

Abstract
Introduction
The number of patients desiring fertility-preserving treatment for endometrial cancer rather than standard surgical management continues to increase.
Objective
We aimed to evaluate the efficacies of fertility-preserving treatments on the live birth rate, remission and relapse rates for women with stage 1a grade 1 endometrial carcinoma to support patient counselling.
Methods
We performed a meta-analysis for our primary outcomes of overall remission and relapse rate, and for secondary analysis, we divided papers into treatment type: systemic progestins, intrauterine progestins or hysteroscopic resection and adjuvant hormonal treatment.
Results
Thirty-five observational studies met inclusion criteria, with a total of 624 patients. Overall, conservative treatment of endometrial cancer showed a remission rate of 77% (95% CI: 70–84%), a relapse rate of 20% (95% CI: 13–27%) and a live birth rate of 20% (95% CI: 15–25%) with more favourable outcomes for the hysteroscopic resection group.
Conclusions
Hysteroscopic resection and adjuvant hormonal treatment had the most favourable fertility and oncological outcomes. Further high-quality prospective multi-centre trials are warranted to determine the optimal treatment regimen and dosage and risk stratification for these patients.
Plain Language Summary
The number of women diagnosed with womb cancer who want to preserve their fertility is increasing. Traditional treatment involves surgery to remove the womb and ovaries, rendering women infertile. Fertility-preserving treatments (e.g. hormone therapy, removing only affected areas) exist but their impact on remission, relapse and fertility is not certain. Our team discovered that for women who underwent fertility-preserving treatment: three in four had cancer remission, one in five had cancer relapse and one in five had a successful birth. More research is needed to work out the best fertility-preserving treatment and identify which women are more likely to have successful pregnancies.
Overall, our research will help to counsel women diagnosed with womb cancer who want to preserve their fertility or are unsuitable for major surgery more effectively.
Introduction
Endometrial carcinoma (EC) is increasing in incidence, affecting 9400 women/year in the United Kingdom (Cancer Research UK Citation2020), primarily driven by a growing obesity epidemic (Raglan et al. Citation2019). In the UK, 3% of women are below 45 years of age at diagnosis (Cancer Research UK Citation2020), with worldwide estimates at 5–7% (Duska et al. Citation2001, Siegel et al. Citation2016, Obermair et al. Citation2020).
Standard surgical management for low-risk tumours comprises total hysterectomy and bilateral salpingo-oophorectomy, with consideration of pelvic lymph-node assessment (Morrison et al. Citation2021). This has excellent survival outcomes (Lajer et al. Citation2012), at the expense of fertility and endocrine function. Women of reproductive-age have lower-stage disease and better stage-specific survival than older women (Lee et al. Citation2007). With women increasingly delaying childbearing (Age of Women Giving Birth Citation2021), many may wish to conserve their reproductive potential and choose fertility-preserving treatments. Non-surgical treatments also have a role for women with significant comorbidities (Terzic et al. Citation2020), although this will not be discussed further here.
Fertility-preserving treatments include progestins, oral (megestrol acetate (MA), medroxyprogesterone acetate (MPA)) and intrauterine (levonorgestrel–intrauterine-system (LNG-IUS)), and gonadotropin-releasing hormone analogs (GnRHa) (Terzic et al. Citation2020). Hysteroscopic resection may be used, usually prior to further hormonal treatment (Alonso et al. Citation2015), which is distinct from hysteroscopic biopsy for diagnosis. The risks of fertility-sparing management options include under-staging of disease and a higher risk of disease progression/relapse, which may ultimately require hysterectomy (Alonso et al. Citation2015). There may be failure to achieve a live-birth despite these risks.
EC guidelines from the British Gynaecological Cancer Society (BGCS) (Morrison et al. Citation2021) and Europe (Concin et al. Citation2021) permit fertility-preserving approaches in selected grade 1/stage 1a EC cases, after careful counselling with regular follow-up. The recommended management is high-dose oral MPA/MA, or consideration of IUS with/without GnRHa. The paucity of data on fertility and oncological outcomes is highlighted, which currently limits confidence in counselling.
There is therefore a need for an updated and comprehensive systematic review of both reproductive and oncological outcomes, focusing on stage 1a/grade 1 EC, reflecting recommended clinical practice.
This paper aims to update the literature by evaluating the efficacies of fertility-preserving EC treatments. The population is reproductive-age women with stage 1a/grade 1 EC desiring fertility. The outcomes are rates of remission, relapse and live-births. A secondary aim is to assess outcomes by treatment-modality where possible.
Methods
Literature search
A systematic review of the following databases was conducted: Medline, Embase, Central, Cochrane, NICE and Web of Science, from database inception to October 2020, for English language publications.
Medical subject headings (MeSH) and free text were combined to generate a subset of citations including studies with endometrial cancer (‘endometr* neoplasm’, ‘endometr* cancer’) and another subset of fertility-preserving treatments (‘fertility preserv’, fertility ‘sparing’, ‘live birth’, ‘pregnancy’), and these subsets were combined. Previous literature reviews were examined for any references not included by the above search strategy.
