

Abstract
Reliably predicting spontaneous preterm birth remains challenging, therefore it persists as a major contributor to perinatal morbidity and mortality. The use of biomarkers to predict premature cervical shortening, a recognised risk factor for spontaneous preterm birth, is yet to be fully explored in current literature. This study evaluates seven cervicovaginal biochemical biomarkers as possible predictors of premature cervical shortening. Asymptomatic, high-risk women (n = 131) presenting to a specialised preterm birth prevention clinic were analysed through a retrospective data analysis. Cervicovaginal biochemical biomarker concentrations were obtained, and the shortest cervical length measurement, up to 28 weeks’ gestation, was recorded. Associations between biomarker concentration and cervical length were then analysed. Of the seven biochemical biomarkers, Interleukin-1 Receptor Antagonist and Extracellular Matrix Protein-1 had statistically significant relationships with cervical shortening below 25 mm. Further investigation is required to validate these findings and any downstream clinical utility, with intentions to improve perinatal outcomes.
What is already known on this subject? Preterm birth is a major cause of perinatal morbidity and mortality. A woman’s risk of delivering preterm is currently stratified using historical risk factors, mid-gestation cervical length, and biochemical biomarkers such as foetal fibronectin.
What do the results of this study add? In a cohort of high-risk, asymptomatic pregnant women, two cervicovaginal biochemical biomarkers, Interleukin-1 Receptor Antagonist and Extracellular Matrix Protein-1, displayed associations with premature cervical shortening.
What are the implications of these findings for clinical practice and/or further research? Further investigation into the possible clinical utility of these biochemical biomarkers is warranted, with a view to improving preterm birth prediction and antenatal resource utilisation, thereby reducing the burden of preterm birth and its sequelae in a cost-effective manner.
IMPACT STATEMENT
Introduction
Preterm birth (PTB), i.e., delivery prior to 37 weeks’ gestation, is a leading cause of perinatal morbidity and mortality, with approximately 11% of livebirths worldwide occurring prematurely (Blencowe et al. Citation2012). Prematurity is associated with a multitude of acute and chronic health complications secondary to multi-organ immaturity and the consequent physical and psychological manifestations (Ward and Beachy Citation2003, Saade et al. Citation2016). Consequently, this population poses a significant clinical resource and financial burden on the healthcare system and broader economy (Hodek et al. Citation2011). The diverse aetiology that precipitates PTB adds to the complexity in predicting and preventing this suboptimal obstetric outcome (Singh et al. Citation2020).
Being a heterogeneous condition, PTB can be broadly categorised as iatrogenic or spontaneous (Goldenberg et al. Citation2008, Polettini et al. Citation2017). Iatrogenic PTB consists of medically indicated premature induction of labour for maternal or foetal disease (Goldenberg et al. Citation2008). Conversely, the aetiology behind spontaneous PTB includes intra-uterine infection, premature rupture of membranes, and premature cervical remodelling – i.e., the focus of this study (Moutquin Citation2003). Despite extensive research into this field, there is currently no effective intervention to prevent preterm delivery once active premature labour has begun, thus the focus on predicting those at risk of PTB (Petraglia and Visser Citation2009, Hughes et al. Citation2017). Current approaches used to predict spontaneous PTB, before labour has commenced, can be divided into three broad groups including risk-factors, cervical length and biomarkers (Georgiou et al. Citation2015).
Dedicated PTB clinics, largely receiving referrals based on risk factors for PTB, have been successful in reducing PTB rates and perinatal morbidity (Vernet et al. Citation2017, Jin et al. Citation2021). They provide a focussed distribution of resources and preventative interventions for those at highest risk of PTB (Newnham et al. Citation2014). Historical risk factors for PTB include a past history of PTB, previous cervical surgery and uterine malformations. Individuals can be misclassified as low risk for PTB as spontaneous PTB can occur in the absence of identifiable risk factors or prior gestational history (Son and Miller Citation2017). If women at increased risk of PTB could be identified more reliably, then more vigilant antenatal surveillance could be appropriately assigned, whilst avoiding superfluous interventions for lower-risk women (Conde-Agudelo et al. Citation2011).
