

Abstract
Background
Haemostasis during ovarian cystectomy is reported to damage the ovarian reserve, but the comparative impacts of three haemostasis methods (bipolar energy, suture and haemostatic sealant) on ovarian reserve in patients with ovarian cysts are not well known.
Methods
The Cochrane Library, PubMed and Web of Science databases were searched from the date of inception of the database to June 2022 for literature exploring the impact of haemostasis methods during ovarian cystectomy on ovarian reserve. A traditional meta-analysis was performed using Review Manager software. A network meta-analysis (NMA) was performed using Stata and GemTC software.
Results
The direct meta-analysis comparison indicated that the mean postoperative reduction of anti-Müllerian hormone (AMH) level was significantly higher in the electrocoagulation (bipolar) group than suture and haemostatic sealant group, both in the overall group and subgroup of women with ovarian endometrioma. In NMA, the reduction of postoperative AMH levels in the electrocoagulation (bipolar) group was higher than the suture group at 6 months with a statistical significance, and at 1, 3 and 12 months without a significant difference. The difference in the postoperative decrease of AMH level did not reach statistical significance between suture and sealant, coagulation and haemostatic sealant. The comprehensive ranking results revealed that suture treatment was, with the highest probability, beneficial to the protection of the ovarian reserve.
Conclusions
There was insufficient research to detect the optimal haemostasis method for ovarian reserve preservation in ovarian cystectomy. Nevertheless, haemostasis by electrocoagulation (bipolar) should be avoided when possible, and the suture might be considered as the best choice.
Plain Language Summary
Haemostasis during ovarian cystectomy is reported to damage the ovarian reserve, but the comparative impacts of three haemostasis methods (bipolar energy, suture and haemostatic sealant) on ovarian reserve in patients with ovarian cysts are not well known. The level of AMH is the most widely used surrogate for ovarian reserve. Our research compared the impact of three haemostasis methods (electrocoagulation, suture and haemostatic sealant) on changes in the levels of anti-Müllerian hormone at 1, 3, 6 and 12 month(s) after the operation. The outcomes revealed that there was insufficient research to detect the optimal haemostasis method for ovarian preservation in ovarian cystectomy. Nevertheless, haemostasis by electrocoagulation (bipolar) should be avoided when possible, and the suture might be considered as the best choice.
1. Introduction
The ovarian cyst is a common gynaecological presentation seen in approximately 6.6% of reproductive-age women (Borgfeldt and Andolf Citation1999). The management of ovarian cysts in premenopausal women will rely on the size of the lesion, the presence of symptoms, fertility desires and the underlying pathology (Farahani and Datta Citation2016, Poplawski and Ma Citation2022). Up to 10% of women would have surgery for an ovarian cyst in their lifetime (Poplawski and Ma Citation2022), and ovarian cystectomy is more favourable among these surgical treatments, even in old women (Yildiz et al. Citation2020). However, though the ovarian cysts are solved, women after surgical management were found with a diminished ovarian reserve and risk of premature ovarian failure (Jones et al. Citation2000, Canis et al. Citation2001, Ragni et al. Citation2005, Ding et al. Citation2015), which was attached with great emphasis.
The histology and size of ovarian cysts are important determinants of the severity of ovarian reserve under the surgery. An ovarian endometriosis cyst and ovarian cysts with a diameter of 5 cm or more are more detrimental to ovarian reserve (Henes et al. Citation2018, Yildiz et al. Citation2020). Apart from the surgical removal of a part of the healthy ovarian tissue and the cyst’s wall, the mode of bleeding control of the ovarian wound ground is also paramount in ovarian reserve preservation. The haemostasis is often conducted by electrocoagulation, suture and haemostatic agents. In the bipolar coagulation treatment, haemostasis of the ovarian parenchyma is achieved with selective minimal bipolar coagulation (20–30 W current). The sutures are performed with intracorporeal knots using 2-0 polyglactin absorbable sutures, and suture is performed using needle holders for the closure of ovarian parenchyma and controlling bleeding. Haemostatic agents are applied to covered bleeding sites under direct vision, of which the FloSeal is widely used. The FloSeal is a novel matrix haemostatic sealant composed of collagen-derived particles and topical bovine-derived thrombin, facilitating the formation of stable clots at the bleeding site (Angioli et al. Citation2009, Ebert et al. Citation2009, Song et al. Citation2014). Coagulation was considered inferior to the haemostasis method of suture and the FloSeal treatment in terms of ovarian reserve protection (Fedele et al. Citation2004, Li et al. Citation2009, Coric et al. Citation2011, El Behery et al. Citation2011, Song et al. Citation2014, Asgari et al. Citation2016, Zhang et al. Citation2016, Sahin et al. Citation2017, Choi et al. Citation2018, Shaltout et al. Citation2019, Xiao et al. Citation2019, E. Y. Park et al. Citation2020, S. J. Park et al. Citation2020, Chung et al. Citation2021, Park et al. Citation2021, Mohamed et al. Citation2011). However, others found no differences (Ferrero et al. Citation2012, Özgönen et al. Citation2013, Tanprasertkul et al. Citation2014, Owczarek et al. Citation2018, Chung et al. Citation2019, da Cunha Araujo et al. Citation2022). Meanwhile, few studies directly compared the damage of ovarian reserve between the suture and the haemostatic sealant treatment.