The population of interest was women with International Federation of Gynecology and Obstetrics (FIGO) stage Ia grade 1 endometrial adenocarcinoma, who desire fertility-preserving treatment. Stage 1A is defined as a tumour confined to the endometrium or less than one-half of the myometrium (Lewin Citation2011). Grade 1 is defined by well differentiated cells (Lewin Citation2011). The interventions were fertility preserving treatments, such as progestins (systemic/intra-uterine), GnRH analogues, hysteroscopic resection or others, in any combination. The outcomes were rates of remission (proportion of all patients who achieved complete response to treatment), relapse (proportion of all patients who relapsed after achieving remission) and of women achieving a live-birth. We did not pre-specify a timeframe for follow-up in our inclusion criteria but recorded this for all studies.
This study was prospectively registered with PROSPERO (CRD42021239714), with a protocol detailing the review question, search strategy, inclusion/exclusion criteria, risk-of-bias assessment and meta-analysis with a plan for assessment of heterogeneity. This review has been conducted in accordance with the AMSTAR-2 criteria (Shea et al. Citation2017).
Study selection and data extraction
Studies were selected if the participants were women with histologically diagnosed grade 1 EC, presumed stage 1a, who underwent fertility-preserving treatments with the purpose of preserving fertility, for the treatment of primary EC. The primary outcomes were rates of live birth, remission and relapse. Both non-randomised (e.g. case reports, observational studies) and randomised studies were included in our review reflecting the available evidence, with very few randomised studies in this field. Exclusion criteria were: not involving stage 1a grade 1 endometrial adenocarcinoma, not involving fertility-preserving treatments, not reporting primary outcomes of interest, review articles, letters and literature that did not provide original data or detailed treatment methods. Case series of fewer than five patients were excluded in order to ensure that centres managing such patients had sufficient experience, and better enable meta-analysis. Conference abstracts were suitable for inclusion if they provided all necessary information.
Two authors (SO and RG) independently screened titles and abstracts. Following this, full texts of shortlisted abstracts were retrieved to assess eligibility for inclusion. Any disagreements between these reviewers were settled by a third reviewer (AO). All duplicates were removed; in cases where the same group had multiple publications with overlapping patient groups, the most recent or complete publication was used, or data combined where it was clearly possible to do so (e.g. where a later publication provided longer-term follow-up data for the same patient group). All excluded papers were coded with a justification for their exclusion from the review.
Baseline characteristics and outcome data were extracted for each study by two authors (SO and OO), achieving consensus, into a table in Microsoft Excel (Microsoft Corporation Citation2018, Redmond, WA). The following data were extracted from each study: population (including median age of patients), study setting, intervention(s), including doses where required, length of follow-up (in months), number of patients, number of patients who achieved complete remission, number of patients who relapsed after complete remission, number of patients who achieved a live birth, and deaths. Rates were calculated for complete remission, relapse and total number of patients who achieved a live birth (number of patients who achieved a live birth divided by total number of patients). This definition of live birth rate was chosen as this reflects what would be of most clinical value to patients.
Risk of bias assessment
A risk of bias assessment using the Methodological Index for Non-Randomised Studies (MINORS) (Slim et al. Citation2003) was conducted by two authors working independently (OO and SO), on all included papers. The items were scored 0 if not reported; 1 when reported but inadequate; and 2 when reported and adequate. The global ideal score is 16 for the included studies.
Statistical analysis
JASP version 0.14.1 (JASP software) (JASP Team Citation2020) was used for statistical analysis. Remission rates, relapse rates and live-birth rates were extracted from each study. Differences in rates with 95% confidence intervals were calculated for each study and for the summary effects. Statistical heterogeneity was assessed with I2 tests and where I2 was greater than 50% results were considered to have significant heterogeneity and a random-effects model was used; otherwise, a fixed-effects model was used.
Results
Study selection
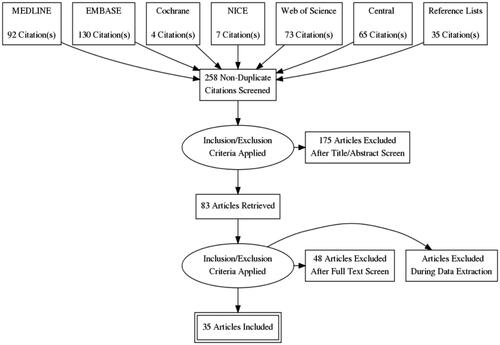
The initial search yielded 367 abstracts, of which 125 were duplicates, leaving 242 abstracts remaining. From 1946 to October 2020, 35 eligible articles were included, with a total of 675 patients across 12 countries (see for a flow diagram). Three primary treatment groups were identified: 441 patients treated with oral progesterone only, 126 patients treated with hysteroscopic resection and adjuvant progestin therapy and 57 patients treated with intrauterine progesterones (LNG-IUS) and adjuvant progesterone therapy. Of the 51 patients not delineated into one of the three groups: one study (14 patients) described intra-uterine photodynamic therapy (Choi Citation2013) and two studies (37 patients) did not report fertility and mortality outcomes for each treatment group (Perri Citation2011, Kudesia Citation2014).
Figure 1. PRISMA flow diagram.
