

Abstract
Background
As women with low ovarian reserve embark on the challenging journey of in-vitro fertilisation (IVF) treatment, the choice between natural and mildly stimulated cycles becomes a pivotal consideration. It is unclear which of these two regimens is superior for women with low ovarian reserve. Our study aims to assess the impact of natural cycles on embryo quality and pregnancy outcomes in women with low ovarian reserve undergoing IVF treatment compared to mildly stimulated cycles.
Methods
This retrospective study enrolled consecutive patients with low ovarian reserve who underwent IVF/intracytoplasmic sperm injection (ICSI) at Guangdong Second Provincial General Hospital between January 2017 and April 2021. The primary outcome for pregnancy rate of 478 natural cycles and 448 mild stimulated cycles was compared. Secondary outcomes included embryo quality and oocyte retrieval time of natural cycles.
Results
The pregnancy rate in the natural cycle group was significantly higher than that in the mildly stimulated cycle group (51.8% vs. 40.1%, p = 0.046). Moreover, natural cycles exhibited higher rates of available embryos (84.1% vs. 78.6%, p = 0.040), high-quality embryos (61.8% vs. 53.2%, p = 0.008), and utilisation of oocytes (73% vs. 65%, p = 0.001) compared to mildly stimulated cycles. Oocyte retrievals in natural cycles were predominantly performed between 7:00 and 19:00, with 94.9% occurring during this time frame. In natural cycles with high-quality embryos, 96.4% of oocyte retrievals were also conducted between 7:00 and 19:00.
Conclusion
Natural cycles with appropriately timed oocyte retrieval may present a valuable option for patients with low ovarian reserve.
PLAIN LANGUAGE SUMMARY
In the realm of in-vitro fertilisation (IVF) treatment, women with low ovarian reserve often face the crucial decision of opting for natural or mildly stimulated cycles. This retrospective study, conducted between January 2017 and April 2021 at Guangdong Second Provincial General Hospital, delves into the impact of these cycles on pregnancy outcomes. Examining 478 natural cycles and 448 mildly stimulated cycles, the study reveals a notably higher pregnancy rate in the natural cycle group (51.8% vs. 40.1%). Additionally, natural cycles demonstrated higher rates of available embryos, high-quality embryos, and oocyte utilisation compared to their mildly stimulated counterparts. The findings suggest that natural cycles, with proper oocyte retrieval timing, could be a favourable choice for those with low ovarian reserve seeking IVF treatment.
Introduction
Assisted reproduction technology (ART) is the primary approach for managing infertility and achieving pregnancy (Kamel Citation2010; Fields et al. Citation2013; Lindsay & Vitrikas Citation2015; Practice Committee of the American Society for Reproductive, Medicine Citation2015). While age is commonly recognised as the primary factor influencing ART effectiveness, pregnancy outcomes can also be affected by the cause of infertility and the specific ART regimens used (Kamel Citation2010; Joshi et al. Citation2012; Fields et al. Citation2013; Lindsay & Vitrikas Citation2015; Practice Committee of the American Society for Reproductive Medicine). The selection of an effective controlled ovarian hyperstimulation protocol to improve ovarian response and embryo quality, reduce cycle cancellation rates, and enhance pregnancy rates in patients with low ovarian reserve remains a significant challenge, with no established optimal regimen identified (Jirge Citation2016; Rasool & Shah Citation2017; Conforti et al. Citation2019).
Routine ovarian stimulation for in vitro fertilisation (IVF)/intracytoplasmic sperm injection (ICSI) in individuals with low ovarian reserve is associated with a high cancellation rate due to poor response, absence of oocytes, fertilisation failure, and suboptimal embryo quality. This places a financial burden and causes mental pressure for patients with low ovarian reserve (Schimberni et al. Citation2009). In recent years, there has been growing interest in natural cycle IVF/ICSI (NC-IVF/ICSI) due to its advantages, such as high-quality embryos, minimal risk of multiple pregnancies, absence of ovarian hyperstimulation syndrome, and patient-friendly nature (Pelinck et al. Citation2002; von Wolff Citation2019; De Marco et al. Citation2021). Moreover, NC-IVF/ICSI is more cost-effective and can be repeated on a monthly basis, although the outcomes between stimulated and unstimulated cycles vary across studies (Lindheim et al. Citation1997; Ng et al. Citation2001; von Wolff Citation2019; De Marco et al. Citation2021). Nevertheless, the lack of large-scale trials prevents definitive conclusions from being drawn. This study aims to compare natural cycles and mildly stimulated cycles in women with infertility due to low ovarian reserve, specifically focusing on oocyte and embryo quality, pregnancy outcomes, and the timing of oocyte retrieval in natural cycles. The findings from this study may contribute to defining the role of NC-IVF/ICSI in managing infertility caused by low ovarian reserve.