Anti-Müllerian hormone (AMH), produced by granulosa cells of preantral and small antral follicles, could accurately predict antral follicle pool size (Cedars Citation2022). Besides, some research indicated that AMH could prevent premature exhaustion of the ovarian reserve by regulating the number of primordial follicles that enter the maturation process and could be an indirect predictor of the primordial follicles (Farhat et al. Citation2022). The level of AMH is widely used as a surrogate for ovarian reserve which is known as the number of primordial follicles that could develop into primary, antral and ovulatory follicles at a particular time in a woman’s life (Iwase et al. Citation2010, Moolhuijsen and Visser Citation2020). Meanwhile, AMH level was potential as a diagnostic and predictive biomarker of premature ovarian insufficiency. The level of AMH is independent of the menstrual cycle and unaffected by hormone use, which was therefore equipped with the most reliable and reproducible outcome (Kalampokas et al. Citation2013, Dewailly et al. Citation2014).
Based on the fact that no consensus has arrived regarding the ovarian reserve preservation of different haemostatic methods and the insufficiency of comparison between the suture and haemostatic agents, a traditional meta-analysis and a network meta-analysis (NMA) were performed in our study. The NMA could integrate the results of direct and indirect comparisons to comprehensively evaluate the impact of haemostatic methods (bipolar energy, suture and sealants) on AMH level during ovarian cyst management. In addition, it was able to rank the efficacy of the other haemostasis in preserving ovarian reserve during different periods in the follow-up (1 month, 3 months, 6 months and 12 months) to guide clinical decision-making for women under ovarian cystectomy.
2. Methods
2.1. Literature search
With guidelines of the preferred reporting items for systematic reviews and meta-analyses (PRISMA), the Cochrane Library, PubMed and Web of Science were searched. The search time was limited from the date of inception of the database to June 2022. The following keywords and subject terms were used: (Ovarian cysts) and (Laparoscopy OR Hemostasis OR suture OR sealants OR ((Ovarian cystectomy) OR (Surgical Energy) OR Electrocoagulation OR coagulation OR electrocautery)) and (fertility OR pregnant OR (Ovarian function) OR (Ovarian reserve) OR ((anti-Müllerian hormone) OR AMH) OR ((Müllerian inhibiting substance) OR MIS)). This study was registered in the PROSPERO and the ID is CRD42023467168.
2.2. Study selection
The inclusion criteria were: ① RCT study; ② patients were diagnosed as an ovarian cyst with a plan to ovarian cystectomy; ③ one of the three haemostasis methods including suture or electrocoagulation (bipolar) or the haemostatic sealant was used; ④ the change of AMH value of 1 month, 3 months, 6 months or 12 months after the cystectomy surgery was recorded or could be calculated. Studies were excluded if they were not published in English and the level of AMH was not presented in the form of mean ± SD.
The title and abstract were screened for relevance, and the full texts were further reviewed for relevance and data extraction. Two authors (Q.X. and Y.X.) conducted the study selection process independently.
2.3. Data extraction
Variables extracted by two reviewers (Q.X. and Y.X.) independently included: study characteristics (authors and publication year), patient characteristics (inclusion criteria and exclusion criteria), haemostasis methods, sample size, the AMH level before and after surgery or the changes in AMH values of 1 month, 3 months, 6 months and 12 months after the cystectomy surgery. If any discrepancies existed, Y.S. and X.Z.Q. would involve in and resolve them by consensus of the reviewers.
2.4. Quality assessment
Studies included in our research were RCTs; therefore, they were assessed according to the Cochrane Handbook of Systematic Reviews of Interventions. Assessment categories included seven domains: (1) sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessment; (5) incomplete outcome data; (6) selective reporting and (7) other bias. Two reviewers (Q.X. and Y.X.) independently assessed the risk of bias. Y.S. and X.Z.Q. coped with any disagreements.