Risk of bias assessment
The risk of bias assessment using the MINORS checklist (Slim et al. Citation2003) is shown in Table S1. The majority of the studies had a clearly stated aim (34 of 35), included consecutive patients (21 of 35) and appropriate endpoints (33 of 35). Over half were prospective cohort studies (21 of 35). Only one study had blinded assessment of outcomes. We defined appropriate follow-up to be at least 5 years (Gallos et al. Citation2012), and this was satisfied in only nine of 35 studies. No studies had a loss to follow up of >5%.
Overall results
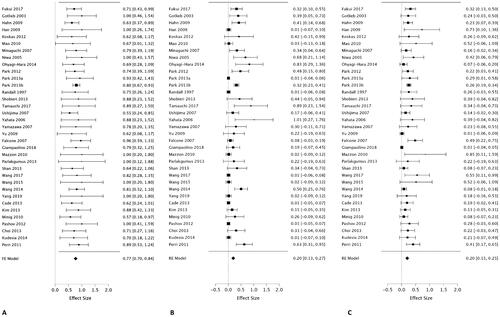
Thirty-five studies were included in our review, involving 675 patients from 12 countries (Randall and Kurman Citation1997, Gotlieb et al. Citation2003, Niwa et al. Citation2005, Yahata et al. Citation2006, Minaguchi et al. Citation2007, Ushijima et al. Citation2007, Yamazawa et al. Citation2007, Hahn et al. Citation2009, Han et al. Citation2009, Yu et al. Citation2009, Mao et al. Citation2010, Mazzon et al. Citation2010, Minig et al. Citation2011, Perri et al. Citation2011, Koskas et al. Citation2012, H. Park et al. Citation2012, Pashov et al. Citation2012, Cade et al. Citation2013, Choi et al. Citation2013, Kim et al. Citation2013, J.-Y. Park et al. Citation2013b, Citation2013a, B.-E. Shan et al. Citation2013, Shobeiri et al. Citation2013, Kudesia et al. Citation2014, Parlakgumus et al. Citation2014, C.-J. Wang et al. Citation2014, Ohyagi-Hara et al. Citation2015, Q. Wang et al. Citation2015, Falcone et al. Citation2017, Fukui et al. Citation2017, F. Wang et al. Citation2017, Tamauchi et al. Citation2018, Giampaolino et al. Citation2019, H.-C. Yang et al. Citation2019). The median ages and median length of follow up are reported in Table S2. Due to similarity of patient population, study type and outcomes reported, combination of data into a meta-analysis was undertaken for overall results and by treatment type. Meta-analysis of all included studies found the fertility-preserving therapies had a combined remission rate of 77% (95% CI: 70–84%) with an I2 value of 0.0%, indicating low heterogeneity (). The combined relapse rate of 20% (95% CI: 13–27%) with I2 of 88% indicating significant heterogeneity (). The proportion of women achieving a live birth was 20% (95% CI: 15–25%) with I2 of 59% indicating significant heterogeneity among studies (). The number of women actively trying to conceive after complete remission was not consistently reported, nor was the proportion receiving assisted reproductive treatments, and so reliable summary data for these could not be described.
Figure 2. Remission rate (A), relapse rate (B) and proportion of live births (C) following fertility-preserving treatment in endometrial cancer.
Oral progestins
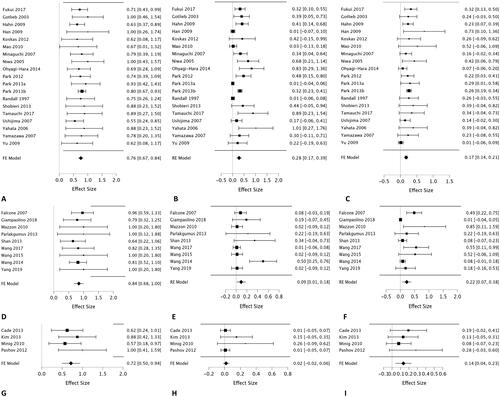
Nineteen studies containing 441 patients reported primary treatment with oral progestin therapy (Randall and Kurman Citation1997, Gotlieb et al. Citation2003, Niwa et al. Citation2005, Yahata et al. Citation2006, Minaguchi et al. Citation2007, Ushijima et al. Citation2007, Yamazawa et al. Citation2007, Hahn et al. Citation2009, Han et al. Citation2009, Yu et al. Citation2009, Mao et al. Citation2010, Koskas et al. Citation2012, H. Park et al. Citation2012, J.-Y. Park et al. Citation2013b, Citation2013a, Shobeiri et al. Citation2013, Ohyagi-Hara et al. Citation2015, Fukui et al. Citation2017, Tamauchi et al. Citation2018). These included MPA (20–1000 mg), MA (10–400 mg), norethisterone acetate (5 mg), nomegestrol acetate (5 mg) and hydroxyprogesterone caproate (doses not disclosed). The complete remission rate was 76% (95% CI: 67–84%) (). The I2 value was 0.0%, indicating no observed heterogeneity among studies. Of those who achieved complete remission, there was a relapse rate of 28% (95% CI: 17–39%) (), The I2 value was 86%, indicating significant heterogeneity among studies. The live birth rate was 17% (95% CI: 14–21%) (). The I2 value was 48%, indicating no significant heterogeneity among the studies.
Figure 3. Remission rate (A), relapse rate (B) and proportion of live births (C) following oral progesterone therapy. Remission rate (D), relapse rate (E) and proportion of live births (F) following hysteroscopic resection and adjuvant progesterone therapy. Remission rate (G), relapse rate (H) and proportion of live births (I) following intrauterine progesterone therapy.
