

Abstract
Inguinal lymph node involvement is the most robust predictor of mortality in vulval cancer and sentinel lymph node (SLN) biopsy is a safe diagnostic modality. We describe a technique based on anatomical landmarks. Our aims are (1) to describe the territorial mapping of SLNs, (2) to evaluate the associated complication rate vis-à-vis those reported in the literature, and (3) to assess its accuracy in detecting SLNs. Data from women who underwent groin SLN biopsies for vulval cancer at a single cancer centre were prospectively collected. All subjects met the GROINSS-V eligibility criteria. The location of the SLN relative to the saphenous vein was recorded. All women were followed up and early and late complications were recorded. The recurrence rate at the time of the census was calculated. A total of 71 groins in 44 women were included. The SLN was primarily located over Cloquet’s node (85.2%). The incidence of early wound cellulitis and dehiscence were 2.8% and 11.3% while lymphocysts were present in 11.3% of groins. The negative nodal recurrence rate was 1.7%. Results showed that this reproducible technique allows access to 96.7% of SLNs, including both deep and superficial SLNs whilst minimising the need for extensive dissection and complications associated with overharvesting of lymph nodes.
IMPACT STATEMENT
What is already known on this subject? Inguinal sentinel lymph node (SLN) biopsy in women with vulval cancer is often construed as a challenging skill to master and the success rate of SLN detection is dependent on the experience and skill of the surgeon. A review of the literature has revealed that whilst studies have largely concentrated on the efficacy of different intraoperative detection modalities or histopathological protocols, the literature describing a standardised surgical technique remains deficient.
What do the results of this study add? Our technique offers multiple advantages: our incision, albeit small, allows the operator to gain access to 96.7% of inguinal SLNs and facilitates access to both deep and superficial SLNs regardless of patients’ body mass index, minimises the need for extensive dissection and hence reduces the incidence of complications associated with overharvesting of lymph nodes such as lymphoedema or lymphocysts, particularly in obese women. Our local figures also support the safety of this operative technique (negative nodal recurrence rate 1.7%) and compare favourably with those from the GROINSS-V study.
What are the implications of these findings for clinical practice and/or further research? We describe a reproducible technique based on anatomical landmarks and an appreciation of the territorial mapping of inguinal SLN to optimise the chances of identifying the inguinal SLN in women with vulval cancer while circumventing the sequelae often attributed to this procedure.
Introduction
Vulval cancer accounts for 3–5% of all gynaecological cancers with over 90% of histological subtypes being comprised of squamous cell cancer (VSCC). Inguinal lymph node involvement is the strongest predictor of mortality (Morrison et al. Citation2020) and the gold standard treatment involves a radical excision of the tumour and inguinofemoral lymphadenectomy, except in FIGO stage 1a disease where the risk of inguinal nodal metastasis is less than 1% (Hacker and Van Der Velden, Citation1993). The risk of occult nodal involvement in women with stage 1b disease is approximately 30% and nodal staging is therefore recommended in this population. Traditionally, unilateral or bilateral complete lymphadenectomy was the standard of care to assess for nodal metastasis in women with vulval cancer. Unfortunately, total inguinofemoral lymphadenectomy is associated with significant morbidity in up to 70% of cases, usually manifest in the form of lower limb lymphoedema which may persist as a lifelong indisposition in some subjects (Giannini et al. Citation2022). Furthermore, nearly two-thirds of women with vulval cancer are aged over 65 and thusly present with multiple medical co-morbidities including frailty (Corrado and Garganese, Citation2022). Inguinal sentinel lymph node (SLN) biopsy was subsequently proposed as an alternative diagnostic approach to triage women into those who mandate a total lymphadenectomy and those who do not and is now the standardised treatment for early-stage VSCC following results from a multicentre study (GROINSS-V) which have demonstrated the safety and accuracy of this technique (Te Grootenhuis et al. Citation2016). The premise for this approach is that lymphatic drainage from the vulva follows a non-random fashion and cancer metastases usually spread to the SLN first. All studies to date have largely concentrated on the safety of SLN biopsies on oncological outcomes or establishing the role of various factors which could impact its detection rate including the use of different dyes and histopathological examination techniques (Meads et al. Citation2014, Wang et al. Citation2022). In contrast, the surgical technique for SLN biopsy or the role of SLN mapping has received less attention and there is a lack of standardised surgical methods for harvesting SLNs. Herein, we describe a technique whereby we rely on the anatomical landmarks to facilitate easy and quick access to SLNs so that surgical time and morbidity associated with ‘over-harvesting’ of lymph nodes can be minimised. Our technique is based on the assumption that the location of the long saphenous vein remains consistent even in obese subjects and thus serves as an important marker for orientation. For our operations, only Technetium-99 is used and all our patients undergo a SPECT-CT scan prior to their surgery. We performed a prospective study to define the territorial distribution of the inguinofemoral SLNs relative to the long saphenous vein. To the best of our knowledge, there are no other studies describing the mapping of groin SLN in vulval cancer following the publication of results from the GROINSS-V study.