Methods
Study design and patients
This retrospective cohort study enrolled consecutive patients with low ovarian reserve function (antral follicular count [AFC] ≤ 5–7 or anti-Müllerian hormone [AMH] ≤ 1.1 ng/ml) who underwent IVF/ICSI at the Centre for Reproductive Medicine of Guangdong Second Provincial Hospital between January 2017 and April 2021. Additionally, patients with acute infectious diseases, somatic organic disorders, chromosomal abnormalities, psychosis, or tumours were excluded (). 926 cycles of patients full-filling the inclusion and exclusion criteria were all enrolled in this study. The study received approval from the Ethics Committee of Guangdong Second Provincial Hospital, and patient informed consent was exempted.
Figure 1. Flowchart describing the selection criteria of our study cohort.
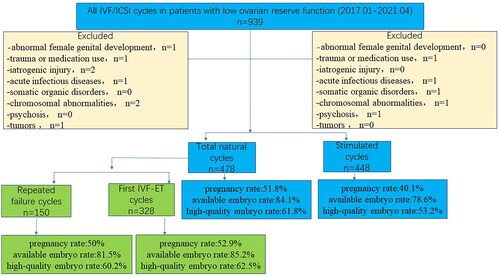
The patients with repeated failed cycles were defined as those who experienced oocyte retrieval failure, fertilisation failures, or lacked embryos available for transfer after undergoing more than two stimulation cycles at other hospitals.
Mildly stimulated cycles and natural cycles
The choice of fertilisation method (IVF or ICSI) depended on the patients’ reproductive history, infertility cause, and sperm parameters. The choice of either mildly stimulated cycles and natural cycles was according to physician preference. For the mild stimulation protocol, letrozole at a dose of 2.5 mg/day was administered from cycle day 2 to 6, and gonadotrophin (r-FSH) at a dose of 75–150 IU with 0.08–0.25 mg/day of GnRH-A was administered when serum luteinizing hormone (LH) levels exceeded the baseline level and continued until the day of hCG administration. If serum LH levels were above the baseline prior to hCG administration, an additional dose of 0.08–0.25 mg/day of GnRH-A was added; otherwise, no GnRH-A was administered. Oocyte retrieval was performed 36 hours after hCG injection when follicles reached a diameter of 16–20 mm. In the natural protocol, monitoring of follicle development and serum levels of oestradiol, progesterone, and LH was conducted upon appearance of the leading follicle and again after two or three days. Daily monitoring of follicle growth occurred once the leading follicle reached a diameter of ≥16 mm. Serum levels of E2, P, and LH were measured daily between 08:00 and 09:00 until a decrease in E2 levels was observed while LH levels continued to increase. Blood samples were then collected twice or thrice daily to detect the onset of the LH surge until LH levels began to decrease. Oocyte retrieval took place 6-10 hours after the LH surge. No additional drugs, such as gonadotrophin or GnRH-a, were administered during the natural protocol.
All embryos from mildly stimulated cycles and natural cycles were cryopreserved on day 3. The embryos of FET cycles in natural cycle group were all from natural cycles, so as the mildly stimulated cycle group. Artificial (HRT) cycles were employed for endometrial preparation in Freezing Embryo Transfer (FET) cycles. Oestradiol (E2) supplementation commenced at a dose of 6 mg/day from cycle day 2 to day 5, increased to 8 mg/day from day 6 to day 9, and further increased to 10 mg/day from day 10 to day 13. Once the endometrial thickness (EMT) reached a minimum of 7 mm, vaginal progesterone (P4) administration of 200 mg three daily was initiated. Day 3 embryo transfer took place 72 hours after the start of progesterone. Blood human chorionic gonadotropin (hCG) levels were measured 14 days after embryo transfer in FET cycles to confirm pregnancy establishment, and transvaginal sonography was conducted 30 days after embryo transfer. Pregnant patients received continued luteal support until 10 weeks after embryo transfer, with regular follow-up appointments.
