

Abstract
Background
There is little information of progestogen-only contraceptives in patients with congenital heart disease (CHD) on the long-term.
Objective
To evaluate the use of contraception in patients with CHD. We studied both short-acting reversible contraceptives (SARCs), oral progestin-only pills (POPs) and long-acting reversible contraceptives (LARCs): intrauterine devices (IUD-IPs) and subdermal implants both impregnated with progestogens (SI-IPs).
Study design
Retrospective study of all women attending the preconception clinic. Contraceptive methods were classified in three TIERs of effectiveness before and after consultation. ESC classification regarding pregnancy risk, WHOMEC classification for combined oral contraceptive safety was collected.
Results
Six hundred and fifty-three patients. A significant proportion of them switched from TIER 3 to TIER 2 or 1 (p < .001) after consultation. One hundred and ninety-nine patients used POPs, 53 underwent IUD-IPs implantation and 36 SI-IPs, mean duration was 58 ± 8, 59 ± 8 and 53 ± 38 months, respectively.
Conclusions
Because of their safety and efficacy, IUD-IPs and SI-IPs should be considered as first-line contraception in patients with CHD.
Plain Language Summary
We looked at the use of progestogen-only contraceptives in women with congenital heart disease (CHD) over a long period and determine how safe and effective these contraceptives are for such patients. We considered two types of contraceptives: short-acting ones like progestin-only pills (POPs) and long-acting ones like intrauterine devices and subdermal implants that release progestogens.
We gathered information from 653 women and assessed how women’s contraceptive choices changed before and after they had a consultation with us.
After consulting with our clinic, a significant number of women switched from less effective contraceptives to more effective ones. Among the women who used POPs, most of them followed the prescribed regimen quite well. Additionally, 89 women used long-acting contraceptives, without failure of method.
In conclusion, our findings suggest that long-acting progestogen-only contraceptives are safe and effective choices for contraception in women with CHD. Therefore, these options should be considered as the first choice.
Introduction
Currently, the vast majority of people with congenital heart disease (CHD) reach adulthood (Marelli et al. Citation2014) and female patients consider contraception or maternity (Miner et al. Citation2017). Therefore, it is essential to offer them advice and safe options following clinical practice guidelines (Regitz-Zagrosek Citation2018).
Despite a 95% survival rate at 18 years, patients with repaired CHD often have significant residual lesions. Tetralogy of Fallot repair, the most common cyanotic CHD, involves surgical amplification of the right ventricular outflow tract. While pulmonary stenosis is eliminated, pulmonary valve regurgitation is a common consequence of the surgery, leading to progressive right ventricular dilatation that often necessitates further intervention.
Despite advances in treatment, some patients develop pulmonary arterial hypertension, and pregnancy is still associated with a 30% mortality rate. Repairs for all types of CHD, including univentricular physiology, involve several interventions to redirect flow directly from the inferior and superior vena cava to the pulmonary artery in the Fontan circulation system. Cyanosis is abolished, but long-term complications due to high central venous pressure persist, and despite treatment, there is a significant increased thrombotic risk. CHD cardiology is a full subspecialty where interaction with other medical specialties such as haematology, gynaecology, neurology and hepatology is crucial for providing healthcare to this young and challenging population. Cardio-obstetrics and gynaecologist teams are essential for providing care during the reproductive life of CHD patients. Risk of thromboembolism is already elevated in the CHD population. According to a study conducted in Sweden, the incidence of stroke was found to be 10 times higher in adults with CHD compared to the healthy population, and this trend was particularly notable among young patients (Giang et al. Citation2021).