The aims of this study are (1) to describe the territorial mapping of inguinal SLNs, (2) to evaluate whether this technique offers any benefit vis-à-vis complication rates reported in the literature and (3) to predict the accuracy of the nodal detection rate using this technique. This study conforms to the STROBE Statement: guidelines for reporting observational studies.
Methods
Patient and setting
Data from women who underwent unilateral or bilateral groin SLN biospies from 1 February 2020 to 15 October 2022 at a single regional cancer centre were prospectively collected. Our centre introduced inguinofemoral SLN biopsies for vulval cancer over 15 years ago and receives referrals from other Cancer Centres across the West Midlands, UK. All subjects met the GROINSS-V eligibility criteria (unifocal tumour, SCC of vulva, the width of tumour not exceeding 4 cm, depth of invasion over 1 mm and no clinically or radiologically suspected nodal involvement). Women with unresectable tumours measuring over 4 cm, multifocal lesions, enlarged or suspicious lymph nodes or in whom a nodal biopsy had previously confirmed the presence of nodal involvement, suspected disseminated disease on imaging (e.g., pulmonary or skeletal metastasis) and those who were pregnant at the time of the study were excluded. All women provided written consent for the procedure as per the Trust protocol. The location of superficial SLN was described relative to the long saphenous vein as ‘above and medial’, ‘above and lateral’ or ‘above saphenous vein’. Cloquet’s node was defined as the deep node medial to the saphenous vein and beneath the cribriform fascia. All women were followed 2-monthly for two years and then 4-monthly for a further three years.
Data were collected as part of routine treatment and the project was considered a ‘service evaluation’; therefore, ethics approval was not deemed necessary. Service evaluation does not require ethical approval in the UK (NHS HRA Citation2017, University College of London (UCL) Research Ethics Committee Citation2015).
Protocol and surgical technique
Four-quadrant peritumoral intradermal injections with technetium-99 radiocolloid were given preoperatively on the morning of the operation by the operating surgeon, followed by lymphoscintigraphy. Women were injected with 40 MBq of Tc99m nanocolloid in four 10MBq injections. The SLNs were identified at the site with the highest concentration of radioactive tracer on the SPECT-CT scan.
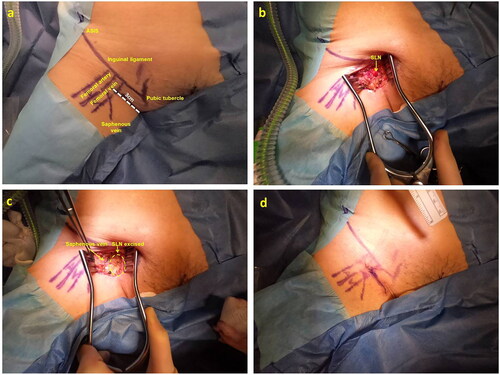
Surgical technique: We start by identifying the anterior superior iliac spine and pubic tubercle to map the course of the inguinal ligament. We then palpate the femoral artery to identify its location and a handheld Doppler may be used in obese women. Situated on its medial side in the femoral triangle is the femoral vein and the latter is joined on its medial side by the saphenous vein at the saphenofemoral junction. We make a 3-4cm incision inferior to and parallel to the inguinal ligament. The incision extends over the femoral vein and slightly above the saphenous vein (). Radiolocalisation of the SLN was achieved after identifying and excising the node with the highest signal count using a handheld gamma counter. The groin was re-examined and dissection continued until there was no residual radioactivity. All histological specimens were analysed using ultrastaging with immunohistochemistry. Ipsilateral unilateral inguinal SLN biopsies were conducted for lateral tumour and bilateral excisions for central tumours. The long saphenous vein was preserved in all cases.
Figure 1. Surgical technique for sentinel lymph node (SLN) biopsy; a – landmark mapping prior to skin incision; b - the SLN is identified and isolated; c - post-excision of SLN; d - 3 cm skin incision closure following SLN biopsy.