Mid-gestation cervical length (CL) measured through trans-vaginal ultrasound (TVS) is another screening tool used to identify women at increased risk of PTB (Iams et al. Citation1996) given the significant association between short CL and PTB (Watson et al. Citation1999). Normally, the cervix gradually shortens and ripens from mid-trimester until term in preparation for labour (Kushnir et al. Citation1990). Premature cervical shortening to <25 mm, and especially <15 mm, is an indication for more vigilant antenatal surveillance, as approximately 35% and 48% of women respectively will go on to deliver prematurely (Jin et al. Citation2021). TVS has been favoured given the real-time insight into the cervical state (Iams et al. Citation1996, Heng et al. Citation2015). However, as with all ultrasound imaging, accurate TVS requires expensive equipment and experienced ultrasonographers (Parry and Elovitz Citation2014). Therefore, a more sensitive test to predict premature cervical shortening would assist in appropriate identification and triage of high-risk women.
There is active investigation into novel biochemical biomarkers that could potentially predict PTB (Conde-Agudelo et al. Citation2011, Polettini et al. Citation2017, Leow et al. Citation2020). Foetal fibronectin is the most widely used biomarker for predicting premature delivery in women with symptomatic threatened PTB (Lockwood et al. Citation1991). However, foetal fibronectin has a limited role in predicting PTB in asymptomatic women (Conde-Agudelo et al. Citation2011). Other cervicovaginal biochemical biomarkers are being explored to investigate their potential to predict spontaneous PTB in asymptomatic women (Leow et al. Citation2020). Given the current difficulty predicting PTB, and the strong association between premature cervical shortening and spontaneous PTB (Iams et al. Citation1996), it validates the exploration of biochemical biomarkers which could predict premature cervical shortening.
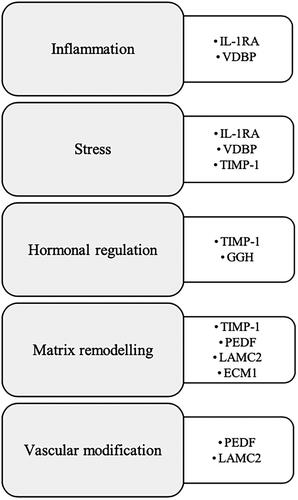
There are several contending biomarkers to consider as potential predictors of premature cervical shortening (Leow et al. Citation2020). The Prediction of PreTerm Labour (PPeTaL) study shortlisted seven preferred candidates using bioinformatic screening and cervicovaginal fluid (CVF) proteomics (Leow et al. Citation2020). These biomarkers include: interleukin-1 receptor antagonist (IL-1RA), 𝛾-glutamyl hydrolase (GGH), extracellular matrix protein-1 (ECM1), vitamin D binding protein (VDBP), metalloproteinase inhibitor-1 (TIMP-1), laminin subunit gamma-2 (LAMC2) and pigment epithelium-derived factor (PEDF). They are involved in various biological processes pertinent to cervical remodelling namely inflammation, oxidative stress, hormonal regulation, matrix remodelling, and vascular modification (Leow et al. Citation2020). The association between these biomarkers and CL will be explored in this study.
This study aims to analyse the predictive value of entry-level concentrations of seven biochemical biomarkers to identify women at increased risk of subsequent premature cervical shortening. This was achieved through a retrospective data analysis of CL and CVF biochemical biomarkers from the PPeTaL database (Leow et al. Citation2020).
Methods
This study was a retrospective data analysis using a subset of the PPeTaL database, which has been described in a previous publication (Leow et al. Citation2020). The PPeTaL study received ethics approval from relevant local institutional committees (Leow et al. Citation2020). In addition to the criteria outlined in the PPeTaL study (Leow et al. Citation2020), inclusion criteria for this study specified asymptomatic pregnant women, ≥18 years of age, attending antenatal follow-up at a specialist PTB prevention clinic, receiving serial CL measurements and biochemical biomarker analysis on their entry-level CVF sample. Referral to the PTB prevention clinic was based on risk factors such as a past history of PTB and/or premature cervical shortening, previous cervical surgery (e.g., cone biopsy), and congenital uterine malformations. Exclusion criteria were if entry-level CVF sample volume was too low for biochemical analyses to be completed.