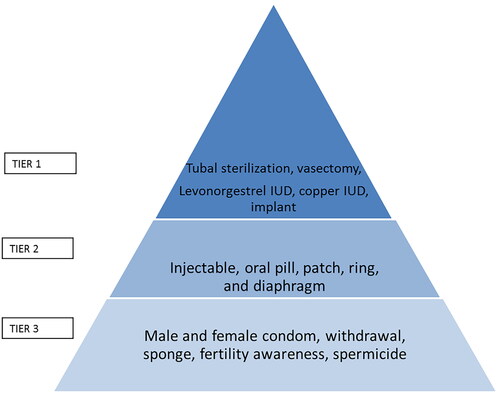
Nowadays, there is a great variety of contraceptive methods. Not only it is important to know their contraindications depending on the severity of the CHD, but also their efficacy (Pearl’s index) (Mansour et al. Citation2010), and the adherence to them. Long-acting reversible contraceptives (LARCs): LARCs are considered TIER 1 (failure rate <1%); and short-acting reversible contraceptives (SARCs) TIER 2 (failure rate 6–12%). Finally, experts discourage TIER 3 methods (failure rate 18–28%), considering their efficacy is too low efficacy for patients at high risk. shows type of contraception classified by efficacy. In patients with a severe CHD, a failure in the contraceptive method with subsequent pregnancy constitutes a risk to the life of the woman (Bédard et al. Citation2009, Roos-Hesselink et al. Citation2015); therefore, methods with high risk of failure should be discouraged. Pregnancy and heart disease guidelines (Regitz-Zagrosek Citation2018) classify CHD and AHD depending on their risk of maternal and foetal complications during pregnancy in five categories. The majority of patients are at high risk if pregnancy (modified European Society of Cardiology, ESC3) or contraindication for pregnancy (ESC4) has significant risk of thrombosis and thus contraindication for combined hormonal contraception (CHC).
Figure 1. Type of contraception classified by efficacy.
Experts advise to use LARCs and SARCs progesterone-only containing, progesterone-only pills (POPs) in CHD patients, especially if classified as World Health Organization Medical Eligibility Contraception (WHOMEC) grade 3 or 4 for the use of CHCs (Anon Citation2015). However, there is scarce information on the safety of LARCs and SARCs, and on the adherence to them in the CHD population. Moreover, the WHOMEC indications on the risks of CHCs do not consider many repaired CHDs patients, as patients with repaired Tetralogy of Fallot or Transposition of Great Arteries.
In our centre, we have established a Multidisciplinary Gynaecology-Cardiology Consultation (MGCC) aimed at providing comprehensive reproductive advice to CHD patients. This consultation involves both cardiologists and gynaecologists and is offered to all patients undergoing CHD clinic follow-up. We already published initial data on progestogen-containing contraceptives in patients with CHD (Pijuan-Domènech et al. Citation2013). However, no data are available on their long-term safety and efficacy. In this context, the objectives of this study were to evaluate the following aspects in patients with CHD. This study aims to:
evaluate the safety, efficacy and adherence to progesterone-containing contraceptive methods recommended after an MGCC consultation, including intrauterine devices impregnated with progestogens (IUD-IPs) and subdermal implants impregnated with progestogens (SI-IPs).
assess gynaecological and cardiological adverse events associated with SARCs like progestin-only pills (POPs).
In this context, the objectives of this study were to evaluate the following aspects in patients with CHD: (1) the safety, efficacy and therapeutic adherence to the contraceptive method indicated after a multidisciplinary counselling visit; (2) the gynaecological and cardiological adverse events attributable to the use of SARCs, such as POPs; and (3) the gynaecological and cardiological adverse events attributable to the use of LARCs, such as IUD-IPs and SI-IPs.
Materials and methods
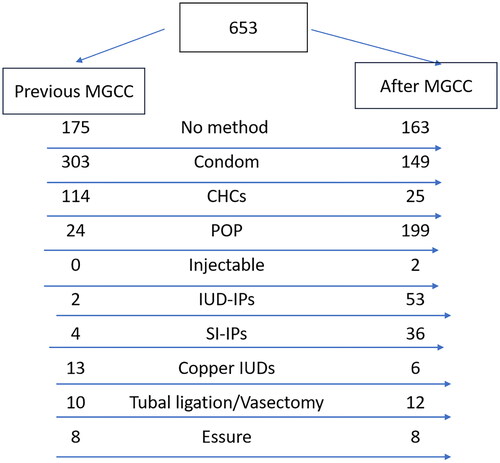
In a retrospective study from January 2007 to December 2019, all women of childbearing age attending the Adolescent and Adult CHD Unit with the World Health Organization for risk of complications if pregnant (ESC > 2–3) were invited to attend the preconception clinic during their routine cardiology follow-up. Patients with low risk of complications if pregnant but contraindication for CHC due to CHD (as per atrial septal defect) were also invited if contraception was required (STROBE) shows flow of patients. The Ethics Committee of the Hospital accepted the review of the data (Number of Ethics Committee PR(MI)190/2010). The requirement for consent was waived by the Ethics Committee due to the retrospective nature of the study and anonymisation of the data.