Statistical analysis
Quantitative data with a parametric distribution were presented using mean ± standard deviation while qualitative data was reported using numbers and percentages. Pearson’s chi-squared test was used for categorical variables. Results with a p value ≤0.05 were considered to be statistically significant. Data analysis was performed using STATA version 17.
Results
71 groins in 44 women were included in the analysis (). The mean age was 64 years. 155 lymph nodes were harvested (mean 2.2 nodes per groin). SLN were successfully identified and obtained in 67 groins (detection rate 94.3%). The SLN could not be detected either preoperatively on lymphoscintigraphy or intraoperatively using the gamma counter in four groins and these patients underwent a full lymphadenectomy. In two groins, the SLN was not identified preoperatively but emitted strong signals intraoperatively and were successfully removed. The location of the SLN was documented in 61 groins. Its position corresponded to Cloquet’s node in 52 groins (85.2%) and the rest were located above and medial to a long saphenous vein in 6 groins (9.8%), above and lateral to long saphenous vein in 2 groins (3.3%) and above the long saphenous vein in a single case (1.7%) (). There was no statistically significant correlation between the laterality of the tumour and the location of the SLN (p = 0.893). The incidence of early wound cellulitis and dehiscence were 2.8% and 11.3% respectively while lymphocysts were noted in 11.3% of groins within 30 days of the operation. We undertook 66 SLN biopsies in 41 women with SCC of the vulva. Of those, 59 were negative for cancer and a recurrence was diagnosed in one of these (1.7%). At the time of census (15 October 2022), four women were deceased of which two were from disease-specific causes.
Figure 2. Topographical distribution of inguinofemoral SLN.
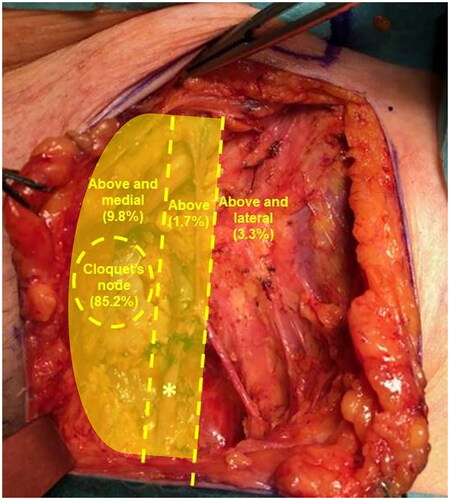
Table 1. Demographic and clinico-pathological outcomes.
Discussion
We describe a surgical technique using technetium-99 and not methylene blue to detect and excise inguinal SLNs. Methylene blue dye was not used for a number of reasons: the SLN detection rate with methylene blue is inferior (65.3%) (Deken et al. Citation2020) and any inadvertent sectioning of the lymphatic ducts during the operation will result in flooding of the surgical field with blue dye which may hamper our vision. Furthermore, our figures have demonstrated that our local negative lymph node recurrence rate using this operative technique is 1.7%. These figures are comparable to those from the GROINSS-V study (Te Grootenhuis et al. Citation2016) which had previously used a combination of methylene blue and Technetium-99. Our figures thusly confirmed that the addition of methylene blue dye did not increase the sensitivity in detecting SLNs.
Previously, Rob et al. (Citation2007) described the anatomical location of SLNs within the groin. This study preceded the GROINSS-V study and aimed to identify an optimal technique for identifying groin SLNs. The study described three groups of superficial nodes: medial (above and medial to the femoral and saphenous veins), intermediate (in the vicinity of and lateral to saphenous and femoral veins), lateral (an outer third of the groin) and one group of deep nodes located along and medial to the femoral vein. Their results showed that approximately two-thirds of SLNs were located medial to the femoral lymph nodes whilst the rest drained to the superficial intermediate nodes. Our results differed from Rob et al whereby 85.2% of SLNs were identified in the deep femoral nodes (Cloquet’s node) in our cohort compared to 16.1%. Our hypothesis that Cloquet’s node corresponds to the inguinal SLN in the majority of patients is supported by the anatomical lymphatic drainage from the vulva. The superficial inguinal lymph nodes located above the cribriform fascia drain into the deep nodes. The uppermost deep node, ‘Cloquet’s node, is considered the nexus between the inguinofemoral and iliac nodes. Drainage from lateral structures proceeds to the superficial inguinal lymph nodes whilst drainage from the clitoris either converges towards the superficial inguinal lymph nodes or terminates directly into the deep inguinal or iliac nodes (Anon Citation1961, Sharma and Suneja Citation2013). It therefore follows that Cloquet’s node is of considerable clinical significance as a candidate for the SLN as it receives lymphatics directly from the clitoris as well as the superficial inguinal nodes which drain the rest of the vulva. Therefore, it was not surprising that most of the SLN found were part of the Cloquet’s nodal group. In contrast, the course of lymphatic drainage in cervical and uterine cancers is less consistent. The FIRES trial (Rossi et al. Citation2017) demonstrated that while the majority of SLN were primarily located along the external iliac (38%), obturator (25%), inframesenteric para-aortic (14%) and common iliac vessels (8%), approximately 17% of SLNs were located outside the boundaries for routine pelvic lymphadenectomy (pre-sacral and internal iliac regions or parametrium). Ultimately, the location of the SLNs in women with vulval cancer is more predictable compared to other gynaecological cancers as 85% of SLNs are located over Cloquet’s area.