CVF collected at the time of recruitment was analysed for the seven cervicovaginal biochemical biomarkers. This was compared against the shortest TVS CL recorded up to 28 weeks’ gestation, in the absence of any signs suggestive of labour. CVF was collected using a sterile speculum and double-tipped swabs (Medical Wire & Equipment Co. Ltd.), which were immersed in CVF for 30 s, then placed into 1 mL of extraction buffer. The samples were vortexed, then centrifuged, followed by collection of the supernatant and storage at −80 °C (Leow et al. Citation2020). The seven biomarkers analysed were IL-1RA, GGH, ECM1, VDBP, TIMP-1, LAMC2 and PEDF, in ng/mL (Leow et al. Citation2020). Their concentrations were quantified using either in-house (IL-1RA, GGH, ECM1 and VDBP) or commercially available (TIMP-1, LAMC2 and PEDF) enzyme-linked immunosorbent assays (ELISA) (Leow et al. Citation2020). TIMP-1 was analysed using the DuoSet ELISA kit (DY970, R&D Systems, Minneapolis, Minnesota, USA), LAMC2 was analysed using LAMC2 ELISA kit (SEC083Hu, Cloud-clone, Wuhan, China), and PEDF was analysed using human SERPINF1/PEDF DuoSet ELISA kit (DY1177-05, R&D Systems) (Leow et al. Citation2020).
Continuous demographic variables were represented as means and standard deviations. Categorical demographic variables were displayed as gross quantities and proportions. Analysis of Variance (ANOVA) (continuous variables) and Chi-squared tests (categorical variables) were conducted to investigate demographic discrepancies amongst the three outcome groups in the three-tiered model, reported as p-values with significance set at <0.05. The following demographics were analysed: maternal age, parity, maternal body mass index (BMI), history of cervical surgery, history of uterine malformation, fertility assisted pregnancy, smoking status, and number of previous miscarriages (<20 weeks’ gestation).
The primary outcome was the shortest CL recorded up to 28 weeks’ gestation. The variables of interest were the seven entry-level biochemical biomarkers. The biomarkers were all continuous variables and the shortest recorded CL, while continuous in nature, was converted into a categorical variable according to standardised cut-offs (Iams et al. Citation1996). Two groups of analyses were performed: (a) two-tiered model – Normal CL (>25 mm) or Short CL (≤25 mm); (b) three-tiered model – Normal CL (>25 mm), Short CL (16–25 mm) or Very Short CL (≤15 mm). In both cases Normal CL was used as the reference group.
Univariate relationships were explored by standard logistic regression with odds ratios (OR) (two-tiered model) and multinomial logistic regression with relative risk ratios (RRR) (three-tiered model), with p-values < 0.05 considered significant. An arbitrary p-value of 0.02 was used for selection in a potential multivariate model. All data were analysed in Stata version 15 (Statacorp, LLC Texas, USA).
Results
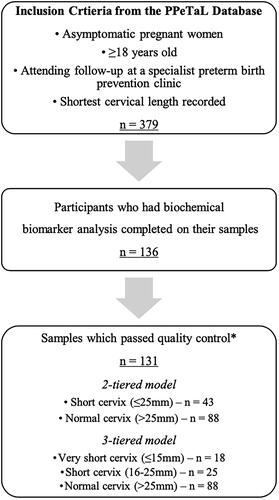
After applying all inclusion and exclusion criteria, a total of 131 samples were eligible for analysis (). The subjects analysed had samples collected from March 2018 to April 2019, ranging from 15 + 2 to 24 + 3 weeks’ gestation. The subsequent CL allowed for further participant classification – two-tiered model: Normal CL (n = 88) and Short CL (n = 43); and three-tiered model: Normal CL (n = 88), Short CL (n = 25), and Very Short CL (n = 18).
Figure 1. Study design and analysis. Flow chart depicting the inclusion and exclusion criteria of participants for this study, refined from the PPeTaL database (Leow et al. Citation2020). *Quality control – five samples were excluded from the analysis as they were low volume samples and unable to have the biochemical analysis completed.
