

Introduction
Pial arteriovenous fistulas (PAVFs) are another type of relatively rare abnormality, and these fistulas are also known as nongalenic arteriovenous fistulas (NG-AVFs) (Jaimes et al. Citation2022). A case of foetal PAVF was diagnosed by prenatal ultrasound (US) and foetal MRI at our institution, and the diagnosis was confirmed after labour induction. Combined with a review of previous literature, we present the following case (informed consent was obtained from the patient).
Case report
A 28-year-old pregnant woman had no family history of genetic disorders and no abnormalities in genetic testing. Physical examination showed no abnormalities. Antenatal US was performed at 26 weeks of gestation at our hospital. A vascular malformation or arteriovenous fistula was suspected ().
Figure 1. (A, B) Disorganised foetal intracranial structures with abnormal blood flow. Dilated superior vena cava, bilateral cephalic brachial veins and left innominate vein. (C–E, triangle) Multiple patches of high-intensity signals on T1-weighted imaging and low-intensity signals on T2-weighted imaging were distributed around the bilateral lateral ventricles just beneath the ependyma and mainly involved the left germinal matrix. (D, E, arrows) A tortuous and dilated vessel was exposed on the convex surface of the left cerebral hemisphere, and it converged into the superior sagittal sinus along with the surrounding dilated vessels. (F, triangle) The left cerebral hemisphere showed a diffuse high-intensity signal. (G, H, arrows) The bilateral transverse sinuses and sigmoid sinuses were also dilated. (I, arrows) A PAVF in a large vein on the surface of the left hemisphere. (J, arrows) Multiple haemorrhagic foci were found in the germinal matrix. In addition to diffuse encephalomalacia, atrophy of the left cerebral hemisphere and cortical dysplasia were present.
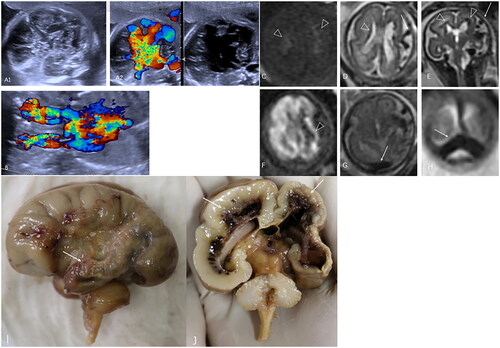
The pregnant woman underwent further examination by foetal MRI, and the results were as follows: (1) a tortuous and dilated vessel was exposed on the convex surface of the left cerebral hemisphere, was connected with the dilated middle cerebral artery, and converged into the superior sagittal sinus along with the surrounding dilated vessels. The bilateral transverse sinuses and sigmoid sinuses were also dilated. (2) The bilateral cerebral hemispheres of the foetus were asymmetric, the left cerebral hemisphere was atrophied. (3) A diffuse increased T2 signal was observed in the bilateral cerebral hemispheres; multiple patches of high-intensity signals on T1-weighted imaging were distributed around the bilateral lateral ventricles just beneath the ependyma. (4) The left cerebral hemisphere showed a diffuse high-intensity signal on diffusion-weighted imaging (DWI). A diagnosis of partial arteriovenous fistula (PAVF) was confirmed by MRI, and abnormal cortical development and intracranial haemorrhage were subsequently confirmed in the autopsy ().
Due to economic constraints, no prenatal examination was conducted before 26 weeks of gestation. Based on the findings on US and MRI imaging, the physician was fully informed about the condition of the foetus and the possibility of a poorer prognosis. Because of concerns about the prognosis of the foetus, labour was induced at our hospital at 27 weeks of gestation, and an autopsy of the foetus was performed with the patient’s consent. A PAVF in a large vein on the surface of the left hemisphere was confirmed by examination of the gross specimen, and multiple haemorrhagic foci were found in the germinal matrix. In addition to diffuse encephalomalacia, atrophy of the left cerebral hemisphere and focal cortical dysplasia were also present ().
