal fibronectin is more valuable than ultrasonographic examination of the cervix or Bishop score in predicting successful induction of labor. Taiwanese Journal of Obstetrics & Gynecology, 55 (1), 94–97.
- World Health Organisation 2011., World Health Organisation recommendations for induction of labour. Switzerland: World Health Organisation.
- Wormer, K.C., Bauer, A., Williford, A.E., 2022. Bishop Score [online]. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470368/ [Accessed 25 Jan 2022].
- Yisma, E., et al., 2013. Completion of the modified World Health Organization (WHO) partograph during labour in public health institutions of Addis Ababa, Ethiopia. Reproductive Health, 10, 23.