2.5. Data synthesis and statistical analysis
The traditional pairwise meta-analysis was conducted by Review Manager 5.4.1 (Copenhagen, Denmark). If the AMH level before and after the ovarian surgery but not the postoperative changes were reported in the original research, the postoperative changes were calculated according to the Cochrane Handbook for Systematic Reviews of Interventions (v6.4). The changes in AMH values of 1, 3, 6 months and 12 months after the cystectomy surgery were a continuous variable and presented as mean ± SD. The AMH of the included research was quantified using a standard enzyme-linked immunosorbent assay in ng/mL, so the weighted mean difference (WMD) of each original study was determined by the accuracy of its effect estimates. Ranges of WMDs were shown with a 95% confidence interval (95% CI). Statistical heterogeneity was assessed by the I2 statistic and p value (I2 > 50%, p < .05 showed apparent heterogeneity). Publication bias and sensitivity analysis were conducted by Review Manager 5.4.1 (Copenhagen, Denmark) and STATA/MP 17.0 (StataCorp, College Station, TX).
The net meta-analysis was conducted by STATA/MP 17.0 (StataCorp, College Station, TX) and GeMTC 0.14.3. Stata software was used to depict the Network graphs, and GeMTC software was used to carry out the data synthesis. The operating parameter of GeMTC software during net meta-analysis was as follows: the number of chains was four; initial value scaling was 10; tuning iterations were 20,000; simulation iterations were 50,000; thinning iterations were 10. The inconsistency model was used first, and then the value of inconsistency factors was analysed. Inconsistency factors were closer to zero, the consistency was better. Meanwhile, if the consistency was well, the value of the random effect standard and inconsistency standard would be comparable. All evaluated treatments were ranked using the Bayesian approach in the range of 0–100%.
At last, the hot map showing the outcome of probabilities of the ranking was made by the GraphPad prism (La Jolla, CA). All tables were produced in Word or Excel (Microsoft, Redmond, WA).
3. Results
3.1. Study selection
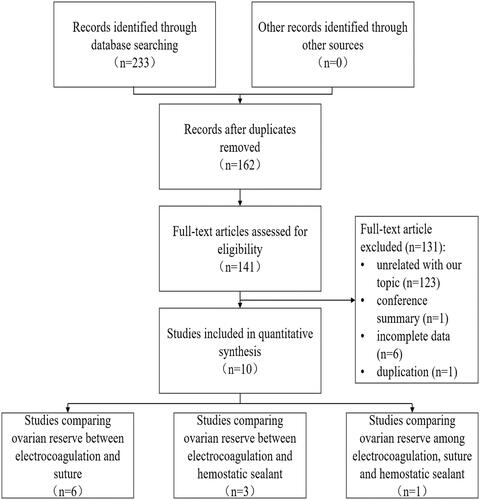
As depicted in , 233 records were searched from electronic databases, including PubMed, Cochrane and Web of Science. After the removal of duplicates, 162 records remained. Titles, abstracts and full text of these manuscripts were further screened, and 10 studies were potentially considered eligible for inclusion and quantitative synthesis. Among these ten studies, six and three studies compared the ovarian reserve preservation between electrocoagulation (bipolar) and suture, electrocoagulation (bipolar) and haemostatic sealant, respectively. Only one study included electrocoagulation (bipolar), suture and haemostatic sealant simultaneously.
Figure 1. PRISMA flow diagram for identification and selection of studies.
3.2. Study characteristics
Characteristics of the ten studies included are summarised in . All analyses were prospective, randomised and controlled trials. Five recruited patients with ovarian endometrioma and the other with undefined cyst type. Among the ten pieces of research, six studies totalling 490 women, five studies totalling 490 women, five studies totalling 431 women and two studies totalling 197 women compared the AMH value changes between coagulation and suture in 1, 3, 6 and 12 months after the ovarian operation, respectively. On the other hand, two, three and two researches were comparing AMH value changes between coagulation and haemostatic sealant in 1, 3 and 6 months after ovarian cystectomy, respectively, with total participants varying from 126 to 221. The postoperative AMH value changes of 12 months between coagulation and haemostatic sealant were compared in one study with a total of 71 women. Besides, only one study included both the haemostatic methods of suture (26 women) and haemostatic sealant (24 women), which compared the AMH value changes in 1 and 6 months after the surgery.
Table 1. Characteristics of randomised controlled trials included in the quantitative analysis.
3.3. Quality assessment
The quality assessment of the 10 RCTs is shown in Figure S1. Eight trials (80%) performed remarkably on the random sequence generation and allocation concealment, regarded as with a low risk of bias. The rest (20%) had an unclear risk of bias. As for blinding of participants and personnel, one study (10%) showed a high risk of bias, three studies (30%) showed a low risk of bias, and six studies (60%) showed an unclear risk of bias. Five RCTs (50%) with low risk and five studies (50%) with unclear risk of blinding of outcome assessment. All research (100%) had a low risk of bias on incomplete outcome data, selective reporting and others.