Discussion
In a foetus, an intracranial AVF can occur in either the pia mater or dura mater and is often associated with haemorrhage, ischaemia and abnormal brain development. PAVFs account for 1.6–4.7% of all intracranial vascular malformations (Kelly and Rijhsinghani Citation2005). The aetiology of PAVFs is currently not fully understood; abnormal angiogenesis and related vascular growth factors and cytokines may also play roles in PAVF formation (Madsen et al. Citation2013, Yu et al. Citation2016). When severe foetal oedema and multiple organ failure occur in a child, it is recommended to terminate the pregnancy. In the present case, multiple haemorrhagic foci were observed in the cerebral parenchyma, mainly in the germinal matrix. Because the vessel wall of the germinal matrix microvasculature of foetuses is immature, fluctuations in cerebral blood flow and the lack of autoregulation seem to be important factors contributing to subventricular haemorrhage (Kutuk et al. Citation2013, Parodi et al. Citation2020). Arteriovenous fistulas have insufficient perfusion, cerebral tissue oedema, ischaemia, cerebral atrophy and cortical dysplasia. In our case, the PAVF was located in the left hemisphere, but haemorrhage and oedema were also observed in the contralateral hemisphere. We speculate that the increased pressure in the superior sagittal sinus may have affected the contralateral venous drainage. Observation of the gross specimen showed atrophy and thinning of the brain parenchyma and multiple anomalies of the cerebellar gyrus and grey matter, suggesting the additional presence of a more complex malformation of cortical development (MCD) (Crino Citation2015).
In the foetal period, PAVFs need to be differentiated from vein of Galen aneurysmal malformations (VGAMs) (Zhou et al. Citation2016). The origin of the malformation and the draining vessels may be the key to differential diagnosis.
At present, there have been few reports on the diagnosis of PAVFs by prenatal MRI, and there have been no corresponding reports on prenatal gross specimens or MRI findings (Pedicelli et al.Citation2017). Foetal MRI provides more powerful evidence than US, especially single-shot fast spin echo (SSFSE) sequences, which provide better visualisation of supplying arteries and draining veins and thus allow PAVFs to be easily distinguished from the high signal intensity in the surrounding parenchyma and cerebrospinal fluid.
Foetal MRI can provide high-resolution images for the diagnosis of PAVFs and assessment of secondary brain injuries, thus providing more powerful evidence for determining a clinical diagnosis and prognosis. However, the patient in this case had no other treatment options, and there are limitations for subsequent prognostic assessment.
Ethical approval
Ethics committee approval was unnecessary due to the nature of the study.
Author contributions
Conceptualisation: LiXia Zhou
. Formal analysis: Yimin Cao
. Funding acquisition: none
. Investigation: Weixin Meng
. Methodology: retrospective study
. Project administration: LiXia Zhou
. Resources: The Second Hospital of Hebei Medical University
. Software: JianXiong Zheng
. Supervision: Duo Gao and Chengye Zhang
. Validation: Weixin Meng
. Visualisation: LiXia Zhou
. Writing-original draft: Yimin Cao and LiXia Zhou
. Writing – review and editing: LiXia Zhou.
Consent form
Written informed consent was obtained from the patient.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Additional information
Funding
References
- Crino, P., 2015. Focal cortical dysplasia. Seminars in Neurology, 35 (3), 201–208.
- Jaimes, C., et al., 2022. Brain injury in fetuses with vein of Galen malformation and nongalenic arteriovenous fistulas: static snapshot or a portent of more? AJNR American Journal of Neuroradiology, 43 (7), 1036–1041.
- Kelly, A. and Rijhsinghani, A., 2005. Antenatal course of a fetal intracranial arteriovenous fistula: a case report. The Journal of Reproductive Medicine, 50 (5), 367–369.
- Kutuk, M.S., et al., 2013. Prenatal diagnosis and postnatal outcome of fetal intracranial hemorrhage. Child’s Nervous System, 30 (3), 411–418.
- Madsen, P.J., et al., 2013. An institutional series and literature review of pial arteriovenous fistulas in the pediatric population. Journal of Neurosurgery. Pediatrics, 12 (4), 344–350.
- Parodi, A., et al., 2020. Cranial ultrasound findings in preterm germinal matrix haemorrhage, sequelae and outcome. Pediatric Research, 87 (Suppl. 1), 13–24.
- Pedicelli, A., et al., 2017. Prenatal diagnosis and multimodal neonatal treatment of a rare pial arteriovenous fistula: case report and review of the literature. World Neurosurgery, 104, 1050.e13–1050.e18.
- Yu, J., et al., 2016. Intracranial non-galenic pial arteriovenous fistula: a review of the literature. Interventional Neuroradiology, 22 (5), 557–568.
- Zhou, L.-X., Dong, S.-Z., and Zhang, M.-F., 2016. Diagnosis of vein of Galen aneurysmal malformation using fetal MRI. Journal of Magnetic Resonance Imaging, 46 (5), 1535–1539.