The participants’ demographics are displayed in . The negative relationship between CL and PTB is demonstrated, with the Normal, Short and Very Short CL groups reporting a PTB rate of 19.3%, 28.0% and 61.1% respectively (p-value = 0.001). Additionally, 27.8% of the Very Short CL group were extreme PTB (<28 weeks’ gestation) compared to only 1.1% in the Normal CL group (p-value < 0.001). 11.1% (n = 2) in the Very Short CL group had a parity ≥4, compared to 1.1% (n = 1) and 0% (n = 0) in the Normal and Short CL groups respectively (p-value = 0.03). 53.4% of those in the Normal CL and 68.0% in the Short CL group reported an absence of past miscarriages compared to 27.8% in the Very Short CL group (p-value = 0.03). Maternal age, maternal BMI, smoking rates, fertility assisted pregnancy, history of uterine malformations and previous cervical surgery were comparable between the three groups (p-values > 0.05, ).
Table 1. Participants’ demographic details categorised in the three-tiered model – normal (CL >25 mm), Short (CL 16–25 mm), Very Short (CL ≤15 mm).
In the two-tiered model, IL-1RA and ECM1 demonstrated a statistically significant relationship with a short CL (≤25 mm) compared to Normal CL (>25 mm) (; p-value 0.046, OR 1.001 and p-value 0.025, OR 1.004 respectively). Upon separating the Short CL group (≤25 mm) to Short (CL 16–25 mm) and Very Short (CL ≤ 15 mm), the association was statistically significant when IL-1RA and ECM1 were analysed for Normal CL relative to Short CL (; p-value = 0.003, RRR = 1.001, and p-value = 0.007, RRR = 1.006 respectively), but not Very Short CL (; IL-1RA to Very Short p-value = 0.647, RRR = 1.000, and ECM1 to Very Short p-value = 0.580, RRR = 1.002). In the two-tiered model, 32 out of 43 women (74.4%) in the Short CL group had an entry level CL > 25mm.
Table 2. Odds ratios and p-values for the two-tiered model using standard logistic regression to explore the relationship between IL-1RA or ECM1 and CL.
Table 3. Relative risk ratios and p-values for the multinominal logistic regression analysis between the panel of seven biochemical biomarkers and CL.
The only demographic factor to demonstrate statistical significance with CL in this study was parity, relative to Very Short, but not Short CL (Table S1; p-value = 0.049, RRR = 1.564 and p-value = 0.287, RRR = 1.271 respectively). Upon combining IL-1RA, ECM1 and parity in a multivariate analysis, the association did not demonstrate statistical significance (Table S2; p-values 0.549, 0.352, 0.159 respectively). Regarding the other five biochemical biomarkers (GGH, VDBP, TIMP-1, PEDF, LAMC2), the relationship between them and the shortest CL did not demonstrate statistical significance in this study ().
Discussion
The aim of this study was to analyse the predictive value of seven biochemical biomarkers in identifying subsequent premature cervical shortening. The biomarkers analysed have been associated with processes pertinent to labour, namely inflammation, stress, hormonal regulation, vascular modification, and matrix remodelling () (Leow et al. Citation2020). Cervical remodelling is largely influenced by inflammatory cells, cytokines and extracellular matrix transformations (Junqueira et al. Citation1980, Ellwood and Anderson Citation1981, Sennstrom et al. Citation2000). In normal pregnancy, cervical softening and dilation occurs at term in preparation for labour. However, premature cervical remodelling can be problematic due to its association with preterm labour and delivery (Kushnir et al. Citation1990, Iams et al. Citation1996, Timmons et al. Citation2010). Given that 74.4% of the Short CL group in the two-tiered model had an entry level CL >25 mm, this reiterates the potential benefit of identifying biomarkers which predict premature cervical shortening, as a one off, real-time TVS CL measurement does not necessarily provide adequate prospective insight. This study identified two biomarkers, IL-1RA and ECM1 which may be involved in these processes and demonstrated associations with premature cervical shortening below 25 mm ().
Figure 2. The seven candidate biochemical biomarkers and the underlying biological processes with which are associated, modified from Leow et al. (Citation2020). Inflammation, stress, hormonal regulation, matrix remodelling, and vascular modification are key to cervical change, and each of the candidate biochemical biomarkers have been linked with these processes (Leow et al., Citation2020).
