

Abstract
Background
Vulvar lichen sclerosus (LS) is a chronic inflammatory dermatosis which can progress to precursor lesion differentiated vulvar intraepithelial neoplasia (dVIN) and vulvar squamous cell carcinoma (VSCC). The risk of developing recurrent vulvar cancer following LS-associated VSCC is high. Evidence suggests that treatment of LS with topical corticosteroids (TCS) can prevent progression to dVIN, VSCC and recurrences. However, current guidelines do not give any recommendation on the management of LS following surgery for VSCC. The aim of this study was to conduct a survey among all registered gynaecologic oncologists (GOs) in the Netherlands to evaluate the current management of LS patients without a history of VSCC (LSnoVSCC) and patients with LS following surgery for VSCC (LSVSCC).
Methods
An online survey was distributed to all registered GOs in the Netherlands. Primary outcome measures were the frequency, type and duration of TCS treatment prescribed for LSnoVSCC and LSVSCC patients, separately. As a secondary outcome measure, reasons for treating or not treating patients with LSnoVSCC and LSVSCC with TCS were analysed.
Results
Forty-four GOs completed the survey, resulting in a response rate of 75%. TCS were prescribed more often to patients with LSnoVSCC as compared to patients with LSVSCC (86% versus 52%, respectively, p < 0.001). If treatment was initiated, ultra-potent (class IV) TCS were most commonly prescribed for an indefinite period of time for both patient groups. The most reported reason for treating patients in both groups with TCS was symptoms, followed by clinical aspects of the lesion and prevention of progression to dVIN and VSCC.
Conclusion
The majority of GOs who participated in our study endorse the utilisation of long-term ultra-potent TCS therapy in both patients with LSnoVSCC and LSVSCC. Nevertheless, Dutch GOs are currently prescribing TCS more frequently to patients with LSnoVSCC than to patients with LSVSCC.
PLAIN LANGUAGE SUMMARY
Vulvar lichen sclerosus (LS) is a chronic skin condition which may progress to vulvar squamous cell carcinoma (VSCC) through differentiated vulvar intraepithelial neoplasia (dVIN). LS symptoms are treated with topical corticosteroids (TCS), which can also prevent progression to dVIN and VSCC. However, current international guidelines do not give any recommendation on the treatment of LS following surgery for VSCC. To evaluate the current management of LS patients without a history of VSCC (LSnoVSCC) and patients with LS following surgery for VSCC (LSVSCC), a survey study was conducted among all gynaecologic oncologists (GOs) in The Netherlands. The findings of this study demonstrate that Dutch GOs prescribed TCS more often to patients with LSnoVSCC as compared to patients with LSVSCC. However, when deciding to prescribe TCS, the majority of Dutch GOs prescribed ultra-potent TCS for an indefinite period of time for both LSnoVSCC and LSVSCC patients.
Introduction
Vulvar squamous cell carcinoma (VSCC) accounts for 90% of all vulvar cancers and is recognised to be heterogeneous due to the two different pathways through which it may develop (Singh and Gilks Citation2020). VSCC can develop from human papillomavirus (HPV)-associated vulvar high-grade squamous intraepithelial lesions (vHSIL) or HPV-independent vulvar intraepithelial neoplasia (VIN) (WHO Citation2020). HPV-independent VIN, also known as differentiated type VIN (dVIN), mostly arises in the background of anogenital lichen sclerosus (LS) (Bigby et al. Citation2016, Swarts et al. Citation2018, Cohen et al. Citation2019). LS is the most common chronic inflammatory dermatosis of the vulva and occurs mostly in postmenopausal women, with a rising incidence over the last decades (Bleeker et al. Citation2016). Symptoms of LS may include pruritus, irritation and scarring of the skin, resulting in the loss of vulvar architecture (Fergus et al. Citation2020). This may severely impact patients’ quality of life and sexual functioning (Van de Nieuwenhof et al. Citation2010). The reported absolute risk of developing VSCC in women with anogenital LS varies widely between studies, ranging from 0.0% to 21.9% (Spekreijse et al. Citation2020, Leis et al. Citation2022, Vieira-Baptista et al. Citation2022). Moreover, LS is frequently found adjacent to VSCC in pathologic resection specimens. In fact, LS-associated VSCC accounts for around 70% of all vulvar cancers (van de Nieuwenhof et al. Citation2008).