3.4. Results of a direct meta-analysis comparison
In the traditional meta-analysis of postoperative changes of AMH level, the mean reduction of AMH in electrocoagulation (bipolar) group, compared to the suture, was more significant at 1 month (WMD −0.58, 95% CI −0.81 to −0.34), 3 months (WMD −0.72, 95% CI −11.87 to −0.38), 6 months (WMD −0.68, 95% CI −0.90 to −0.45) and 12 months (WMD −1.08, 95% CI −1.60 to −0.56) after the surgery, respectively, shown in . The decrease in AMH level 1 month after the ovarian surgery was not significant in the electrocoagulation (bipolar) group and the haemostatic sealant group (WMD 0.18, 95% CI −0.34 to 0.71). The mean reduction of AMH was significantly higher in the electrocoagulation (bipolar) group than haemostatic sealant group at 3 (WMD −0.45, 95% CI −0.61 to −0.30), and 6 months (WMD −0.43, 95% CI −0.59 to −0.27). Only one study compared the AMH level at a follow-up time of 12 months, which indicated that the postoperative decrease of AMH level in the electrocoagulation (bipolar) group was significantly higher than in the haemostatic sealant group (WMD −0.59, 95% CI −0.78 to −0.37), as shown in Figure S2.
Figure 2. Forest plot for the estimates of postoperative changes of AMH level between bipolar coagulation and suture.
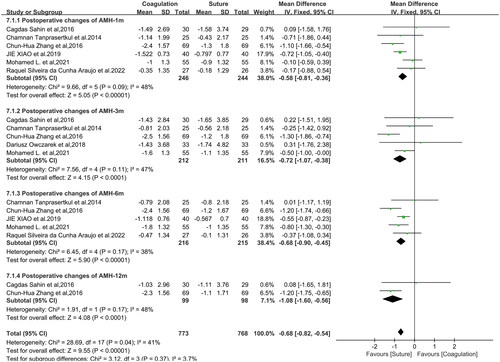
Meanwhile, when researches of different follow-up times were taken together, the reduction of AMH level in the electrocoagulation (bipolar) was higher than the suture group (WMD −0.68, 95% CI −0.82 to −0.56). Besides, the electrocoagulation (bipolar) caused a more significant decrease in the AMH level than the haemostatic sealant group (WMD −0.46, 95% CI −0.55 to −0.37), as shown in and Figure S2.
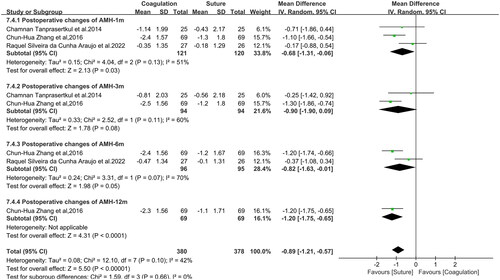
Subgroup analysis of ovarian endometrioma was conducted. The mean reduction of AMH in electrocoagulation (bipolar) group, compared to the suture, was more significant at 1 month (WMD −0.68, 95% CI −1.31 to −0.06), 6 (WMD −0.82, 95% CI −1.61 to −0.01) and 12 months (WMD −1.20, 95% CI −1.75 to −0.65) but not 3 months (WMD −0.90, 95% CI −1.90 to 0.09) after the surgery, respectively, shown in . The total analysis of 1, 3, 6 and 12 months indicated that the postoperative decrease of AMH level in the electrocoagulation (bipolar) group was significantly higher than in the suture group (WMD −0.89, 95% CI −1.21 to −0.57). On the other hand, as shown in Figure S3, the postoperative decrease of AMH level was significant between the electrocoagulation (bipolar) group and the sealant group in 3 (WMD −0.46, 95% CI −0.61 to −0.30), 6 (WMD −0.43, 95% CI −0.59 to −0.27) and 12 (WMD −0.59, 95% CI −0.78 to −0.40) months but not 1 month (WMD 0.18, 95% CI −0.34 to 0.71) after the ovarian surgery. The total analysis of 1, 3, 6 and 12 months indicated that the postoperative decrease of AMH level in the electrocoagulation (bipolar) group was significantly higher than in the sealant group (WMD −0.46, 95% CI −0.56 to −0.37).
Figure 3. Forest plot of subgroup analysis with ovarian endometrioma for the estimates of postoperative changes of AMH level between bipolar coagulation and suture.
3.5. Results of a network meta-analysis comparison
To explore the comparative results between the suture group and haemostatic sealant group and to pool data from individual studies, the NMA of AMH level between three haemostasis methods was constructed. The overall situation of the comparison is shown in Figure S4 and the NMA results are presented in . The postoperative decrease of AMH level seemed comparable in the haemostatic sealant group and the suture group with no statistical significance at the follow-up time of 1 month (WMD −0.54, 95% CI −1.58 to 0.55), 3 months (WMD −0.29, 95% CI −1.33 to 0.86), 6 months (WMD −0.31, 95% CI −1.07 to 0.34) and 12 months (WMD −0.37, 95% CI −2.18 to 1.82).