Figure 2. STROBE: diagram of flow patients.
The WHOMEC classification for the risk of CHCs considers patients in group 4 as having formal contraindication, and group 3 as having relative contraindication. This classification does not include many repaired CHDs, so it could be deduced that it is safe to use CHCs in these patients. However, considering previously published information (Pijuan-Domènech et al. Citation2013) we included the following patients in group WHOMEC 3: those with significant mitral regurgitation (MR), those with repaired CHD and significant residual right valve disease (pulmonary regurgitation (PR) or tricuspid regurgitation (TR)); patients with TGA and atrial switch repair, or TGA and arterial switch repair, or coronary anomaly with previous surgery that included coronary reimplantation; and patients carrying endocavitary pacemakers or implantable cardioverter defibrillator (ICD). We also considered patients with moderate or severe aortic stenosis included WHOMEC3 as with some risk of atrial fibrillation. Finally, we considered patients with moderate or severe mitral stenosis were included in group WHOMEC 4 due to high risk of thrombosis.
Clinical variables were collected: age, type of CHD, BMI, presence of other cardiovascular risk factors. Clinical factors with special relevance in terms of contraception were also collected: presence of pacemaker or ICD, presence of chronic cyanosis; chronic anticoagulation; residual left-to-right shunt; presence of a mechanical valve; pulmonary hypertension; WHOMEC Risk Classification of CHCs (Thorne et al. Citation2006) and also modified by us WHOMEC Risk Classification for the use of CHCs. Specifically, the presence of residual left-to-right shunt was assessed from the most recent echocardiogram. Finally, current and past contraceptive methods and duration of the treatment were recorded. Secondary effects were reported by patients that started POPs at successive in-person visits. Specifically, throughout the follow-up period, they were consistently questioned about occurrences such as amenorrhoea, spotting, new cardiovascular events, including stroke and transient ischaemic attack (TIA), myocardial infarction and endocarditis. Death or cardiac transplantation was also registered.
Cervical cytology tests were performed following clinical recommendations. Results were considered as following: HPV+: human papilloma virus positive; ASCUS: atypical squamous cells of undetermined significance; LSIL: low-grade squamous intraepithelial lesion; HSIL: high-grade squamous intraepithelial lesion.
Transvaginal ultrasound exams were performed during follow-up.
Patients were classified in different categories on the basis of the contraceptive method used: (1) TIER 1 (failure rate <1%), including LARCs (IUD-IPs Mirena® and Kyleena®, Implanon® and copper-bearing IUD) and definitive methods (Essure®, tubal ligation, and vasectomy); (2) TIER 2 (failure rate 6–12%), including SARCs (POPs, CHCs, combined contraceptives in patch, vaginal ring and injectables depot (Depo-Provera®)); and (3) TIER 3 (failure rate 18–28%), including condoms, fertile days technique and spermicides. Experts discourage TIER 3 methods (failure rate 18–28%), considering their efficacy is too low for patients at high risk (Lindley et al. Citation2021).
Data were analysed using R version 4.1 (R Foundation for Statistical Computing, Vienna, Austria). Means and ranges are presented for continuous variables, and counts and percentages for nominal variables. Differences between groups were assessed using Kruskal–Wallis tests in case of continuous variables and Chi-square tests for categorical variables. In the case of short-term and adverse effects, differences between groups were assessed using Fisher’s tests. Effect of contraceptives in outcomes was compared to control group using logistic linear regression, and results are reported as odds ratio (OR) (with 95% confidence intervals).
Results
A total of 653 women were assisted at our MGCC from 2007 to 2019, all of whom were included in the study. Eleven patients were lost to follow-up, as they changed their location. The main characteristics of the patients are listed in . The commonest types of CHD are presented in Supplemental Table 1S.
Table 1. Baseline and demographic characteristics of the patients included in the study.