Treatment of vulvar cancer primarily consists of surgical excision, followed by adjuvant radiation therapy or chemotherapy in cases of advanced-stage cancer (IKNL 2018). Local vulvar recurrences occur in up to 40% of patients at 10 years after primary treatment of early-stage VSCC (Te Grootenhuis et al. Citation2019). The risk of developing a recurrent VSCC is significantly higher in patients with LS-associated VSCC compared to HPV-induced VSCC, with a 10-year recurrence rate of 44% and 28%, respectively (Nooij et al. Citation2017, Te Grootenhuis et al. Citation2019). Residual vulvar LS has been identified as one of the primary factors leading to a higher risk of local vulvar recurrence in patients treated for VSCC (Regauer et al. Citation2011, Yap et al. Citation2016).
First-line treatment of vulvar LS focuses primarily on symptom relief and consists of long-term therapy with potent or ultra-potent topical corticosteroids (TCS) (Kirtschig et al. Citation2015, Lewis et al. Citation2018, ACOG Citation2020, NVDV Citation2021). Compliant therapy with ultra-potent TCS in patients with LS has shown to reduce the risk of developing VSCC to nearly 0% (Lee et al. Citation2015). As the risk of developing a recurrent VSCC is particularly high in the presence of LS, this suggests that TCS treatment of LS following VSCC surgery could also potentially reduce the risk of developing a recurrence. In fact, a recent study reported that patients with vulvar LS who adhered to TCS therapy had a VIN or VSCC recurrence rate of 27%, as compared to the previously reported 5-year recurrence rates of 44–47% (Regauer et al. Citation2011, Yap et al. Citation2016, Chin et al. Citation2020).
Although first-line treatment of LS consists of ultra-potent TCS, current guidelines do not give a specific recommendation for treatment of LS following excision of VSCC, other than oncological follow-up visits (RCOG Citation2014, Schnürch et al. Citation2016, Oonk et al. Citation2017, IKNL 2018, Lewis et al. Citation2018, Saito et al. Citation2018, Morrison et al. Citation2020). A study from 2018 in the United Kingdom (UK) reported that 71% of gynaecologic oncologists (GOs) in the UK indeed prescribe TCS to patients with LS following VSCC surgery (Pounds et al. Citation2018). However, it is unknown to what extent this hypothesis is being complied in current medical practice in the Netherlands. Therefore, the aim of this study was to conduct a survey amongst Dutch GOs to investigate the management of LS and LS following VSCC surgery by TCS in the Netherlands.
Materials and methods
Study population and survey distribution
All GOs registered at the Netherlands Association of Obstetrics and Gynaecology (NVOG) in May 2020 (n = 59) were selected for inclusion. E-mail addresses were provided by the NVOG. An online questionnaire was distributed to all selected GOs via Castor EDC, an electronic data capture tool for clinical research, which remained accessible for 8 weeks. Three reminders were sent to all non-responders with a one-to-two-week interval.
The survey contained 20 questions divided into three sections: (1) characteristics of the participating gynaecologists, (2) prescribing TCS in patients with LS without a history of VSCC (LSnoVSCC) and (3) prescribing TCS in patients with LS following VSCC surgery (LSVSCC). An English translation of the questionnaire is provided in Supplementary Methods 1. We referred to the classification system of TCS as used in Dutch medical practice, ranging from mild potency (class I) to ultra-potent (class IV) TCS (NVDV Citation2021).
Ethical approval was obtained prior to study initiation from the Institutional Review Board (IRB) at the Netherlands Cancer Institute in Amsterdam (registered under number IRBd20-052). All participating GOs provided informed consent online through Castor EDC before submitting the questionnaire.
Outcome measures
The primary outcome measures of this study were the frequency, potency and duration of TCS treatment prescribed for patients with LSnoVSCC and patients with LSVSCC. Subsequently, we specifically looked for the number of GOs who always prescribe ultra-potent (class IV) TCS for an indefinite period of time for both LSnoVSCC and LSVSCC patients separately. Results were stratified for the GOs’ area of interest and number of LSnoVSCC and LSVSCC patients they treated each year. As a secondary outcome measure, we analysed the reasons for treating patients with LSnoVSCC and LSVSCC with TCS.
Statistical analysis
Categorical variables were displayed as frequencies and transformed to binary data for further analysis. Comparisons of GO prescription behaviour between patients with LSnoVSCC and patients with LSVSCC were visualised by Sankey diagrams. Paired binary data were compared using the McNemar test. For other comparisons we used the Pearson Chi-Square test. P-values <0.05 were considered statistically significant. Analyses were performed in IBM SPSS 28 and diagrams were created using SankeyMATIC.