Table 2. League table of results from a network meta-analysis for the preservation of ovarian reserve indicated by the postoperative changes of AMH level.
The reduction of postoperative AMH levels in the electrocoagulation (bipolar) group was higher than the suture group at 6 months (WMD −0.68, 95% CI −1.11 to −0.22) with a statistical significance, and at 1 (WMD −0.46, 95% CI −1.08 to 0.16), 3 (WMD −0.60, 95% CI −1.23 to 0.22) and 12 months (WMD −0.95, 95% CI −2.10 to 0.51) without a significantly difference. Meanwhile, compared with the haemostatic sealant group, the postoperative level of AMH in the electrocoagulation (bipolar) group was also decreased at 1 (WMD 0.07, 95% CI −0.91 to −0.03), 3 (WMD −0.64, 95% CI −1.45 to −0.03), 6 (WMD −0.64, 95% CI −1.45 to −0.03) and 12 months (WMD −0.64, 95% CI −1.45 to −0.03) without statistical significance.
3.6. Comprehensive ranking results
The surface under the cumulative ranking area (SUCRA) was further used to provide a hierarchical ranking of electrocoagulation (bipolar), suture and haemostatic sealant treatment. The SUCRA is a numeric presentation of an overall ranking that presents a single number associated with each treatment and ranges from 0 to 1. As shown in , the postoperative decrease of AMH level of the suture group (rank 1: 0.81, 0.72, 0.87, 0.67) was less compared to electrocoagulation (bipolar) and the sealant treatment in 1, 3, 6 and 12 months after the ovarian surgery, respectively. About electrocoagulation (bipolar) and the sealant treatment, the sealant treatment with high probability in rank 2 in 3 (0.55), 6 (0.78) and 12 months (0.54) but in rank 3 (0.54) in 1 month after the surgery.
Table 3. Probabilities of the ranking of three haemostasis for ovarian preservation.
3.7. Publication bias and sensitivity analysis
Publication bias is indicated in Figures S5 and S6 by visual examination of funnel plots. Publication bias in research comparing electrocoagulation and suture seemed low, and comparing electrocoagulation and sealant seemed moderate. Sensitivity analysis was indicated in Supplemental Figures S7 and S8. It revealed that the comparative results between electrocoagulation and suture, electrocoagulation and haemostatic sealant group were robust.
4. Discussion and conclusions
This pairwise and NMA evaluated the ovarian reserve in haemostasis with electrocoagulation, suture or haemostatic sealant among women with ovarian cystectomy. AMH is considered the preferred ovarian reserve marker. Higher AMH may indicate better ovarian reserve. Although the included research was insufficient, our study showed that electrocoagulation was inferior to the suture and haemostatic sealant in terms of postoperative change of AMH level, and the suture was comparable to the haemostatic sealant. According to the SUCRA, suture is probably the best haemostasis, and electrocoagulation is the worst.
The NMA demonstrates that considering the ovarian reserve, haemostasis with electrocoagulation haemostasis after ovarian cystectomy should be avoided. The detailed mechanism(s) by which electrocoagulation damages the level of AMH needed to be clarified. The mechanism might be the thermal injury of normal ovarian tissue and follicle development. The detrimental effect of electrocoagulation on ovarian reserve was demonstrated before (Fedele et al. Citation2004, Li et al. Citation2009, Coric et al. Citation2011, El Behery et al. Citation2011, Song et al. Citation2014, Ata et al. Citation2015, Asgari et al. Citation2016, Zhang et al. Citation2016, Peters et al. Citation2017, Sahin et al. Citation2017, Choi et al. Citation2018, Shaltout et al. Citation2019, Xiao et al. Citation2019, E. Y. Park et al. Citation2020, S. J. Park et al. Citation2020, Chung et al. Citation2021, Park et al. Citation2021). Electrocoagulation was associated with a more significant decline in serum AMH levels than alternative haemostatic methods, such as suture and haemostatic sealant. Although electrocoagulation is easy to operate and useful to clot blood quickly, it should be avoided as much as possible for women with fertility desires.
Haemostasis of suture and sealant are better than electrocoagulation in preserving ovarian reserve. Nevertheless, the comparison between the suture and haemostatic sealant was urgently required due to inadequate research. In our study, the suture is thought to be the optimal haemostasis in the SUCRA analysis which pooled data from all studies. Only one study compared the AMH level after surgery in the suture group with the haemostatic sealant group and no difference was found (da Cunha Araujo et al. Citation2022). Theoretically, haemostatic sealant is less invasive to the ovaries than sutures, on the other hand, sutures could promote the ovarian border adjacent, which might be well for the recovery of ovarian function.