Hysteroscopic resection and adjuvant progestin
Nine studies containing 126 patients reported on hysteroscopic resection with adjuvant progestins (Yu et al. Citation2009, Mazzon et al. Citation2010, B.-E. Shan et al. Citation2013, Parlakgumus et al. Citation2014, C.-J. Wang et al. Citation2014, Q. Wang et al. Citation2015, Falcone et al. Citation2017, F. Wang et al. Citation2017, Giampaolino et al. Citation2019). Adjuvant progestins included oral MA (80–320 mg daily)/MPA (250–500 mg daily)/oral dydrogesterone (10 mg daily), or the LNG-IUS (20 µg daily). The complete remission rate was 84% (95% CI: 68–100%) (). The I2 value was 0.0%, indicating no observed heterogeneity among studies. Of those who achieved complete remission, there was a relapse rate of 9.3% (95% CI: 0.0–18%) (), The I2 value was 70%, indicating significant heterogeneity among studies. Among the patients who achieved complete remission, the live birth rate was 22% (95% CI: 7.0–38%) (), the I2 value was 83%, indicating significant heterogeneity among the studies.
Intrauterine progestins and adjuvant hormonal therapy
Four studies containing 57 patients reported using the LNG-IUS (20 µg daily) alongside systemic progestins including oral MA (400–500 mg daily), or intramuscular GnRH analogues (leuprorelin acetate 3.75 mg monthly) (Minig et al. Citation2011, Pashov et al. Citation2012, Cade et al. Citation2013, Kim et al. Citation2013). The complete remission rate was 72% (95% CI: 50–94%) (). The I2 value was 0.0%, indicating no observed heterogeneity among studies. Of those who achieved complete remission, there was a relapse rate of 2.1% (95% CI: 0.0–5.9%) (). The I2 value was <0.1%, indicating no observed heterogeneity among studies. The live birth rate was 14% (95% CI: 4.0–23%) (), the I2 value was 0.0%, indicating no significant heterogeneity among the studies ().
Discussion
This systematic review and meta-analysis provides a comprehensive summary of the evidence regarding oncological and reproductive outcomes following different fertility-preserving managements for stage 1a grade 1 EC. These data show that fertility-sparing management of EC results in remission rates of 77% (95% CI: 70–84%), with relapse rates of 20% (95% CI: 13–27%). The proportion of women achieving a live birth is only 20% (95% CI: 15–25%), despite fertility preservation being a main aim of treatment.
Analysis by treatment type suggests that hysteroscopic resection with adjuvant progestin therapy results in the highest proportion of patients delivering live births (22%, 95% CI: 7.0–38%) and entering remission (84%, 95% CI: 68–100%), with relatively low rates of relapse (9.3%, 95% CI: 0.0–18%). Oral progestins are associated with similar but slightly lower rates of live birth (19%, 95% CI: 13–25%), and remission (77%, 95% CI: 69–84%), but by far the highest rates of relapse of 28% (95% CI: 17–39%). Intrauterine progestins result in the lowest rates of live births (14%, 95% CI: 4.0–23%) and remission (72%, 95% CI: 50–94%), with the lowest rates of relapse (2.1%, 95% CI: 0.0–5.9%). Reassuringly, regardless of treatment protocol, patients who relapsed were successfully treated with a secondary course of progesterone therapy and/or hysterectomy, with no deaths within the follow-up periods reported.
This comprehensive review provides an update of fertility-preserving management for stage 1a grade 1 EC, with a prospectively registered protocol, and synthesis of primary outcome data with meta-analysis. This builds upon previous reviews, which did not assess remission rate (Guillon et al. Citation2019), live-birth-rate (Fan et al. Citation2018) or comprised case-reports and high grade/stage patients outside usual practice (Lucchini et al. Citation2021). We focused on EC rather than considering EH in combination, to provide relevant data for oncology patients. This study excluded cases of fewer than five cases, reducing publication bias. The use of a random-effects meta-analysis helps account for variability between studies.
We acknowledge several limitations. The quality of this review is limited by the available evidence. Studies were heterogeneous in size, findings and treatment protocols. Most studies are small case series, retrospective and lack blinded assessment, indicating a high risk of bias. Fewer than half of studies had 5-year follow up, which may lead to under-reporting of primary outcomes including relapse and live births. Most studies did not report the number of patients actively trying to conceive, or those actively managed by a reproductive-health team, as recommended. Our inclusion of all women in the denominator may have decreased the percentage of women achieving a live birth; however, we feel this approach is justified given that all women initially desired fertility-preservation, and is relevant to patients considering this approach over standard care. The number of patients in each treatment group substantially differed, with the majority of included patients treated with oral progestins. The lower number in other groups limits the accuracy of findings, and the confidence in making comparisons between treatment groups. The omission of studies describing patients with grade 2 disease (W. Shan et al. Citation2021) can be seen as a study limitation in light of recent ESGO/ESHRE/ESGE guidelines allowing consideration of fertility-preservation in such cases after careful counselling, as discussed later (Rodolakis et al. Citation2023).