Results
Characteristics of study Participants
A total of 44 out of 59 GOs in the Netherlands completed the online survey, resulting in a response rate of 75%. All 17 Dutch hospitals employing a GO were represented by at least one participant completing the survey. The characteristics of participating GOs are shown in . Participating GOs were mostly female and had obtained a PhD degree. Years of experience as a specialised GO ranged from 0 to 38 years, with a median of 10.5 years. The majority of GOs were employed within an academic medical centre. Just over 50% reported to have specific interest in vulvar carcinoma. Roughly half of all GOs reported to treat more than 20 patients with LSnoVSCC or LSVSCC patients per year.
Table 1. Characteristics of gynaecologic oncologists completing survey (n = 44).
Frequency, potency and duration of steroid prescription
An overview of the frequency, potency and duration at which GOs reported to prescribe TCS to patients with LSnoVSCC and LSVSCC can be appreciated in and . A higher frequency of prescribing TCS was observed for patients with LSnoVSCC compared to LSVSCC patients, with 86% of GOs always or almost always prescribing TCS for LSnoVSCC patients versus 52% doing so for LSVSCC patients (p < 0.001, McNemar test). One GO reported to always prescribe TCS for patients with LSnoVSCC, but never for patients with LSVSCC ().
Figure 1. Prescription behaviour of gynaecologic oncologists (GOs) for patients with lichen sclerosus without a history of vulvar cancer (LSnoVSCC) versus patients with lichen sclerosus following surgery for vulvar cancer (LSVSCC); (A) Frequency of prescribing topical corticosteroids (TCS), (B) type of TCS prescribed and (C) duration of TCS treatment. Class IV, ultra-potent TCS; Class III, potent TCS; Class II, moderately potent TCS; Class I, mildly potent TCS.
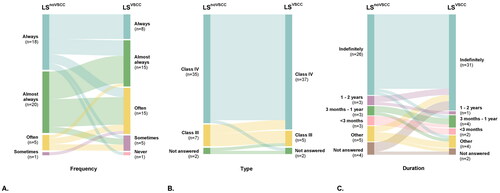
Table 2. Frequency, potency and duration of corticosteroid treatment prescribed by gynaecologic oncologists (GOs) in patients with lichen sclerosus (LS) without a history of vulvar cancer (LSnoVSCC) and patients with LS following surgery for vulvar cancer (LSVSCC).
With regards to potency of corticosteroids and duration of treatment, no differences were observed between treatment of LSnoVSCC and LSVSCC patients (p = 0.625 and p = 0.180, respectively, McNemar test, ). The preferred type of TCS in both patient groups were ultra-potent (class IV) TCS (). Mild and moderately potent TCS (Class I and II) were never prescribed to LSnoVSCC or LSVSCC patients by any of the GOs participating in this survey. Interestingly, whenever TCS were prescribed, most GOs did so for an indefinite period of time to both LSnoVSCC and LSVSCC patients (59% and 68%, respectively, p = 0.180, McNemar test, ).
When combining frequency, type and duration of TCS treatment, significantly more GOs always prescribed ultra-potent TCS for an indefinite period of time for their patients with LSnoVSCC compared to their patients with LSVSCC (14 versus 8, respectively, p = 0.031, McNemar test). The eight GOs who always prescribed ultra-potent TCS indefinitely to their patients with LSVSCC, also did this for their patients with LSnoVSCC.
With regards to LSnoVSCC patients, stratification for characteristics of the participating GOs did not result in any significant differences in prescription behaviour. For patients with LSVSCC, however, GOs employed in an academic medical centre prescribed TCS more often as compared to GOs employed in a non-academic centre (22/35 versus 1/9, respectively, p = 0.029, Pearson Chi-Square test). Stratification for other characteristics did not show any significant differences.
Reasons for treatment with topical corticosteroids
Symptoms were the most frequently reported reason for prescribing TCS in patients with LSnoVSCC (84%), followed by clinical aspects of the lesion (50%) (). A similar result is seen for LSVSCC patients, although overall less GOs reported that symptoms and clinical aspects of the lesion were the main indications for TCS treatment (68 and 43%, respectively). Prevention of (recurrent) dVIN or VSCC was reported more frequently by GOs as an important reason for TCS treatment in patients with LSVSCC (30%) than in patients with LSnoVSCC (16%).
Table 3. Reported reasons for treating patients with lichen sclerosus (LS) without a history of vulvar cancer (LSnoVSCC) and patients with LS following surgery for vulvar cancer (LSVSCC) with topical corticosteroids (TCS).