Outcomes and definitions
The primary outcome assessed in this study was the pregnancy rate. Secondary outcomes included the rates of available embryos and high-quality embryos, the rate of ovulation prior to aspiration, the rate of cycles with oocytes, the mean number of oocytes, the metaphase II oocytes rate, the utilisation rate of oocytes, the fertilisation rate, the normal fertilisation rate, the normal cleavage rate, the number of embryo cells, the blastomere symmetry score, the fragmentation score, the early abortion rate, the biochemical pregnancy rate and oocyte retrievals time of natural cycles.
Embryo scores were determined based on blastomere symmetry and fragmentation. The scoring system for blastomere symmetry was as follows: 1 point for equally sized symmetrical blastomeres, 2 points for unevenly sized blastomeres, and 3 points for highly unevenly sized blastomeres. The scoring system for fragmentation was as follows: 1 point for fragmentation ≤10%, 2 points for fragmentation between 11% and 20%, 3 points for fragmentation between 20% and 50%, and 4 points for fragmentation >50%. Good quality embryos were defined as follows: 1) >7-cell embryos with a blastomere symmetry score of 1–2 and fragmentation ≤10%, or 2) >7-cell embryos with a blastomere symmetry score of 1 and fragmentation between 11% and 20%. The criteria for available embryos were >4-cell embryos with a blastomere symmetry score of 1–2 and fragmentation ≤20%.
Data collection
The patients’ demographic characteristics (age, BMI, and duration of infertility), laboratory test results (AMH, AFC, and basal hormone levels), ovarian stimulation protocols and related data, oocyte quality, embryo outcomes, and pregnancy outcomes were collected through the medical record system.
Statistical analysis
All data were analysed using SPSS 22.0 (IBM, Armonk, NY, USA). The continuous variables were confirmed with normal distribution using the Kolmogorov-Smirnov test, presented as means ± standard deviation, and analysed between groups using Student’s t-test. Categorical data were presented as n (%) and analysed using the Chi-square test. Two-sided P values <0.05 were considered statistically significant.
Results
Pregnancy outcomes and embryo quality in natural vs. mildly stimulated cycles
The natural cycle group exhibited no gonadotrophin while the stimulated cycle group exhibited high average total gonadotrophin dose and long duration of stimulation (0 vs. 1693.64 ± 897.74 IU, p < 0.001; 0 vs. 8.78 ± 3.52 days, p < 0.001) ().
Table 1. Characteristics of total natural cycles and stimulated cycles.
Among the 478 natural cycles, 28 cycles (5.8%) experienced ovulation before aspiration, and 31 cycles (6.5%) had no oocytes aspirated. In contrast, no cycles in the 448 stimulated cycles (0%) experienced ovulation before aspiration, and 8 cycles (1.8%) had no oocytes aspirated. Oocyte retrieval was performed in 419 natural cycles (88%) and 440 stimulated cycles (98%), resulting in the retrieval of 472 and 872 oocytes, respectively. Although the mean number of retrieved oocytes was lower in natural cycles compared to stimulated cycles (1.1 ± 0.5 vs. 1.9 ± 0.8, p < 0.01), the metaphase II rate was higher (92.6% vs. 87.5%, p < 0.01). Furthermore, the natural cycle group exhibited significantly higher rates of available embryos (84.1% vs. 78.6%, p = 0.04), high-quality embryos (61.8% vs. 53.2%, p = 0.008), and utilisation of oocytes (73.3% vs. 64.6%, p = 0.001) compared to the stimulated cycle group (). Additionally, the natural cycle group had a lower score of symmetrical blastomeres compared to the stimulated cycle group (1.5 ± 0.6 vs. 1.7 ± 0.7, p < 0.01). There were 110 FET cycles in which embryos were all from natural cycles. The clinical pregnancy rate was significantly higher in the natural cycle group compared to the stimulated cycle group (51.8% vs. 40.1%, P = 0.046) ().