IL-1RA is an anti-inflammatory protein, acting via its antagonism of the interleukin-1 receptor and downstream pro-inflammatory cytokines (Ellwood and Anderson Citation1981, Arend et al. Citation1998). The association of IL-1RA with PTB is well established in the literature, with the results of this study adding to this foundation (Ruiz et al. Citation2012, Belousova et al. Citation2019, Leow et al. Citation2020). This study found a weakly positive association between CL and IL-1RA ( and ), whereas other literature displays negative relationships between IL-1RA and the inflammatory nature of labour (Heng et al. Citation2014, Liong et al. Citation2015). However, direct comparison of these studies is limited by the discrepant populations investigated, for example, other literature focussed on term births (Heng et al. Citation2014), symptomatic women (Liong et al. Citation2015) or their outcomes are defined as PTB rather than CL (Ruiz et al. Citation2012, Belousova et al. Citation2019). Comparatively, ECM1 plays a role in extracellular matrix remodelling, cellular proliferation and angiogenesis (Chan Citation2004). Therefore, it may be involved in cervical collagenolysis and maturation, in preparation for delivery (Winkler et al. Citation1999). This relationship is less widely explored in current research, and the findings of this study require additional investigation to determine any downstream clinical utility.
The biomarkers IL-1RA and ECM1 displayed statistical significance in the three-tiered model in predicting Short, but not Very Short CL (). These two populations are distinct, with a much higher rate of PTB reported in the Very Short (61.1%) compared to the Short CL group (28.0%) () (Owen et al. Citation2001). This incongruency appears counterintuitive, but it may suggest that IL-1RA and ECM1 do not capture all the mechanisms that underpin cervical change. Given that majority of the existing literature explores a standard CL cut-off for clinical significance at 25 mm (Iams et al. Citation1996, Owen et al. Citation2001, Hughes et al. Citation2016), if ECM1 or IL-1RA is able to predict which cervices will shorten below 25 mm (as demonstrated in ), irrespective of shortening specifically below 15 mm, they may still prove useful. When combined in a multivariate model, these biomarkers were unable to demonstrate statistical significance in predicting cervical shortening (supplemental Table S2) contrary to recommendations in the literature suggesting a combinatory approach to predicting PTB (Heng et al. Citation2015, Leow et al. Citation2020). This may suggest that the two biomarkers work via different pathways. Despite statistical significance between IL-1RA and ECM1 with cervical shortening to ≤25mm, the potential for clinical utility is less clear. The RRR can be interpreted as the increased relative risk of a short cervix for every one unit increase in the biomarker of interest. With a RRR of 1.001 (IL-1RA) and 1.004 (ECM1), it is uncertain if this difference would be clinically detectible. However, given the ability to pick statistical significance in a small cohort, it may reinforce the potential of these results.
Other significant findings of this study include the demographic variability identified between the three outcome groups (). Contextually, these may be validated in the setting of their differing CL. The Very Short CL group had a significantly higher rate of PTB and past miscarriages, justified by their shortened cervices (Hughes et al. Citation2016). The statistically significant difference in parity ≥4 must be interpreted with caution, as the discrepancy between absolute numbers is minimal (). The marginal statistical significance between parity and CL remains of unclear clinical importance (Table S1). Furthermore, this study did not demonstrate statistical significance of the five other biochemical biomarkers in predicting premature cervical shortening. This is in comparison to some of the existing literature, especially that around the value of VDBP (Liong et al. Citation2013, Liong et al. Citation2015, Kook et al. Citation2018) and TIMP-1 (Yoo et al. Citation2017) in predicting labour or PTB. However, given the absence of extensive literature exploring the use of biomarkers to predict premature cervical shortening in asymptomatic pregnant women, there is limited validity in directly comparing current knowledge to the findings of this study.
Strengths of this study include using a well-defined, previously published cohort of patients and examining specific biomarkers relevant to PTB in relation to predicting premature cervical shortening in a subset of this cohort. Limitations include being retrospective data analyses of a relatively small sample size; the participants being high-risk for PTB, therefore minimally representative of the general population; the possibility that not all PTB prevention clinic attendees were included, and/or had CL measurements, and/or biomarker analyses; and participants were not a randomised sample as they volunteered to participate, therefore, were not a homogenous group. Furthermore, two thirds of women had a past history of PTB (the highest risk category), however, collectively all women were at higher risk of PTB even if their degree of risk slightly differed. The clinical cost-effectiveness of utilising these biomarkers in practice is undetermined, although it is likely to be less costly than repeated TVS CL measurements. Ultimately, a large prospective cohort study is needed to explore the clinical utility of ECM1 and IL-1RA in predicting premature cervical shortening. These biomarkers could be further investigated by exploring relationships between various biomarker cut-off levels and premature cervical shortening below 25 mm.
