

Abstract
Robert’s uterus was firstly reported in 1970, it’s a rare Müllerian duct anomaly with 2 intra-uterine cavities divided by asymmetrical septum. One of the cavities is completely obstructed to cervix by septum and menstruation fluid retents in this blind cavity, periodical pelvic pain during menstruation can lead attendance to hospital. We report a gravida of Robert’s uterus with missed abortion in the blind cavity, who had mild dysmenorrhoea since adolescent age, diagnosed and treated by minimally invasive surgical methods. To our knowledge, it’s a previously unreported case which gynaecologists terminated pregnancy in blind cavity of Robert’s uterus without resecting the septum while dysmenorrhoea relieved entirely and postoperative volume of menstruation stayed the same as preoperative.
Case report
A 30-year-old woman, gravida 4, para 2, who attempted a failed induced miscarriage, presented to our hospital at 8 weeks gestation. Her menarche was at 11 years; since then, dysmenorrhoea has been present but not aggravated, and her menstrual cycles have been regular.
The patient underwent two full-termed caesarean sections. Her children were healthy, uterine appearance was normal, and menstruation was not affected by the operations. Gynecological examination showed a normal vagina, cervix, and an anterior uterus at an 8-week gestational size. Transvaginal ultrasound revealed a 1.5-cm thick septum inside the uterus and a gestational sac corresponding to 8 weeks in the left cavity; however, foetal heartbeat was absent (). Urinary tract ultrasonography results were normal.
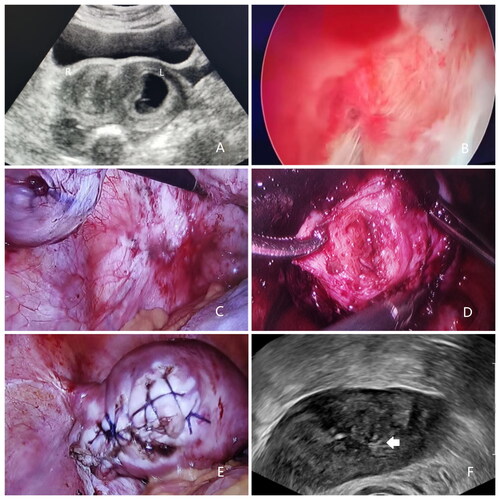
Figure 1. (A) Transvaginal ultrasound showing a septum inside the uterus and the gestational sac in the blind cavity. (B) Hysteroscopic appearance of a unicornuate uterus. (C) Violet-blue nodules are observed on the surface of the left uterosacral ligament. (D) The blind cavity was confirmed using forceps to explore. (E) The appearance of the uterus after salpingectomy and elimination of the blind cavity. (F) Transvaginal ultrasound showing the uterus with one cavity with scar (white arrow) formed in the myometrium of the former blind cavity 5 months later.
A hysteroscopy was performed; only the right fallopian ostium was observed, and the uterine cavity was narrow (). On laparoscopy, the left uterine horn bulged to 5 cm in diameter; there was no depression at the bottom of the uterus. The appendages were normal, and violet-blue nodules were observed on the left uterosacral ligament’s surface (). The bulged part was opened using an electrocautery needle, and the gestational tissues were removed from the left cavity. Forceps were used to explore and confirm the blind cavity ). Ipsilateral salpingectomy and endometrectomy (including the septal endometrium) were performed; the removed myometrium was at least 5-mm thick, and the left uterine horn’s residual myometrium was sutured to the septum to eliminate the blind cavity (). The endometriotic lesions were treated with bipolar electrocoagulation.
A transvaginal ultrasonography 5 months later revealed that the uterus had one cavity with a scar in the myometrium of the former blind cavity (). The patient reported that postoperative menstruation with regular cycles occurred four times, menstruation volume was same as preoperatively, and dysmenorrhoea ceased.
Discussion
Patients with Robert’s uterus usually visit hospital for progressively worsening dysmenorrhoea and have disappointing pregnancy outcomes with recurrent losses and infertility (Liu et al. Citation2022).
Musset and Poitout (Citation1974) described three Robert’s uterus characteristics: (1) primary dysmenorrhoea, (2) discordance between the normal laparoscopic appearance and hysterographic appearance of a unicornuate uterus, and (3) a normal urinary system. The extremely rare pregnancies in these patients possibly result from transperitoneal migration of the sperm via the cervix, contralateral cavity, and fallopian tubes (Singhal et al. Citation2003).
When encountering this abnormality, a unicornuate uterus with a noncommunicating rudimentary horn, defined as type A1b according to the American Fertility Society (Khati et al. Citation2012), should be distinguished, because these malformations can also cause symptoms such as dysmenorrhoea and miscarriage, and a depression at the bottom of the uterus should be confirmed. Recent reports (Ludwin et al. Citation2016) have demonstrated the importance of imaging examinations, such as MRI or 3-D ultrasound, in diagnosing Robert’s uterus. We approve of their viewpoints. Meanwhile, we highlight the minimally invasive surgery’s application in treating Robert’s uterus, especially when an unexpected pregnancy occurs in the blind cavity. The combination of hysteroscopy and laparoscopy allows direct observation of the anomaly, offering more choices for treatment (Siam and Soliman Citation2014).