Three GOs provided reasons for not using TCS as a treatment modality for LSnoVSCC or LSVSCC. The single GO who had never prescribed TCS to LSVSCC patients reported that the reason was their lack of familiarity with it. Two GOs indicated that patient preferences influenced their decision not to prescribe TCS for LSnoVSCC, with one of them also citing it as a reason for not treating LSVSCC patients.
Discussion
In this survey study, we demonstrated a difference in TCS prescription behaviour of GOs for patients with LSnoVSCC versus patients with LSVSCC in the Netherlands. TCS are prescribed more often to patients with LSnoVSCC as compared to patients with LSVSCC, whereas the type and duration of prescribed TCS treatment is similar between these groups. All 17 Dutch hospitals employing GOs were represented by at least one participant completing the survey. Therefore, in combination with a response rate of 75%, our results give a sufficient representation of prescription behaviour by GOs in the Netherlands.
Worldwide guidelines recommend topical therapy with potent or ultra-potent TCS (class III-IV) as first-line treatment for LS, starting with daily application during the first month followed by reduced application for the following two months (Kirtschig et al. Citation2015, Lewis et al. Citation2018, ACOG Citation2020, NVDV Citation2021). Until recently, no specific recommendations were given on the duration of TCS treatment after induction therapy, however long-term use was commonly advocated by clinicians (Fergus et al. Citation2020). In the last two decades, several studies have indicated that continuous maintenance therapy with ultra-potent TCS is crucial to prevent pre-cancerous changes in patients with LS (Renaud-Vilmer et al. Citation2004, Virgili et al. Citation2013, Lee et al. Citation2015). As of more recently, novel evidence is emerging that compliant therapy with ultra-potent TCS is also associated with a significantly lower rate of progression to vulvar cancer in patients diagnosed with and treated for dVIN (Gallio et al. Citation2023). Despite concerns associated with chronic use of TCS, studies have demonstrated that prolonged use of medium to high-potency TCS is safe, effective and unlikely to cause skin changes, infections or systemic adverse effects (Wijaya et al. Citation2021, Mautz et al. Citation2022).
Interestingly, the Dutch guideline on management of LS was updated in 2021, shortly after we conducted this survey (NVDV Citation2021). Current recommendations in the Netherlands include maintenance treatment with TCS one to four times per week, in addition to daily use of emollients. This is reflected in our results, as the majority of GOs reported to prescribe ultra-potent TCS for an indefinite period of time to patients with LS. Guidelines on the management of LS have also been updated in other countries in recent years, advising continuous maintenance TCS treatment even when patients are asymptomatic (ACOG Citation2020, Yeon et al. Citation2021).
Contrary to recommendations provided for LSnoVSCC, current (inter)national guidelines do not give any recommendations for the treatment of patients with LSVSCC (RCOG Citation2014, Kirtschig et al. Citation2015, Oonk et al. Citation2017, IKNL 2018, Lewis et al. Citation2018, Saito et al. Citation2018, Morrison et al. Citation2020, NVDV Citation2021). This is also reflected in our results, as we observed that GOs prescribe TCS for patients with LSVSCC less frequently than for their patients with LS without cancer. Numerous other factors may contribute to the difference in TCS prescription behaviour between LSnoVSCC and LSVSCC patients. Patient-reported symptoms may have changed due to possible nerve damage caused by VSCC surgery. Also, post-operative scarring may lead to extensive disfigurement and alterations in vulvar anatomy. As a result, the characteristic efflorescence of LS may not be as prominent.
A limitation of our study is that we cannot comment on the effect of prior treatment on the decision for GOs to prescribe TCS in both LSnoVSCC and LSVSCC patients. Patients with LS are referred to a GO when there are signs of neoplasia. Thus, these patients likely already have a specific treatment regimen which the GO can choose to continue or alter following VSCC surgery.
In addition, views on maintenance therapy with corticosteroids may differ between different types of specialists. Dermatologists and non-oncological gynaecologists are mostly not involved in the oncological follow-up and management of LSVSCC patients in the Netherlands, whereas they are one of the primary treatment providers for patients with LS without vulvar cancer. Therefore, including these specialists in our survey may have given a different view on this subject. Furthermore, the organisation of care for LS patients may vary from country to country. Therefore, our findings are unique to the Netherlands and, as a result, have limited generalisability to other countries.