Conclusion
This study identified two CVF biochemical biomarkers, IL-1RA and ECM1, which demonstrate associations with premature cervical shortening in high-risk, asymptomatic pregnant women. Further investigation regarding the predictive capabilities and possible clinical utility of these biomarkers is required, with a view to ultimately reduce the burden of PTB and its sequelae.
Supplemental Material
Download MS Word (17.5 KB)Acknowledgements
We thank all the women who participated in the PPeTaL study, and the staff members involved in the PPeTaL study from the University of Melbourne, the Royal Women’s Hospital, and the Mercy Hospital for Women. The findings of this paper have been presented at the Perinatal Society of Australia and New Zealand Annual Congress 2022 as a poster abstract.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, Di Salvo, L., upon reasonable request.
Additional information
Funding
References
- Arend, W. P., et al., 1998. Interleukin-1 receptor antagonist: role in biology. Annual Review of Immunology, 16, 27–55.
- Belousova, V. S., et al., 2019. Polymorphism of the IL-1beta, TNF, IL-1RA and IL-4 cytokine genes significantly increases the risk of preterm birth. Biochemistry. Biokhimiia, 84 (9), 1040–1046.
- Blencowe, H., et al., 2012. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet (London, England), 379 (9832), 2162–2172.
- Chan, I., 2004. The role of extracellular matrix protein 1 in human skin. Clinical and Experimental Dermatology, 29 (1), 52–56.
- Conde-Agudelo, A., et al., 2011. Novel biomarkers for the prediction of the spontaneous preterm birth phenotype: a systematic review and meta-analysis. BJOG : An International Journal of Obstetrics and Gynaecology, 118 (9), 1042–1054.
- Ellwood, D. A. and Anderson, A. B. M., 1981. The cervix in pregnancy and labour: clinical and biochemical investigations. Edinburgh: Churchill Livingstone.
- Georgiou, H. M., et al., 2015. Predicting preterm labour: current status and future prospects. Disease Markers, 2015, 435014.
- Goldenberg, R. L., et al., 2008. Epidemiology and causes of preterm birth. Lancet (London, England), 371 (9606), 75–84.
- Heng, Y. J., et al., 2014. The interplay of the interleukin 1 system in pregnancy and labor. Reproductive Sciences (Thousand Oaks, Calif.), 21 (1), 122–130.
- Heng, Y. J., et al., 2015. Human cervicovaginal fluid biomarkers to predict term and preterm labor. Frontiers in Physiology, 6, 151.
- Hodek, J. M., Von Der Schulenburg, J. M. and Mittendorf, T., 2011. Measuring economic consequences of preterm birth - methodological recommendations for the evaluation of personal burden on children and their caregivers. Health Economics Review, 1 (1), 6.
- Hughes, K., et al., 2016. Cervical length as a predictor for spontaneous preterm birth in high-risk singleton pregnancy: current knowledge. Ultrasound in Obstetrics & Gynecology : The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 48 (1), 7–15.
- Hughes, K., et al., 2017. Outcomes and predictive tests from a dedicated specialist clinic for women at high risk of preterm labour: a ten year audit. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 57 (4), 405–411.
- Iams, J. D., et al., 1996. The length of the cervix and the risk of spontaneous premature delivery. National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The New England Journal of Medicine, 334 (9), 567–572.
- Jin, W., et al., 2021. The contemporary value of dedicated preterm birth clinics for high-risk singleton pregnancies: fifteen-year outcomes from a leading maternal centre. Journal of Perinatal Medicine, 49(9), 1048–1057.
- Junqueira, L. C., et al., 1980. Morphologic and histochemical evidence for the occurrence of collagenolysis and for the role of neutrophilic polymorphonuclear leukocytes during cervical dilation. American Journal of Obstetrics and Gynecology, 138 (3), 273–281.
- Kook, S. Y., et al., 2018. Vitamin D-binding protein in cervicovaginal fluid as a non-invasive predictor of intra-amniotic infection and impending preterm delivery in women with preterm labor or preterm premature rupture of membranes. PLoS One, 13 (6), e0198842.