Our proposed surgical incision, albeit small, allows the operator to gain access to the superficial and deep inguinal nodes where the SLNs are most likely to be found; in our case, 96.7% of SLN were located within the territory accessed via the incision proposed (). Therefore, our proposed incision facilitates rapid and easy access to both superficial and deep inguinal lymph nodes regardless of the patients’ body mass index, and this reduces the need for extensive dissection while minimising the incidence of early and long-term complications associated with SLN biopsy. Our technique provides a fixed anatomical landmark to assist the surgeon in gaining access to SLN and therefore circumvents a number of challenges such as overharvesting lymph nodes and their associated sequelae such as lymphoedema or lymphocyst formation, particularly in obese women. In addition, the benefit of our technique is evidenced by our relatively low incidence of complications; our figures compared favourably with the rates reported in the GROINSS-V trial especially those of wound cellulitis (2.8% vs 4.5%) and dehiscence (11.3% vs 11.7%). Finally, in cases where a full lymphadenectomy may be required in the future, extending the incision parallel to the inguinal ligament is sufficient to facilitate access to the rest of the nodal basin which remains untampered with and hence less likely to be fibrotic at re-exploration.
The negative nodal recurrence rate was 1.7% in our cohort. Although we concede that the mean follow-up duration (16 months) was relatively short, these figures are comparable to results we had previously published using a similar technique whereby we demonstrated a negative nodal recurrence rate of 2% in women with VSCC who underwent an SLN biopsy in our centre (Underwood et al. Citation2013). All women in that cohort had been selected according to the GROINSS-V criteria and all specimens were processed according to their described protocol. A long-term audit of 131 women with VSCC who underwent inguinofemoral SLNB within our centre showed a recurrence rate of 2.1% in women who had previously been identified with a negative SLN at their index surgeries (n = 4) and this is below those reported by the GROINSS-V study (figure S1).
Tailoring adjuvant treatment according to the results of the SLN biopsy is essential to improve the oncological outcomes in women with vulval cancer and further decrease treatment-related morbidity. Inguinofemoral lymphadenectomy followed by adjuvant radiotherapy is currently advocated for all women diagnosed with >1 metastatic node or those with extracapsular nodal spread. Recent evidence from the GROINSS-V-I study (Oonk et al. Citation2021) has demonstrated that adjuvant inguinofemoral radiotherapy alone (without inguinofemoral lymphadenectomy) is a safe alternative in women with SLN micrometastasis (≤2mm) as the ipsilateral groin nodal recurrence rate at two years is low (1.6%). However, the omission of inguinofemoral lymphadenectomy in women with SLN macrometastases (>2mm) is associated with detrimental outcomes: 22% of women who underwent adjuvant radiotherapy alone recurred at two years compared to 6.9% with inguinofemoral lymphadenectomy with or without adjuvant radiotherapy.
The authors acknowledge that one of the limitations of this study is that it was conducted in a single cancer centre. Furthermore, the Surgeons relied on radio localisation of the SLN through recognition of the characteristic sound associated with the Geiger counters in all subjects. The fluorescent dye indocyanine green (ICG) has emerged as one of the main tracers for SLN mapping in early gynaecological cancers (Uccella et al. Citation2022, Raffone et al. Citation2022). Further randomised controlled trials are required to validate the safety and effectiveness of ICG for real-time intraoperative SLN mapping in vulval cancer.
Conclusion
The success rate of SLN detection is dependent on the experience and skills of the surgeon and inguinofemoral SLN biopsy is often construed as a challenging skill to master. We hereby describe a reproducible surgical technique based on anatomical landmark mapping and knowledge of the topographical distribution of the SLNs. We believe that our technique allows the operator to reduce the risk of perioperative complications by facilitating access to SLN, minimising excessive dissection, completing the procedure via a conservative incision and protect women from the morbidity associated with extensive dissection and overharvesting of lymph nodes. Finally, we demonstrated that this technique does not compromise on oncological outcomes and the negative nodal detection rate remains lower than those reported in the literature.