Table 2. Laboratory and pregnancy outcomes of natural and stimulated cycles.
Pregnancy outcomes and embryo quality of natural cycles in patients with repeated failure cycles vs. the first cycle
In our study, a total of 478 NC-IVF/ICSI cycles were analysed, with a specific focus on comparing the outcomes of patients with repeated failure cycles to those of the control group. Patients with repeated failure cycles had lower rates of cleavage (96% vs. 99%, p = 0.045) and oocyte utilisation (64.6% vs. 77.2%, p = 0.004) compared to the control group (Supplementary Table S1). However, there were no significant differences between the two groups in terms of the mean number of retrieved oocytes, metaphase II rate, overall fertilisation rate, normal fertilisation rate, rate of available embryos, embryo cleavage stage, blastomere symmetry score, fragmentation score, clinical pregnancy rate, early abortion rate, and biochemical pregnancy rate (Supplementary Table S2).
Oocyte retrieval time
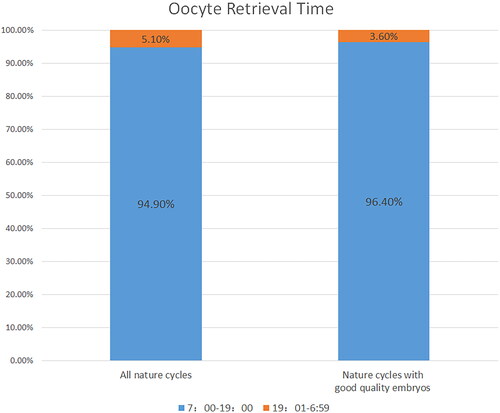
To evaluate the timing of oocyte retrieval in natural cycles, we collected clinical data from 415 natural cycles (excluding 31 cycles with no retrieved oocytes, 28 cycles with ovulation prior to aspiration, 2 cycles without fertilisation, and 2 cycles with oocyte degeneration). The distributions of the precise oocyte retrieval time and the time interval between oocyte retrieval and fertilisation were analysed using scatterplots and columns. As shown in , 94.9% of oocyte retrievals (394 cycles) were conducted between 7:00 am and 7:00 pm, while only 5.1% of oocyte retrievals occurred during nonworking hours.
On the other hand, to confirm whether more high-quality embryos were obtained by retrieving oocytes during all natural cycles, we collected accurate data from 223 natural cycles with high-quality embryos, including information on oocyte retrieval time and the time interval between oocyte retrieval and fertilisation. The scatterplot in demonstrated that, similar to all natural cycles, 96.4% of oocyte retrievals (215 cycles) took place between 7:00 am and 7:00 pm in the total natural cycles with high-quality embryos. Only 3.6% of oocyte retrievals occurred during nonworking hours. Therefore, it was observed that more good-quality embryos were obtained when oocytes were retrieved during natural cycles between 7:00 am and 7:00 pm.
Figure 2. Oocyte Retrieval Time in Total Natural Cycles. The frequencies of oocyte retrieval time are shown for all natural cycles and natural cycles with good quality embryos. The columns represent the number of oocyte retrieval times.
Discussion
The present study demonstrated significantly higher rates of available embryos, high-quality embryos, utilisation of oocytes, and pregnancy in the natural cycle group compared to the mildly stimulated cycle group, suggesting that natural cycles with appropriate oocyte retrieval time may be an ideal option for patients with low ovarian reserve.
Improving embryo quality and pregnancy rates in patients with low ovarian reserve poses a challenge in reproductive medicine (Mahutte and Arici Citation2007; Jirge Citation2016; Rasool and Shah Citation2017). Some studies have indicated that natural cycles are at least as effective as stimulated cycles for patients with repeated failure in stimulated cycles (Schimberni et al. Citation2009), while others suggest that the natural protocol is not effective for patients with high FSH levels and low numbers of retrieved oocytes in previous IVF/ICSI cycles (Kolibianakis et al. Citation2004). Furthermore, several studies have reported that high-dose gonadotropin stimulation fails to improve the pregnancy rate in patients with ovarian hyporesponsiveness and may even increase the rate of oocyte chromosome abnormalities (Di Guardo et al. Citation2022). Therefore, natural cycle IVF/ICSI treatment may be more effective for patients with low ovarian reserve.