The outcomes of our research were consistent with the previous two meta-analysis articles (Ata et al. Citation2015, Peters et al. Citation2017). They found that suturing for haemostasis was superior to surgical energy in preserving ovarian function. However, in the research of Ata et al. (Citation2015), the quality of evidence favouring haemostatic sealant over bipolar coagulation was stronger than evidence favouring suture over bipolar coagulation. No direct comparison was conducted between the haemostatic sealant group and the suture group. Whether haemostatic sealant was better or not needs to be further identified by large, prospective, randomised controlled research.
Our study has several strengths. First, the first data for the overview of three different haemostasis (electrocoagulation, suture or haemostatic sealant) in women with ovarian cysts undergoing ovarian cystectomy were provided. Second, four other follow-up times (1 month, 3 months, 6 months and 12 months) are recorded in our study. Third, based on the direct and indirect comparisons, a unique opportunity was provided to rank the three haemostasis simultaneously in one pooled analysis, which may have important implications for clinical practice.
There existed some limitations requiring attention. First, owing to strict inclusion and exclusion criteria, only 10 RCTs were included in this net meta-analysis, which limited the application of the evidence assessment approach and affected the credibility of the final evaluation of results. Second, variations exist within inclusion and exclusion criteria, including the number of ovarian cysts, types of cysts, watt for bipolar coagulation, etc. Five RCTs included recruited patients with ovarian endometrioma, patients of the other five RCTs have ovarian cysts of unknown type. Therefore, the subgroup analysis could only be conducted by women with ovarian endometrioma in the five RCTs but not by follicular cysts or dermoid cysts. Meanwhile, when used for haemostasis of the ovarian parenchyma, the watt for bipolar coagulation is usually 20–30 W current. However, two pieces of research included applied 35–40 W current, which might damage the ovarian reserve more seriously. Third, AMH was an accurate measure of antral follicle count (AFC) but not the primordial follicles, and some researchers showed that AMH had limited prognostic value for the density of primordial and primary follicles (von Wolff et al. Citation2019, Citation2020). Therefore, the predictable ability of AMH on ovarian reserve was in question though AMH was widely used to evaluate the ovarian reserve in clinics and research (Anderson et al. Citation2022, Cedars Citation2022, Daniilidis et al. Citation2023). Meanwhile, only the level of AMH was compared in our study, indicators of ovarian reserves, such as basal AFC, follicle stimulation hormone (FSH), oestradiol (E2), ovarian arterial peak systolic velocity (PSV), ovarian volume (OV), etc., were not analysed, which were be relevant to ovarian reserve. Moreover, in research with the AMH level before and after the ovarian surgery but not the postoperative changes, the postoperative changes of AMH value were calculated according to the Cochrane Handbook for Systematic Reviews of Interventions (v6.4), which to some extent, might increase the inaccuracy of the results.
In conclusion, this review and NMA demonstrated that there was insufficient research to detect the optimal haemostasis method for ovarian reserve preservation in ovarian cystectomy. Nevertheless, haemostasis by electrocoagulation (bipolar) should be avoided when possible. In addition, the suture was considered the best haemostasis in the result of the ranking possibilities. Well-designed RCTs and high-quality evidence are required for future meta-analyses to better guide clinical practice.
Ethics statement
All research included was searched from databases. When these researches conducted, they were complied with the Ethics of Experimentation. Therefore, registration of all subjects or ethical approval is not applicable.
Supplemental Material
Download Zip (5.5 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Additional information
Funding
References
- Anderson, R.A., et al., 2022. Anti-Müllerian hormone as a marker of ovarian reserve and premature ovarian insufficiency in children and women with cancer: a systematic review. Human Reproduction Update, 28 (3), 1–11.
- Angioli, R., et al., 2009. Feasibility of the use of novel matrix hemostatic sealant (FloSeal) to achieve hemostasis during laparoscopic excision of endometrioma. Journal of Minimally Invasive Gynecology, 16 (2), 153–156.
- Asgari, Z., et al., 2016. Comparing ovarian reserve after laparoscopic excision of endometriotic cysts and hemostasis achieved either by bipolar coagulation or suturing: a randomized clinical trial. Archives of Gynecology and Obstetrics, 293 (5), 1015–1022.
- Ata, B., et al., 2015. Effect of hemostatic method on ovarian reserve following laparoscopic endometrioma excision; comparison of suture, hemostatic sealant, and bipolar dessication. A systematic review and meta-analysis. Journal of Minimally Invasive Gynecology, 22 (3), 363–372.