Overall summary outcomes are similar to previous systematic reviews, which found that hysteroscopic resection with adjuvant progestin therapy achieved the highest rate of complete remission and pregnancy rates (Gallos et al. Citation2012, Fan et al. Citation2018, Lucchini et al. Citation2021). These results are of major importance to women with EC considering fertility-preserving management. Oral progestins are most commonly given for this indication across Europe, followed by LNG-IUS (La Russa et al. Citation2018), yet they may not be the most effective treatments. Hysteroscopic resection of EC is less commonly performed in the United Kingdom and Europe and was not referenced in BGCS guidelines until this year (Morrison et al. Citation2021). The new ESGO/ESHRE/ESGE guidelines now support the approach of hysteroscopic resection followed by oral/intra-uterine progestins (Rodolakis et al. Citation2023), and so this is likely to become more widespread in the coming years.
Possible explanations for this are that resection of the primary lesion along with adjacent endometrium and 3–4 mm of myometrium ensures adequate removal of tumour, and better evaluation of margins and depth of invasion over hysteroscopic biopsy, which may be particularly important given that there is no hysterectomy specimen (De Marzi et al. Citation2015). Concerns have been raised regarding the seeding of tumour cells into the peritoneum during hysteroscopy, with a recent systematic review finding this to be significant for intrauterine pressures above 80 mmHg (Dong et al. Citation2021). However, there is lack of evidence for this in lower stage disease, and no evidence of peritoneal spread among the case series reviewed.
Another potential complication is the risk of intrauterine adhesions, which may adversely impact surveillance biopsies and embryo implantation. This particularly occurs after resection, which damages the basilar layer of the endometrium across widespread or opposing areas of the cavity (Deans and Abbott Citation2010). There is limited evidence on the incidence of intra-uterine adhesions following hysteroscopic resection of EC (or EH), although a case series of 23 patients reported no instances of intra-uterine adhesions following EC/EH resection, on follow-up hysteroscopic biopsy for a median 25 months (De Marzi et al. Citation2015).
All patients treated with hysteroscopic resection received adjuvant progestin, and so are not at risk of undertreatment. The question is therefore whether hysteroscopic resection confers additional benefit over oral/intra-uterine progesterone alone, and whether this outweighs potential risks. This question is now amenable to consideration in a prospective, multi-centre, randomised controlled trial. Weight loss rates and use of metformin therapy and treatment adjuncts were not assessed in this study, but both have been found to be associated with response in EC and EH (B.-Y. Yang et al. Citation2020, Barr et al. Citation2021, Chae-Kim et al. Citation2021).
We considered only grade 1 stage 1a EC, as this was included within national guidelines at the time of study design; however, the fertility-sparing management of grade 2 stage 1a disease is now included within ESGO/ESHRE/ESGE guidelines (Rodolakis et al. Citation2023). A systematic review of patients with grade 2 disease found poorer overall rates of complete response (64.3%), relapse (23.8%) and live births (eight live births in 54 patients) (Giampaolino et al. Citation2022). Fertility-sparing management in this context may be appropriate in certain women after very careful counselling; however, evidence is limited, and fertility and long-term oncological outcomes may not be as reassuring as for grade 1 disease.
The role of molecular classification in the fertility-sparing management of EC remains to be fully determined. Patients with Lynch syndrome are more likely to develop EC at an earlier age and therefore may have greater interest in fertility preservation (Dominguez-Valentin et al. Citation2020). However, mismatch-repair deficiency appears to be associated with significantly reduced treatment response (Chung et al. Citation2021), and many gynaecological oncologists exclude patients from non-surgical management for this reason (La Russa et al. Citation2018). Mismatch-repair-deficiency (on immunohistochemistry) does not predict failure to achieve complete response after hysteroscopic resection and progestins, but is a highly specific predictor of recurrence (Raffone et al. Citation2021), and small case series have shown patients with confirmed Lynch syndrome have high rates of recurrence and often fail to achieve pregnancy (Catena et al. Citation2022). Whilst routine screening for Lynch syndrome is now standard-of-care in all EC patients, current guidelines find insufficient evidence to offer recommendations either for or against the consideration of fertility-preserving management in these patients (Concin et al. Citation2021, Morrison et al. Citation2021, Rodolakis et al. Citation2023). The management of other molecular subtypes within the Cancer Genome Atlas classification is similarly undefined, although p53 abnormal tumours are likely to have a poorer prognosis (Arciuolo et al. Citation2022). Other novel biomarkers such as ESR1, WFDC2 and B-cell lymphoma show early promise in predicting cancer progression and prognosis and may have a future role in patient selection (Travaglino et al. Citation2018, Coll-de la Rubia et al. Citation2020). Future studies should routinely report immunohistochemical/molecular profile to enable better patient stratification and identification of high-risk groups.
Conclusions
This meta-analysis reports the reproductive and oncological outcomes of fertility-sparing treatments of EC, thus enabling optimal counselling for women considering this approach. The quality of available data is generally low, with often inadequate duration of follow-up. These results suggest that hysteroscopic resection followed by progestin therapy may produce superior rates of remission and live birth rates compared to other fertility-sparing management options. Further high-quality prospective multi-centre trials are warranted to determine the optimal treatment regime for these patients.
Author contributions
MO: study selection, data extraction, risk of bias assessment, statistical analysis, manuscript drafting and revision.