In this retrospective study, the natural protocol and a mildly stimulated protocol were compared in women with low ovarian reserve. The two groups were similar in terms of age, ovarian reserve markers, and BMI. The intake of gonadotrophins and the duration of stimulation were significantly lower in the natural protocol group. Consequently, the mean number of retrieved oocytes was lower in natural cycles compared to stimulated cycles. However, the rates of metaphase II oocytes, available embryos, high-quality embryos, and utilisation of oocytes were higher in natural cycles than in stimulated cycles. Additionally, the symmetrical blastomere scores were better in natural cycles, indicating more equally sized embryos. Importantly, the clinical pregnancy rate was higher in natural cycles compared to stimulated cycles. Previous retrospective studies (Elizur et al. Citation2005; Ata et al. Citation2008; Polyzos et al. Citation2012; Kedem et al. Citation2014; Lainas et al. Citation2015; Drakopoulos et al. Citation2019) and clinical trials (Morgia et al. Citation2004; Kim et al. Citation2009) have compared natural cycles with stimulated cycles, but there were significant variations in stimulation regimens and patient populations among these studies (Di Guardo et al. Citation2022), making direct comparisons with the present study challenging. Nonetheless, most of these studies either reported negative results (i.e. no differences in pregnancy outcomes) or differences between natural cycles and high-dose gonadotropin cycles (Drakopoulos et al. Citation2019).
During IVF/ICSI, embryos often exhibit significant heterogeneity in terms of morphology and chromosomal constitution. Ziebe et al. demonstrated that the stimulation protocol did not influence the morphology of early-stage embryos (Ziebe et al. Citation2004). Conversely, Kaneko et al. found that the rate of mature oocytes was higher in stimulated cycles compared to natural protocols (Kaneko et al. Citation2000). However, a previous study has shown that repeated ovarian stimulation can lead to increased spindle defects and chromosomal errors in mice (Van Blerkom and Davis Citation2001). DiMattina et al. reported that the fertilisation rate of oocytes derived from secondary follicles was lower than that of oocytes derived from dominant follicles (DiMattina et al. Citation2014). Nevertheless, the addition of gonadotrophins in stimulated cycles did not provide optimal conditions for selecting dominant follicles. This may explain the higher number of utilised and good-quality embryos observed in natural cycles.
Ovulation prior to oocyte retrieval can occur in natural cycles (øHøjgaard et al. Citation2001; Ingerslev et al. Citation2001). The literature reports oocyte retrieval rates ranging from 28.6% to 86.1% in natural cycles (Phillips et al. Citation2007). The timing of oocyte retrieval in natural cycles depends on the occurrence of an appropriate spontaneous LH surge. In patients with advanced age or poor ovarian reserve, the descending branch of LH is shorter, resulting in a weakened positive feedback of sex steroids on LH secretion. Due to the higher ovulation rate before oocyte retrieval, only a few centres have widely adopted the natural protocol. However, the ovulation rate prior to oocyte retrieval in the present study was lower than that reported in the literature. Our centre has extensive experience in assisted reproductive technology, suggesting that natural cycles with an optimal oocyte retrieval time are equally effective as mildly stimulated cycles in women with low ovarian reserve.
In the present study, patients with repeated failure cycles did not show significant differences in the pregnancy rate, high-quality embryo rate, and available embryo rate compared to other patient groups. This suggests that natural cycles may yield more good-quality embryos compared to stimulated cycles in patients with recurrent repeated failures. One reason for this could be that previous hormonal stimulation protocols can induce chromosomal abnormalities in subsequent oocytes (Munne et al. Citation1997). Additionally, the appropriate timing of oocyte retrieval plays a crucial role in the success of the procedure. The outcomes are not related to the patients’ history of repeated failures but may be directly influenced by different treatment approaches in different centres. In our centre, treatment via natural IVF/ICSI cycles may benefit patients with low ovarian reserve who have experienced repeated failures with stimulated IVF/ICSI cycles.