- Borgfeldt, C. and Andolf, E., 1999. Transvaginal sonographic ovarian findings in a random sample of women 25–40 years old. Ultrasound in Obstetrics & Gynecology, 13, 6.
- Canis, M., et al., 2001. Ovarian response during IVF–embryo transfer cycles after laparoscopic ovarian cystectomy for endometriotic cysts of >3 cm in diameter. Human Reproduction, 16 (12), 2583–2586.
- Cedars, M.I., 2022. Evaluation of female fertility—AMH and ovarian reserve testing. Journal of Clinical Endocrinology and Metabolism, 107 (6), 1510–1519.
- Choi, C., et al., 2018. Usefulness of hemostatic sealants for minimizing ovarian damage during laparoscopic cystectomy for endometriosis. Journal of Obstetrics and Gynaecology Research, 44 (3), 532–539.
- Chung, J., et al., 2019. Impact of haemostatic sealant versus electrocoagulation on ovarian reserve after laparoscopic ovarian cystectomy of ovarian endometriomas: a randomised controlled trial. British Journal of Gynecology, 126 (10), 1267–1275.
- Chung, J.P.W., et al., 2021. Ovarian reserve and recurrence 1 year post-operatively after using haemostatic sealant and bipolar diathermy for haemostasis during laparoscopic ovarian cystectomy. Reproductive Biomedicine Online, 43 (2), 310–318.
- Coric, M., et al., 2011. Electrocoagulation versus suture after laparoscopic stripping of ovarian endometriomas assessed by antral follicle count: preliminary results of randomized clinical trial. Archives of Gynecology and Obstetrics, 283 (2), 373–378.
- da Cunha Araujo, R.S., et al., 2022. Ovarian function following use of various hemostatic techniques during treatment for unilateral endometrioma: a randomized controlled trial. International Journal of Gynaecology and Obstetrics, 157 (3), 549–556.
- Daniilidis, A., et al., 2023. Surgical management of ovarian endometrioma: impact on ovarian reserve parameters and reproductive outcomes. Journal of Clinical Medicine, 12 (16), 5324.
- Dewailly, D., et al., 2014. The physiology and clinical utility of anti-Mullerian hormone in women. Human Reproduction Update, 20 (3), 370–385.
- Ding, Y., et al., 2015. Comprehensive assessment of the impact of laparoscopic ovarian cystectomy on ovarian reserve. Journal of Minimally Invasive Gynecology, 22 (7), 1252–1259.
- Ebert, A.D., et al., 2009. Laparoscopic ovarian cystectomy without bipolar coagulation or sutures using a gelantine–thrombin matrix sealant (FloSeal): first support of a promising technique. Archives of Gynecology and Obstetrics, 280 (1), 161–165.
- El Behery, M.M., et al., 2011. Effect of laparoscopic ovarian drilling on vascular endothelial growth factor and ovarian stromal blood flow using 3-dimensional power Doppler. International Journal of Gynaecology and Obstetrics, 112 (2), 119–121.
- Farahani, L. and Datta, S., 2016. Benign ovarian cysts. Obstetrics, Gynaecology & Reproductive Medicine, 26 (9), 271–275.
- Farhat, S.A., et al., 2022. Targeting signaling pathways involved in primordial follicle growth or dormancy: potential application in prevention of follicular loss and infertility. Expert Opinion on Biological Therapy, 22 (7), 871–881.
- Fedele, L., et al., 2004. Bipolar electrocoagulation versus suture of solitary ovary after laparoscopic excision of ovarian endometriomas. Journal of the American Association of Gynecologic Laparoscopists, 11 (3), 344–347.
- Ferrero, S., et al., 2012. Hemostasis by bipolar coagulation versus suture after surgical stripping of bilateral ovarian endometriomas: a randomized controlled trial. Journal of Minimally Invasive Gynecology, 19 (6), 722–730.
- Henes, M., et al., 2018. Ovarian cyst removal influences ovarian reserve dependent on histology, size and type of operation. Women’s Health, 14, 174550651877899.
- Iwase, A., et al., 2010. Serum anti-Mullerian hormone level is a useful marker for evaluating the impact of laparoscopic cystectomy on ovarian reserve. Fertility and Sterility, 94 (7), 2846–2849.
- Jones, K.D., Christopher, J.G., and Sutton, 2000. Laparoscopic management of ovarian endometriomas: a critical review of current practice. Current Opinion in Obstetrics & Gynecology, 12 (4), 309–315.
- Kalampokas, T., et al., 2013. AMH after laparoscopic surgery of the ovaries: a review. Gynecological Endocrinology, 29, 408–411.