Ethics statement
This study was undertaken in line with our institution’s Clinical Information and Audit Department regulations. Ethical approval was not required. All patient data were anonymised. Written consent was obtained for photographs.
Author contribution
The authors confirm contribution to the paper as follows: study conception and planning: JY; data collection, analysis and interpretation of results: FLK, MS; draft manuscript preparation: FLK. All authors reviewed the results and approved the final version of the manuscript.
Supplemental Material
Download TIFF Image (29.5 MB)Acknowledgement
The authors would like to thank all women who have participated in this study.
Disclosure of interests
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Anon. 1961. Chapter 1: anatomy of the vulva. In: Acta Radiologica. Taylor and Francis. 16–23
- Corrado, G. and Garganese, G., 2022. Leading new frontiers in vulva cancer to build personalized therapy. Cancers, 14 (24), 6027.
- Deken, M.M., et al., 2020. Near-infrared fluorescence imaging compared to standard sentinel lymph node detection with blue dye in patients with vulvar cancer-a randomized controlled trial. Gynecologic Oncology, 159 (3), 672–680.
- Giannini, A., et al., 2022. The giant steps in surgical downsizing toward a personalized treatment of vulvar cancer. The Journal of Obstetrics and Gynaecology Research, 48 (3), 533–540.
- Hacker, N.F. and Van Der Velden, J., 1993. Conservative management of early vulvar cancer. Cancer, 71 (4 Suppl), 1673–1677.
- Meads, C., et al., 2014. Sentinel lymph node biopsy in vulval cancer: systematic review and meta-analysis. British Journal of Cancer, 110 (12), 2837–2846.
- Morrison, J., et al., 2020. Vulval cancer guidelines: Recommendations for practice [online]. British Gynaecological Cancer Society (BGCS). Available from: https://www.bgcs.org.uk/wp-content/uploads/2021/07/BGCS-vulval-guidelines-v22.pdf [Accessed 28 January 2023]
- National Health System (NHS) Health Research Authority (HRA). 2017. Governance Arrangements for Research Ethics Committees (GAfREC) [Web page]. UK Health Departments. Available from: http://www.hra.nhs.uk
- Oonk, M.H.M., et al., 2021. Radiotherapy versus inguinofemoral lymphadenectomy as treatment for vulvar cancer patients with micrometastases in the sentinel node: results of GROINSS-V II. Journal of Clinical Oncology, 39 (32), 3623–3632.
- Raffone, A., et al., 2022. Comparison between laparoscopic and robotic approach for sentinel lymph node biopsy in endometrial carcinoma women. Journal of Personalized Medicine, 13 (1), 29.
- Rob, L., et al., 2007. Further data on sentinel lymph node mapping in vulvar cancer by blue dye and radiocolloid Tc99. International Journal of Gynecological, 17 (1), 147–153.
- Rossi, E.C., et al., 2017. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): a multicentre, prospective, cohort study. The Lancet. Oncology, 18 (3), 384–392.
- Sharma, A. and Suneja, A., 2013. Vulva: anatomy, blood supply and lymphatic drainage. In: Rajaram S., Goel N., ed. State-of-the-Art Vaginal Surgery. Jaypee Brothers Medical Publishers. 1–8.
- Te Grootenhuis, N.C., et al., 2016. Sentinel nodes in vulvar cancer: long-term follow-up of the GROningen INternational Study on Sentinel nodes in Vulvar cancer (GROINSS-V) I. Gynecologic Oncology, 140 (1), 8–14.
- Uccella, S., et al., 2022. Cervical versus utero-ovarian ligament injection of the tracer for the pelvic sentinel lymph node mapping in gynecologic oncology: A prospective observational study. Gynecologic and Obstetric Investigation, 87 (3-4), 242–247.
- Underwood, M., et al., 2013. The use of sentinel node sampling in vulval cancer. Journal of Obstetrics and Gynaecology, 33 (8), 892–897.
- University College of London (UCL) Research Ethics Committee 2015. Exemptions [Web page]. University College of London. Available from: https://ethics.grad.ucl.ac.uk/exemptions.php
- Wang, T., et al., 2022. Sentinel Lymph Node Mapping: Current Applications and Future Perspectives in Gynecology Malignant Tumors. Frontiers in Medicine, 9, 922585.