SO: study selection, data extraction, risk of bias assessment, manuscript drafting and revision.
RG: study selection and manuscript revision.
AO: conceptualisation, supervision and manuscript revision.
Supplemental Material
Download MS Word (10.9 KB)Supplemental Material
Download MS Word (13.3 KB)Acknowledgements
The authors would like to thank Jacqueline Smith, librarian at University College London library services, for her assistance with the literature search.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, MO, upon reasonable request.
Additional information
Funding
References
- Age of Women Giving Birth, 2021. Office for National Statistics. Available from: https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/ageofwomengivingbirth [Accessed 10 Feb 2021].
- Alonso, S., et al., 2015. Hysteroscopic surgery for conservative management in endometrial cancer: a review of the literature. Ecancermedicalscience, 9 (February), 505.
- Arciuolo, D., et al., 2022. TCGA molecular prognostic groups of endometrial carcinoma: current knowledge and future perspectives. International Journal of Molecular Sciences, 23 (19), 11684.
- Barr, C.E., et al., 2021. Weight loss during intrauterine progestin treatment for obesity-associated atypical hyperplasia and early-stage cancer of the endometrium. Cancer Prevention Research, 14 (11), 1041–1050.
- Cade, T.J., et al., 2013. Long-term outcomes after progestogen treatment for early endometrial cancer. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 53 (6), 566–570.
- Cancer Research UK, 2020. Uterine cancer incidence statistics. Cancer Research UK. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/uterine-cancer/incidence#heading-Two [Accessed 11 Mar 2020].
- Catena, U., et al., 2022. Fertility-sparing treatment for endometrial cancer and atypical endometrial hyperplasia in patients with lynch syndrome: molecular diagnosis after immunohistochemistry of MMR proteins. Frontiers of Medicine, 9 (August), 948509.
- Chae-Kim, J., et al., 2021. Outcomes of women treated with progestin and metformin for atypical endometrial hyperplasia and early endometrial cancer: a systematic review and meta-analysis. International Journal of Gynecological Cancer, 31 (12), 1499–1505.
- Choi, M.C., et al., 2013. Fertility preservation via photodynamic therapy in young patients with early-stage uterine endometrial cancer: a long-term follow-up study. International Journal of Gynecological Cancer, 23 (4), 698–704.
- Chung, Y.S., et al., 2021. Mismatch repair status influences response to fertility-sparing treatment of endometrial cancer. American Journal of Obstetrics and Gynecology, 224 (4), 370.e1–370.e13.
- Coll-de la Rubia, E., et al., 2020. Prognostic biomarkers in endometrial cancer: a systematic review and meta-analysis. Journal of Clinical Medicine, 9 (6), 1900.
- Concin, N., et al., 2021. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. International Journal of Gynecological Cancer, 31 (1), 12–39.
- De Marzi, P., et al., 2015. Hysteroscopic resection in fertility-sparing surgery for atypical hyperplasia and endometrial cancer: safety and efficacy. Journal of Minimally Invasive Gynecology, 22 (7), 1178–1182.
- Deans, R. and Abbott, J., 2010. Review of intrauterine adhesions. Journal of Minimally Invasive Gynecology, 17 (5), 555–569.
- Dominguez-Valentin, M., et al., 2020. Cancer risks by gene, age, and gender in 6350 carriers of pathogenic mismatch repair variants: findings from the prospective lynch syndrome database. Genetics in Medicine, 22 (1), 15–25.
- Dong, H., et al., 2021. Whether preoperative hysteroscopy increases the dissemination of endometrial cancer cells: a systematic review and meta-analysis. The Journal of Obstetrics and Gynaecology Research, 47 (9), 2969–2977.
- Duska, L.R., et al., 2001. Endometrial cancer in women 40 years old or younger. Gynecologic Oncology, 83 (2), 388–393.
- Falcone, F., et al., 2017. Fertility preserving treatment with hysteroscopic resection followed by progestin therapy in young women with early endometrial cancer. Journal of Gynecologic Oncology, 28 (1), e2.
- Fan, Z., et al., 2018. Fertility-preserving treatment in young women with grade 1 presumed stage IA endometrial adenocarcinoma: a meta-analysis. International Journal of Gynecological Cancer, 28 (2), 385–393.
- Fukui, Y., et al., 2017. Polycystic ovarian morphology may be a positive prognostic factor in patients with endometrial cancer who achieved complete remission after fertility-sparing therapy with progestin. Asian Pacific Journal of Cancer Prevention, 18 (11), 3111–3116.
- Gallos, I.D., et al., 2012. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: a systematic review and metaanalysis. American Journal of Obstetrics and Gynecology, 207 (4), 266.e1–266.e12.
- Giampaolino, P., et al., 2019. Hysteroscopic endometrial focal resection followed by levonorgestrel intrauterine device insertion as a fertility-sparing treatment of atypical endometrial hyperplasia and early endometrial cancer: a retrospective study. Journal of Minimally Invasive Gynecology, 26 (4), 648–656.
- Giampaolino, P., et al., 2022. Fertility-sparing approach in patients with endometrioid endometrial cancer grade 2 stage IA (FIGO): a qualitative systematic review. BioMed Research International, 2022, 4070368-15.