A similar survey study from 2018 showed that amongst 41 UK gynaecologists, 71% prescribed TCS to patients with LSVSCC and 27% never did so (Pounds et al. Citation2018). In this study, merely 2% never prescribed TCS to LSVSCC patients. Furthermore, the majority of UK gynaecologists chose potent (class III) TCS (52%), whereas Dutch GOs primarily chose ultra-potent (class IV) TCS (84%). The variance in our results compared to the findings in the UK is likely a reflection of the differences in expert clinical opinion at time of the surveys between these two countries.
In conclusion, Dutch GOs are currently prescribing ultra-potent TCS more often to their patients with LSnoVSCC as compared to patients with LSVSCC. Nevertheless, clinical practice and expert clinical opinions concerning the management of patients with LS, especially following VSCC, are evolving the last decade as reflected by our findings. Further prospective studies are needed to integrate the use of TCS in patients with LSVSCC in both (inter)national LS and vulvar cancer guidelines.
Author contributions
Féline O. Voss: Data curation, Formal analysis, Investigation, Methodology, Visualisation, Writing – original draft. Karelina L. Groenewegen: Data curation, Formal analysis, Investigation, Writing – review and editing. Hester Vermaat: Writing – review and editing. Maaike C.G. Bleeker: Supervision, Writing – review and editing. Marc van Beurden: Conceptualisation, Methodology, Project administration, Supervision, Writing – review and editing.
Supplemental Material
Download MS Word (15 KB)Acknowledgements
We thank all participating gynaecologic oncologists for their contributions in this study. We also thank the Dutch organization for Obstetrics and Gynaecology (NVOG) for providing contact details of all registered gynaecologic oncologists.
Disclosure statement
The authors have no conflicts of interest to disclose.
Data availability statement
The data that support the findings of this study are available upon reasonable request.
Additional information
Funding
References
- ACOG, American College of Obstetricians and Gynecologists. 2020. Diagnosis and management of vulvar skin disorders: ACOG Practice Bulletin, Number 224. Obstetrics & Gynecology, 136, e1–e14.
- Bigby, S.M., et al., 2016. The natural history of vulvar intraepithelial neoplasia, differentiated type: evidence for progression and diagnostic challenges. International Journal of Gynecological Pathology, 35 (6), 574–584.
- Bleeker, M.C., et al., 2016. Lichen Sclerosus: incidence and risk of Vulvar Squamous cell carcinoma. Cancer Epidemiology, Biomarkers & Prevention, 25 (8), 1224–1230.
- Chin, S., et al., 2020. Association of topical corticosteroids with reduced vulvar squamous cell carcinoma recurrence in patients with vulvar Lichen Sclerosus. JAMA Dermatology, 156 (7), 813–814.
- Cohen, P.A., et al., 2019. Clinical and molecular classification of vulvar squamous pre-cancers. International Journal of Gynecological Cancer, 29 (4), 821–828.
- Fergus, K.B., et al., 2020. Pathophysiology, clinical manifestations, and treatment of Lichen Sclerosus: a systematic review. Urology, 135, 11–19.
- Gallio, N., et al., 2023. Differentiated Vulvar Intraepithelial Neoplasia: three decades’ experience of a referral center. 14th Congress of European College for the Study of Vulval Disease (ECSVD), Helsinki, Finland.
- IKNL, Integraal Kankercentrum Nederland. 2018. Werkgroep oncologische gynaecologie. Utrecht, The Netherlands: Landelijke richtlijn Vulvacarcinoom.
- Kirtschig, G., et al., 2015. Evidence-based (S3) guideline on (anogenital) Lichen sclerosus. Journal of the European Academy of Dermatology and Venereology, 29 (10), e1-43–43.
- Lee, A., Bradford, J. and Fischer, G., 2015. Long-term management of adult vulvar lichen sclerosus: a prospective cohort study of 507 women. JAMA Dermatology, 151 (10), 1061–1067.
- Leis, M., et al., 2022. Risk of vulvar squamous cell carcinoma in Lichen Sclerosus and Lichen Planus: a systematic review. Journal of Obstetrics and Gynaecology Canada, 44 (2), 182–192.
- Lewis, F.M., et al., 2018. British association of dermatologists guidelines for the management of lichen sclerosus, 2018. The British Journal of Dermatology, 178 (4), 839–853.
- Mautz, T.T., Krapf, J.M. and Goldstein, A.T., 2022. Topical corticosteroids in the treatment of vulvar Lichen Sclerosus: a review of pharmacokinetics and recommended dosing frequencies. Sexual Medicine Reviews, 10 (1), 42–52.