- Kushnir, O., et al., 1990. Vaginal ultrasonographic assessment of cervical length changes during normal pregnancy. American Journal of Obstetrics and Gynecology, 162 (4), 991–993.
- Leow, S. M., et al., 2020. Preterm birth prediction in asymptomatic women at mid-gestation using a panel of novel protein biomarkers: the Prediction of PreTerm Labor (PPeTaL) study. American Journal of Obstetrics & Gynecology MFM, 2 (2), 100084.
- Liong, S., et al., 2013. Is vitamin D binding protein a novel predictor of labour? PLoS One, 8 (10), e76490.
- Liong, S., et al., 2015. New biomarkers for the prediction of spontaneous preterm labour in symptomatic pregnant women: a comparison with fetal fibronectin. BJOG : An International Journal of Obstetrics and Gynaecology, 122 (3), 370–379.
- Lockwood, C. J., et al., 1991. Fetal fibronectin in cervical and vaginal secretions as a predictor of preterm delivery. The New England Journal of Medicine, 325 (10), 669–674.
- Moutquin, J. M., 2003. Classification and heterogeneity of preterm birth. BJOG: An International Journal of Obstetrics & Gynaecology, 110 (Suppl 20), 30–33.
- Newnham, J. P., et al., 2014. Strategies to prevent preterm birth. Frontiers in Immunology, 5, 584.
- Owen, J., et al., 2001. Mid-trimester endovaginal sonography in women at high risk for spontaneous preterm birth. JAMA, 286 (11), 1340–1348.
- Parry, S. and Elovitz, M. A., 2014. Pros and cons of maternal cervical length screening to identify women at risk of spontaneous preterm delivery. Clinical Obstetrics and Gynecology, 57 (3), 537–546.
- Petraglia, F. and Visser, G. H., 2009. Prevention and management of preterm labour. The Journal of Maternal-Fetal & Neonatal Medicine, 22 (sup2), 24–30.
- Polettini, J., et al., 2017. Biomarkers of spontaneous preterm birth: a systematic review of studies using multiplex analysis. Journal of Perinatal Medicine, 45 (1), 71–84.
- Ruiz, R. J., et al., 2012. Second trimester maternal plasma levels of cytokines IL-1Ra, Il-6 and IL-10 and preterm birth. Journal of Perinatology : Official Journal of the California Perinatal Association, 32 (7), 483–490.
- Saade, G. R., et al., 2016. Development and validation of a spontaneous preterm delivery predictor in asymptomatic women. American Journal of Obstetrics and Gynecology, 214 (5), 633 e1-633–e24.
- Sennstrom, M. B., et al., 2000. Human cervical ripening, an inflammatory process mediated by cytokines. Molecular Human Reproduction, 6 (4), 375–381.
- Singh, N., et al., 2020. Prevention of preterm birth: proactive and reactive clinical practice-are we on the right track? Placenta, 98, 6–12.
- Son, M. and Miller, E. S., 2017. Predicting preterm birth: cervical length and fetal fibronectin. Seminars in Perinatology, 41 (8), 445–451.
- Timmons, B., Akins, M. and Mahendroo, M., 2010. Cervical remodeling during pregnancy and parturition. Trends in Endocrinology and Metabolism: TEM, 21 (6), 353–361.
- Vernet, G., et al., 2017. The role of PTB clinics: a review of the screening methods, interventions and evidence for preterm birth surveillance clinics for high-risk asymptomatic women. Women s Health Bulletin, 4 (4), e12667.
- Ward, R. M. and Beachy, J. C., 2003. Neonatal complications following preterm birth. Bjog: An International Journal of Obstetrics & Gynaecology, 110 (Suppl 20), 8–16.
- Watson, W. J., et al., 1999. Observations on the sonographic measurement of cervical length and the risk of premature birth. The Journal of Maternal-Fetal Medicine, 8 (1), 17–19.
- Winkler, M., et al., 1999. Collagenolysis in the lower uterine segment during parturition at term: correlations with stage of cervical dilatation and duration of labor. American Journal of Obstetrics and Gynecology, 181 (1), 153–158.
- Yoo, H. N., et al., 2017. Non-invasive prediction of preterm birth in women with cervical insufficiency or an asymptomatic short cervix (</=25 mm) by measurement of biomarkers in the cervicovaginal fluid. PLoS One, 12 (7), e0180878.