- Gotlieb, W.H., et al., 2003. Outcome of fertility-sparing treatment with progestins in young patients with endometrial cancer. Obstetrics and Gynecology, 102 (4), 718–725.
- Guillon, S., et al., 2019. A systematic review and meta-analysis of prognostic factors for remission in fertility-sparing management of endometrial atypical hyperplasia and adenocarcinoma. International Journal of Gynaecology and Obstetrics, 146 (3), 277–288.
- Hahn, H.-S., et al., 2009. Conservative treatment with progestin and pregnancy outcomes in endometrial cancer. International Journal of Gynecological Cancer, 19 (6), 1068–1073.
- Han, A.R., et al., 2009. Pregnancy outcomes using assisted reproductive technology after fertility-preserving therapy in patients with endometrial adenocarcinoma or atypical complex hyperplasia. International Journal of Gynecological Cancer, 19 (1), 147–151. https://ijgc.bmj.com/content/19/1/147.abstract.
- JASP Team, 2020. JASP (version 0.14.1). Available from: https://jasp-stats.org/.
- Kim, M.K., et al., 2013. Combined medroxyprogesterone acetate/levonorgestrel–intrauterine system treatment in young women with early-stage endometrial cancer. American Journal of Obstetrics and Gynecology, 209 (4), 358.e1–358.e4.
- Koskas, M., et al., 2012. Progestin treatment of atypical hyperplasia and well-differentiated adenocarcinoma of the endometrium to preserve fertility. Anticancer Research, 32 (3), 1037–1043.
- Kudesia, R., et al., 2014. Reproductive and oncologic outcomes after progestin therapy for endometrial complex atypical hyperplasia or carcinoma. American Journal of Obstetrics and Gynecology, 210 (3), 255.e1–255.e4.
- La Russa, M., et al., 2018. Conservative management of endometrial cancer: a survey amongst European clinicians. Archives of Gynecology and Obstetrics, 298 (2), 373–380.
- Lajer, H., et al., 2012. Survival after stage IA endometrial cancer; can follow-up be altered? A Prospective Nationwide Danish Survey. Acta Obstetricia et Gynecologica Scandinavica, 91 (8), 976–982.
- Lee, N.K., et al., 2007. Prognostic factors for uterine cancer in reproductive-aged women. Obstetrics and Gynecology, 109 (3), 655–662.
- Lewin, S.N., 2011. Revised FIGO staging system for endometrial cancer. Clinical Obstetrics and Gynecology, 54 (2), 215–218.
- Lucchini, S.M., et al., 2021. Updates on conservative management of endometrial cancer in patients younger than 45 years. Gynecologic Oncology, 161 (3), 802–809.
- Mao, Y., et al., 2010. Outcomes of conservative therapy for young women with early endometrial adenocarcinoma. Fertility and Sterility, 93 (1), 283–285.
- Mazzon, I., et al., 2010. Conservative surgical management of stage Ia endometrial carcinoma for fertility preservation. Fertility and Sterility, 93 (4), 1286–1289.
- Microsoft Corporation, 2018. Microsoft Excel (version 2019 16.0). Available from: https://office.microsoft.com/excel.
- Minaguchi, T., et al., 2007. Combined phospho-Akt and PTEN expressions associated with post-treatment hysterectomy after conservative progestin therapy in complex atypical hyperplasia and stage Ia, G1 adenocarcinoma of the endometrium. Cancer Letters, 248 (1), 112–122.
- Minig, L., et al., 2011. Progestin intrauterine device and GnRH analogue for uterus-sparing treatment of endometrial precancers and well-differentiated early endometrial carcinoma in young women. Annals of Oncology, 22 (3), 643–649.
- Morrison, J., et al., 2021. British Gynaecological Cancer Society (BGCS) uterine cancer guidelines: recommendations for practice. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 270, 50–89.
- Niwa, K., et al., 2005. Outcome of fertility-preserving treatment in young women with endometrial carcinomas. British Journal of Gynecology, 112 (3), 317–320.
- Obermair, A., et al., 2020. Fertility-sparing treatment in early endometrial cancer: current state and future strategies. Obstetrics & Gynecology Science, 63 (4), 417–431.
- Ohyagi-Hara, C., et al., 2015. Efficacies and pregnant outcomes of fertility-sparing treatment with medroxyprogesterone acetate for endometrioid adenocarcinoma and complex atypical hyperplasia: our experience and a review of the literature. Archives of Gynecology and Obstetrics, 291 (1), 151–157.
- Park, H., et al., 2012. Effectiveness of high-dose progestin and long-term outcomes in young women with early-stage, well-differentiated endometrioid adenocarcinoma of uterine endometrium. Archives of Gynecology and Obstetrics, 285 (2), 473–478.
- Park, J.-Y., et al., 2013a. Hormonal therapy for women with stage Ia endometrial cancer of all grades. Obstetrics and Gynecology, 122 (1), 7–14.
- Park, J.-Y., et al., 2013b. Pregnancy outcomes after fertility-sparing management in young women with early endometrial cancer. Obstetrics and Gynecology, 121 (1), 136–142.
- Parlakgumus, H.A., et al., 2014. Fertility outcomes of patients with early stage endometrial carcinoma. The Journal of Obstetrics and Gynaecology Research, 40 (1), 102–108.