Despite the advantages of natural cycles, two challenges limit their widespread use. Firstly, spontaneous LH surges and premature ovulation can occur at any time, especially in patients with poor ovarian reserve. A previous study reported that the percentage of premature ovulation could be as high as 29.8% (Ingerslev et al. Citation2001). Secondly, even with appropriate timing, unsuccessful oocyte retrieval can still occur, making it difficult to predict follicle maturity and the optimal oocyte pick-up time. However, in the present study, no cycles were cancelled in either group. Furthermore, ovulation before aspiration occurred in 28 cycles (5.9%), and in 31 other natural cycles (6.5%), no oocytes were aspirated. Oocyte retrieval was successfully performed in 419 natural cycles (87.7%). Accurate prediction of the oocyte pick-up time and excellent oocyte retrieval skills contributed to a high success rate.
It is commonly believed that planning oocyte retrieval based on spontaneous LH surges requires intensive monitoring, but most laboratories and clinicians cannot provide round-the-clock service. Surprisingly, our research has revealed that the majority of oocyte retrievals in the present study were conducted between 7:00 am and 7:00 pm. This finding may aid in predicting the optimal clinical oocyte retrieval time.
One limitation of this study is that the overall pregnancy rates for the natural cycles were not available. Firstly, in some cases (82 cycles), embryos from natural cycles were combined with thawed embryos from other cycles. Additionally, in order to maximise the chances of successful pregnancy, some patients (15 cycles) need repeated natural cycles before initiating embryo transfer.
In conclusion, natural cycles with appropriate oocyte retrieval time, high-quality embryos, and a favourable pregnancy rate may represent a valuable option for patients with low ovarian reserve.
Ethical approval
The study received approval from the Medical Ethics Committee of Guangdong Second Provincial General Hospital on August 16th (2022-SZ-KY-006-01).
Informed Consent
Not applicable. The requirement for informed consent was waived by the Medical Ethics Committee of Guangdong Second Provincial General Hospital.
Supplemental Material
Download Zip (91.9 KB)Disclosure statement
No potential conflict of interest was reported by the author(s). This study adhered to the principles outlined in the Declaration of Helsinki.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Additional information
Funding
References
- Ata, B., et al., 2008. Embryo implantation rates in natural and stimulated assisted reproduction treatment cycles in poor responders. Reproductive Biomedicine Online, 17 (2), 207–212.
- Conforti, A., et al., 2019. Management of women with an unexpected low ovarian response to gonadotropin. Frontiers in Endocrinology, 10, 387.
- De Marco, M. P., et al., 2021. Natural cycle results in lower implantation failure than ovarian stimulation in advanced-age poor responders undergoing IVF: fertility outcomes from 585 patients. Reproductive Sciences , 28 (7), 1967–1973.
- Di Guardo, F., et al., 2022. Poor ovarian response and the possible role of natural and modified natural cycles. Therapeutic Advances in Reproductive Health, 16, 26334941211062026.
- DiMattina, M., et al., 2014. Follicular and estradiol parameters that improve success with natural cycle in vitro fertilization. J Reprod Med, 59, 267–273.
- Drakopoulos, P., et al., 2019. Modified natural cycle IVF versus conventional stimulation in advanced-age Bologna poor responders. Reproductive Biomedicine Online, 39 (4), 698–703.
- Elizur, S. E., et al., 2005. Modified natural cycle using GnRH antagonist can be an optional treatment in poor responders undergoing IVF. Journal of Assisted Reproduction and Genetics, 22 (2), 75–79.
- Fields, E.,., et al., 2013. Fertility (update): summary of NICE guidance. BMJ (Clinical Research ed.), 346 (1), f650–f650. and
- Højgaard, A., Ingerslev, H. J. and Dinesen, J., 2001. Friendly IVF: patient opinions. Human Reproduction , 16 (7), 1391–1396.
- Ingerslev, H. J., et al., 2001. A randomized study comparing IVF in the unstimulated cycle with IVF following clomiphene citrate. Human Reproduction , 16 (4), 696–702.
- Jirge, P. R., 2016. Poor ovarian reserve. Journal of Human Reproductive Sciences, 9 (2), 63–69.
- Joshi, N., et al., 2012. Trends and correlates of good perinatal outcomes in assisted reproductive technology. Obstetrics and Gynecology, 120 (4), 843–851.