- Morrison, J., et al., 2020. British Gynaecological Cancer Society (BGCS) vulval cancer guidelines: recommendations for practice. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 252, 502–525.
- Nooij, L.S., et al., 2017. Genomic characterization of vulvar (Pre)cancers identifies distinct molecular subtypes with prognostic significance. Clinical Cancer Research, 23 (22), 6781–6789.
- NVDV, Nederlandse Vereniging voor Dermatologie en Venereologie. 2021. Richtlijn Lichen sclerosus. Utrecht, The Netherlands: Richtlijnendatabase.
- Oonk, M.H.M., et al., 2017. European society of gynaecological oncology guidelines for the management of patients with vulvar cancer. International Journal of Gynecological Cancer, 27 (4), 832–837.
- Pounds, R., et al., 2018. A survey on the use of topical steroids in patients treated for lichen sclerosus-associated vulval squamous cell carcinoma. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 38 (2), 265–269.
- RCOG, Royal College of Obstetricians and Gynaecologists. 2014. Guidelines for the diagnosis and management of vulval carcinoma. England: Royal College of Obstetricians and Gynaecologists
- Regauer, S., Eberz, B. and Reich, O., 2011. Residual anogenital lichen sclerosus after cancer surgery has a high risk for recurrence: a clinicopathological study of 75 women. Gynecologic Oncology, 123 (2), 289–294.
- Renaud-Vilmer, C., et al., 2004. Vulvar lichen sclerosus: effect of long-term topical application of a potent steroid on the course of the disease. Archives of Dermatology, 140 (6), 709–712.
- Saito, T., et al., 2018. Japan society of gynecologic oncology guidelines 2015 for the treatment of vulvar cancer and vaginal cancer. International Journal of Clinical Oncology, 23 (2), 201–234.
- Schnürch, H. G., et al., 2016. Diagnosis, therapy and follow-up care of vulvar cancer and its precursors. Guideline of the DGGG and DKG (S2k-level, AWMF registry number 015/059, November 2015. Geburtshilfe Und Frauenheilkunde, 76 (10), 1035–1049.,
- Singh, N. and Gilks, C.B., 2020. Vulval squamous cell carcinoma and its precursors. Histopathology, 76 (1), 128–138.
- Spekreijse, J.J., et al., 2020. The risk of developing squamous cell carcinoma in patients with anogenital lichen sclerosis: a systematic review. Gynecologic Oncology, 157 (3), 671–677.
- Swarts, D.R.A., et al., 2018. Molecular heterogeneity in human papillomavirus-dependent and -independent vulvar carcinogenesis. Cancer Medicine, 7 (9), 4542–4553.
- Te Grootenhuis, N.C., et al., 2019. Margin status revisited in vulvar squamous cell carcinoma. Gynecologic Oncology, 154 (2), 266–275.
- Van De Nieuwenhof, H.P., et al., 2010. The effect of vulvar lichen sclerosus on quality of life and sexual functioning. Journal of Psychosomatic Obstetrics and Gynaecology, 31 (4), 279–284.
- Van De Nieuwenhof, H.P., Van Der Avoort, I.A. and De Hullu, J.A., 2008. Review of squamous premalignant vulvar lesions. Critical Reviews in Oncology/Hematology, 68 (2), 131–156.
- Vieira-Baptista, P., et al., 2022. Risk of development of vulvar cancer in women with Lichen Sclerosus or Lichen Planus: a systematic review. Journal of Lower Genital Tract Disease, 26 (3), 250–257.
- Virgili, A., et al., 2013. Proactive maintenance therapy with a topical corticosteroid for vulvar lichen sclerosus: preliminary results of a randomized study. The British Journal of Dermatology, 168 (6), 1316–1324.
- WHO, World Health Organization. 2020., World health organization classification of tumours, female genital tumours. 5th ed. Lyon, France: IARC Press.
- Wijaya, M., et al., 2021. Quality of life in vulvar Lichen Sclerosus patients treated with long-term topical corticosteroids. Journal of Lower Genital Tract Disease, 25 (2), 158–165.
- Yap, J.K., et al., 2016. Adjacent Lichen Sclerosis predicts local recurrence and second field tumour in women with vulvar squamous cell carcinoma. Gynecologic Oncology, 142 (3), 420–426.
- Yeon, J., et al., 2021. Vulval lichen sclerosus: an Australasian management consensus. The Australasian Journal of Dermatology, 62 (3), 292–299.