Surgery normalises the uterine morphology, protects fertility, and prevents dysmenorrhoea. While hysteroscopic septal electrotomy must be performed under ultrasonographic or laparoscopic guidance, and mostly requires a second surgery to incise the intrauterine adhesions, despite use of combined oral contraceptives or intrauterine devices, endometrectomy and ipsilateral salpingectomy can eliminate the dysmenorrhoea. A case of pregnancy with Robert’s uterus after endometrectomy has been reported (Vural et al. Citation2011).
Benzineb et al. (Citation1993) first reported a terminated pregnancy in a Robert’s uterus’ blind cavity via laparotomy. Another case of Robert’s uterus with pregnancy in a blind hemi-cavity was treated by hysteroscopic metroplasty (Yang et al. Citation2019). The patient underwent a second surgery because of residual gestational tissue seen on 3D ultrasound 2 weeks after the first procedure performed under trans-abdominal ultrasonographic and laparoscopic guidance. Liu et al. (Citation2021) reported a similar case; however, the pregnancy was terminated via hysterectomy.
Our patient had dysmenorrhoea and conceived in the blind cavity. Hysteroscopic septal electrotomy was not appropriate because, (1) dysmenorrhoea would continue if laparoscopic electrocoagulation was not performed for the endometriosis; (2) the patient’s septum was thick, and the pregnant uterus bled easily, with the bloody hysteroscopic surgical field making surgery difficult; (3) the tissues of missed miscarriage adhered to the uterine wall, and the septum was large; therefore, intrauterine adhesions or residual gestation tissue was likely to be present after hysteroscopic electrotomy, rendering a second surgery inevitable; and (4) the patient had full-termed deliveries twice by caesarean sections, and theoretically, her fertile function was not impaired by the septum. Therefore, we performed a laparoscopic endometrectomy, with the removed myometrium measuring at least 5 mm, to prevent iatrogenic adenomyosis. Consequently, missed miscarriage and dysmenorrhoea were treated simultaneously and satisfactorily, and a second surgery was avoided.
Ethical approval
The patient gave informed consent for treatment and publication of this case report. Approval by the Medical Ethics Committee of The second people’s hospital of Guiyang (No. 2023WZ01) was received for publication of this case report.
Author contributions
H. Y. was involved in project development, case analysis and manuscript writing.
Y. S. was involved in project development, figures editing and manuscript editing.
G. J. was involved in project development, manuscript revising, and other (treatment procedure).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Additional information
Funding
References
- Benzineb, N., et al., 1993. Robert’s uterus with menstrual retention in the blind cavity. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction, 22 (4), 366–368.
- Khati, N.J., Frazier, A.A. and Brindle, K.A., 2012. The unicornuate uterus and its variants: clinical presentation, imaging findings, and associated complications. Journal of Ultrasound in Medicine, 31 (2), 319–331.
- Liu, Y., et al., 2021. Pregnancy in the blind hemi-cavity of Robert’s uterus: a case report. Radiology Case Reports, 16 (5), 1085–1088.
- Liu, Y., Hou, C. and Zhou, Y., 2022. Ultrasound combined with hysteroscopy for optimum treatment of Robert’s uterus: a case report and a review. BMC Women’s Health, 22 (1), 334.
- Ludwin, A., Ludwin, I. and Martins, W.P., 2016. Robert’s uterus: modern imaging techniques and ultrasound-guided hysteroscopic treatment without laparoscopy or laparotomy. Ultrasound in Obstetrics & Gynecology, 48 (4), 526–529.
- Musset, R. and Poitout, P., 1974. A further case of asymetrically divided uterus. Role of the isthmus in the initiation of menstruation. Journal of Gynecology and Obstetrics and Reproductive Biology, 3 (7), 1117–1122.
- Siam, S. and Soliman, B.S., 2014. Combined laparoscopy and hysteroscopy for the detection of female genital system anomalies results of 3,811 infertile women. Journal of Reproductive Medicine, 59 (11–12), 542–546.
- Singhal, S., et al., 2003. Pregnancy in asymmetric blind hemicavity of Robert’s uterus–a previously unreported phenomenon. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 107 (1), 93–95.
- Vural, M., et al., 2011. Favourable pregnancy outcome after endometrectomy for a Robert’s uterus. Journal of Obstetrics and Gynaecology, 31 (7), 668–669.
- Yang, Q.M., et al., 2019. Pregnancy in a blind hemi-cavity of Robert’s uterus with ipsilateral renal agenesis: a case report and literature review. The Journal of International Medical Research, 47 (7), 3427–3434.