- Li, C.-Z., et al., 2009. The impact of electrocoagulation on ovarian reserve after laparoscopic excision of ovarian cysts: a prospective clinical study of 191 patients. Fertility and Sterility, 92 (4), 1428–1435.
- Mohamed, M.L., et al., 2011. Effect on ovarian reserve of laparoscopic bipolar electrocoagulation versus laparotomic hemostatic sutures during unilateral ovarian cystectomy. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 114 (1), 69–72.
- Moolhuijsen, L.M.E. and Visser, J.A., 2020. Anti-Mullerian hormone and ovarian reserve: update on assessing ovarian function. Journal of Clinical Endocrinology and Metabolism, 105 (11), 3361–3373.
- Owczarek, D., Malinowski, A., and Wilczyński, M., 2018. Ovarian reserve evaluation after laparoscopic cyst enucleation, depending on applied haemostasis technique and with particular consideration of endometrial cysts. Przeglad Menopauzalny = Menopause Review, 17 (1), 22–27.
- Özgönen, H., et al., 2013. Comparison of the effects of laparoscopic bipolar electrocoagulation and intracorporeal suture application to ovarian reserve in benign ovarian cysts. Archives of Gynecology and Obstetrics, 287 (4), 729–732.
- Park, E.Y., et al., 2020. Epinephrine minimizes the use of bipolar coagulation and preserves ovarian reserve in laparoscopic ovarian cystectomy: a randomized controlled trial. Scientific Reports, 10 (1), 20911.
- Park, S.J., et al., 2020. Preservation of ovarian reserve and hemostasis during ovarian cystectomy: a randomised controlled trial. Journal of Minimally Invasive Gynecology, 27 (7), S62.
- Park, S.J., et al., 2021. A randomized controlled trial of ovarian reserve preservation and hemostasis during ovarian cystectomy. Scientific Reports, 11 (1), 8495.
- Peters, A., Rindos, N.B., and Lee, T., 2017. Hemostasis during ovarian cystectomy: systematic review of the impact of suturing versus surgical energy on ovarian function. Journal of Minimally Invasive Gynecology, 24 (2), 235–246.
- Poplawski, R. and Ma, K., 2022. Benign ovarian cysts in premenopausal women. Obstetrics, Gynaecology & Reproductive Medicine, 32 (10), 234–239.
- Ragni, G., et al., 2005. Damage to ovarian reserve associated with laparoscopic excision of endometriomas: a quantitative rather than a qualitative injury. American Journal of Obstetrics and Gynecology, 193 (6), 1908–1914.
- Sahin, C., et al., 2017. Which should be the preferred technique during laparoscopic ovarian cystectomy: hemostatic sutures or bipolar electrocoagulation? A randomized controlled prospective study of long-term ovarian reserve. Reproductive Sciences, 24 (3), 393–399.
- Shaltout, M.F., et al., 2019. A randomized controlled trial of a new technique for laparoscopic management of ovarian endometriosis preventing recurrence and keeping ovarian reserve. Journal of Ovarian Research, 12 (1), 66.
- Song, T., Lee, S.-H., and Kim, W.Y., 2014. Additional benefit of hemostatic sealant in preservation of ovarian reserve during laparoscopic ovarian cystectomy: a multi-center, randomized controlled trial. Human Reproduction, 29 (8), 1659–1665.
- Tanprasertkul, C., et al., 2014. Impact of hemostasis methods, electrocoagulation versus suture, in laparoscopic endometriotic cystectomy on the ovarian reserve: a randomized controlled trial. Journal of the Medical Association of Thailand, 97 (Suppl. 8), S95–S101.
- von Wolff, M., et al., 2019. Serum anti-Müllerian hormone concentration and follicle density throughout reproductive life and in different diseases—implications in fertility preservation. Human Reproduction, 34 (12), 2513–2522.
- von Wolff, M., et al., 2020. Serum anti-Mullerian hormone (AMH) concentration has limited prognostic value for density of primordial and primary follicles, questioning it as an accurate parameter for the ovarian reserve. Maturitas, 134, 34–40.
- Xiao, J., et al., 2019. Impact of hemostatic methods on ovarian reserve and fertility in laparoscopic ovarian cystectomy. Experimental and Therapeutic Medicine, 17 (4), 2689–2693.
- Yildiz, S., et al., 2020. The pain symptoms and mass recurrence rates after ovarian cystectomy or uni/bilateral oophorectomy procedures in patients over 40 years old with endometriosis. Ginekologia Polska, 91 (6), 295–300.
- Zhang, C.-H., Wu, L., and Li, P.-Q., 2016. Clinical study of the impact on ovarian reserve by different hemostasis methods in laparoscopic cystectomy for ovarian endometrioma. Taiwanese Journal of Obstetrics & Gynecology, 55 (4), 507–511.