- Kamel, R. M., 2010. Management of the infertile couple: an evidence-based protocol. Reproductive Biology and Endocrinology, 8 (1), 21.
- Kaneko, T., et al., 2000. Effects of controlled ovarian hyperstimulation on oocyte quality in terms of the incidence of apoptotic granulosa cells. Journal of Assisted Reproduction and Genetics, 17 (10), 580–585.
- Kedem, A., et al., 2014. Is the modified natural in vitro fertilization cycle justified in patients with “genuine” poor response to controlled ovarian hyperstimulation? Fertility and Sterility, 101 (6), 1624–1628.
- Kim, C. H., et al., 2009. Minimal stimulation using gonadotropin-releasing hormone (GnRH) antagonist and recombinant human follicle-stimulating hormone versus GnRH antagonist multiple-dose protocol in low responders undergoing in vitro fertilization/intracytoplasmic sperm injection. Fertility and Sterility, 92 (6), 2082–2084.
- Kolibianakis, E., et al., 2004. Modified natural cycle for IVF does not offer a realistic chance of parenthood in poor responders with high day 3 FSH levels, as a last resort prior to oocyte donation. Human Reproduction , 30 (10), 2321–2330.
- Lainas, T. G., et al., 2015. Live birth rates after modified natural cycle compared with high-dose FSH stimulation using GnRH antagonists in poor responders. Human Reproduction, 30 (10), 2321–2330.
- Lindheim, S. R., et al., 1997. Poor responders to ovarian hyperstimulation may benefit from an attempt at natural-cycle oocyte retrieval. Journal of Assisted Reproduction and Genetics, 14 (3), 174–176.
- Lindsay, T. J. and Vitrikas, K. R., 2015. Evaluation and treatment of infertility. Am Fam Physician, 91, 308–314.
- Mahutte, N. G. and Arici, A., 2007. Role of gonadotropin-releasing hormone antagonists in poor responders. Fertility and Sterility, 87 (2), 241–249.
- Morgia, F., et al., 2004. A controlled trial of natural cycle versus microdose gonadotropin-releasing hormone analog flare cycles in poor responders undergoing in vitro fertilization. Fertility and Sterility, 81 (6), 1542–1547.
- Munne, S., et al., 1997. Treatment-related chromosome abnormalities in human embryos. Human Reproduction , 12 (4), 780–784.
- Ng, E. H., et al., 2001. In vitro fertilization and embryo transfer during natural cycles. The Journal of Reproductive Medicine, 46 (2), 95–99.
- Pelinck, M. J., et al., 2002. Efficacy of natural cycle IVF: a review of the literature. Human Reproduction Update, 8 (2), 129–139.
- Phillips, S. J., et al., 2007. Controlled natural cycle IVF: experience in a world of stimulation. Reproductive Biomedicine Online, 14 (3), 356–359.
- Polyzos, N. P., et al., 2012. Live birth rates following natural cycle IVF in women with poor ovarian response according to the Bologna criteria. Human Reproduction, 27 (12), 3481–3486.
- Practice Committee of the American Society for Reproductive, Medicine. 2015. Diagnostic evaluation of the infertile female: a committee opinion. Fertil Steril, 103, e44-50.
- Rasool, S. and Shah, D., 2017. Fertility with early reduction of ovarian reserve: the last straw that breaks the Camel’s back. Fertil Res Pract, 3, 15.
- Schimberni, M., et al., 2009. Natural-cycle in vitro fertilization in poor responder patients: a survey of 500 consecutive cycles. Fertility and Sterility, 92 (4), 1297–1301.
- Van Blerkom, J. and Davis, P., 2001. Differential effects of repeated ovarian stimulation on cytoplasmic and spindle organization in metaphase II mouse oocytes matured in vivo and in vitro. Human Reproduction, 16 (4), 757–764.
- von Wolff, M., 2019. The role of natural cycle IVF in assisted reproduction. Best Practice & Research. Clinical Endocrinology & Metabolism, 33 (1), 35–45.
- Ziebe, S., et al., 2004. Embryo quality in natural versus stimulated IVF cycles. Human Reproduction , 19 (6), 1457–1460.