- Pashov, A.I., Tskhay, V.B., and Ionouchene, S.V., 2012. The combined GnRH-agonist and intrauterine levonorgestrel-releasing system treatment of complicated atypical hyperplasia and endometrial cancer: a pilot study. Gynecological Endocrinology, 28 (7), 559–561.
- Perri, T., et al., 2011. Prolonged conservative treatment of endometrial cancer patients: more than 1 pregnancy can be achieved. International Journal of Gynecological Cancer, 21 (1), 72–78.
- Raffone, A., et al., 2021. Mismatch repair-deficiency specifically predicts recurrence of atypical endometrial hyperplasia and early endometrial carcinoma after conservative treatment: a multi-center study. Gynecologic Oncology, 161 (3), 795–801.
- Raglan, O., et al., 2019. Risk factors for endometrial cancer: an umbrella review of the literature. International Journal of Cancer, 145 (7), 1719–1730.
- Randall, T.C. and Kurman, R.J., 1997. Progestin treatment of atypical hyperplasia and well-differentiated carcinoma of the endometrium in women under age 40. Obstetrics and Gynecology, 90 (3), 434–440.
- Rodolakis, A., et al., 2023. ESGO/ESHRE/ESGE guidelines for the fertility-sparing treatment of patients with endometrial carcinoma. Facts, Views & Vision in ObGyn, 15 (1), 3–23.
- Shan, B.-E., et al., 2013. A prospective study of fertility-sparing treatment with megestrol acetate following hysteroscopic curettage for well-differentiated endometrioid carcinoma and atypical hyperplasia in young women. Archives of Gynecology and Obstetrics, 288 (5), 1115–1123.
- Shan, W., et al., 2021. Conservative management of grade 2 stage IA endometrial carcinoma and literature review. The Journal of Obstetrics and Gynaecology Research, 47 (3), 984–991.
- Shea, B.J., et al., 2017. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (Clinical Research ed.), 358 (September), j4008.
- Shobeiri, M.J., et al., 2013. Fertility sparing treatment in young patients with early endometrial adenocarcinoma. Pakistan Journal of Medical Sciences, 29 (2), 651–655.
- Siegel, R.L., Miller, K.D., and Jemal, A., 2016. Cancer Statistics, 2016. CA: A Cancer Journal for Clinicians, 66 (1), 7–30.
- Slim, K., et al., 2003. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ Journal of Surgery, 73 (9), 712–716.
- Tamauchi, S., et al., 2018. Efficacy of medroxyprogesterone acetate treatment and retreatment for atypical endometrial hyperplasia and endometrial cancer. The Journal of Obstetrics and Gynaecology Research, 44 (1), 151–156.
- Terzic, M., et al., 2020. Fertility preservation in endometrial cancer patients: options, challenges and perspectives. Ecancermedicalscience, 14 (May), 1030.
- Travaglino, A., et al., 2018. Loss of B-cell lymphoma 2 immunohistochemical expression in endometrial hyperplasia: a specific marker of precancer and novel indication for treatment: a systematic review and meta-analysis. Acta Obstetricia et Gynecologica Scandinavica, 97 (12), 1415–1426.
- Ushijima, K., et al., 2007. Multicenter phase II study of fertility-sparing treatment with medroxyprogesterone acetate for endometrial carcinoma and atypical hyperplasia in young women. Journal of Clinical Oncology, 25 (19), 2798–2803.
- Wang, C.-J., et al., 2014. Fertility-preserving treatment in young women with endometrial adenocarcinoma: a long-term cohort study. International Journal of Gynecological Cancer, 24 (4), 718–728.
- Wang, F., et al., 2017. Fertility preserved hysteroscopic approach for the treatment of stage Ia endometrioid carcinoma. International Journal of Gynecological Cancer, 27 (9), 1919–1925.
- Wang, Q., et al., 2015. Fertility-conservation combined therapy with hysteroscopic resection and oral progesterone for local early stage endometrial carcinoma in young women. International Journal of Clinical and Experimental Medicine, 8 (8), 13804–13810.
- Yahata, T., et al., 2006. Long-term conservative therapy for endometrial adenocarcinoma in young women. Human Reproduction, 21 (4), 1070–1075.
- Yamazawa, K., et al., 2007. Fertility-preserving treatment with progestin, and pathological criteria to predict responses, in young women with endometrial cancer. Human Reproduction, 22 (7), 1953–1958.
- Yang, B.-Y., et al., 2020. Metformin plus megestrol acetate compared with megestrol acetate alone as fertility-sparing treatment in patients with atypical endometrial hyperplasia and well-differentiated endometrial cancer: a randomised controlled trial. British Journal of Gynecology, 127 (7), 848–857.
- Yang, H.-C., Liu, J.-C., and Liu, F.-S., 2019. Fertility-preserving treatment of stage IA, well-differentiated endometrial carcinoma in young women with hysteroscopic resection and high-dose progesterone therapy. Taiwanese Journal of Obstetrics & Gynecology, 58 (1), 90–93.
- Yu, M., et al., 2009. Fertility-preserving treatment in young women with well-differentiated endometrial carcinoma and severe atypical hyperplasia of endometrium. Fertility and Sterility, 92 (6), 2122–2124.