Before the visit, 26.8% of the patients did not use a contraceptive method, while 46.4% used a TIER 3 method, 21.0% a TIER 2 and 5.8% a TIER 1. We provide appropriate contraception to all patients, emphasising that TIER 2 and especially TIER 1 are more recommendable than TIER 3 methods. Following evaluation and subsequent follow-ups, the distribution shifted, with 25.0% of the patients not using any method, 22.8% using a TIER 3 method, 34.6% a TIER 2 method and 17.6% a TIER 1. These changes were statistically significant (p < .001).
During the follow-up, seven patients experienced TIAs: two while using LARCs, and five while not receiving contraceptive treatment. We conducted a comparative OR analysis between the groups, and no significant difference was observed (p = .516).
Only one patient with an IUD-IP and a history of coronary artery disease experienced acute coronary syndrome, which was not attributed to the IUD-PI. Endocarditis was observed in two patients using POPs, but notably, they were not using any type of implant.
Sixteen patients were reported to have died or undergone transplantation during the follow-up, which was expected due to their CHD. Cardiac transplantation was more frequent among patients with PI-IP (p = .013).
illustrates cardiovascular complications observed during follow-up in the no-treatment group, the POP group, the IUD-PI group and the IP-PI group, along with their respective comparison.
Table 2. Cardiovascular complications in each group of patients during follow-up.
Gynaecological side effects were categorised as short-term (first three months) and long term (after three months).
Patients treated with POPs
Patients who initiated treatment with POPs after their MGCC visit exhibited demographic and clinical characteristics similar to those of the overall study population, mean age 27.3 ± 7.5 and BMI 23.5 ± 7.5; p = .264), see . Out of the patient cohort, 199 individuals began treatment with POPs. The mean duration of POPs treatment was 58 months (±8), with a median of 31 months. This duration ranged from 9 to 148 months.
A significant percentage of patients reported secondary effects associated with POPs, the most frequent being amenorrhoea (42.7%). displays the reported long-term secondary effects associated to progestogen only contraception methods and comparison between the three groups. At the time of prescribing the drug, patients were warned of this effect, even if not having harmful consequences for health. A total of 46 patients (23%) discontinued POPs during first 3 months of follow-up. The most frequent motivations for discontinuation of POPs were personal reasons (62.0%) or secondary effects (12.0%), mostly spotting, followed by liquid retention, headache, vaginal dryness, laboratory abnormalities and mastodynia.
Table 3. Long-term side effects related to progestin-only contraception.
In our analysis, we did not observe any statistically significant differences (p = NS) when comparing the results of the cervical cytology test among different groups. Additionally, no statistically significant differences were found, even in the presence of functional cysts. Analytical parameters related to lipids also did not show any alterations that reached statistical significance (p = NS).
Throughout the follow-up, the frequency of pregnancies among patients taking POPs was low, being Pearl’s index 0.0045. Comparison with other LARCs method did not reach statistical significance (p = .435).
Patients with an IUD-IP implant
A total of 53 patients (mean age of 33.9 ± 6.5 years and BMI of 23.1 ± 3.5) underwent an IUD-IP implantation (69 IUD-IPs were implanted) with a mean duration of 59 ± 8 months, including patients with more than one IUD-IP. Their characteristics are detailed in . A substantial proportion of these patients received anticoagulant treatment. Significantly more patients in this group received anticoagulant treatment compared to the global population of the study (34.0% vs. 13%, p < .001), as indicated in .
Prior to the insertion of IUD-IP, a cervical cytology test was performed to rule out asymptomatic underlying infection. We used endocarditis prophylaxis only during first year of the series. Most patients (85.5%) underwent IUD-IP insertion without sedation. shows short-term complications during IUD-IP insertion, considering each individual IUD-IP insertion. During insertion, 2.9% insertions were accompanied by vagal reaction with symptomatic hypotension that recovered with simple Trendelenburg’s position but without syncope (one patient with TGA and one patient with TOF, both with IUD-IP Mirena®). We have determined that patients with conditions such as severe aortic stenosis, pulmonary arterial hypertension or those with ICDs require sedation at the time of insertion to prevent life-threatening syncope and ensure their safety.
Table 4. Short-term (3 months) side effects during IP-IUD and PI-IP insertion.
As IUD-IPs is an invasive method with prosthetic material, we considered bacterial endocarditis (BE) risk in the high-risk population of CHD. We did not observe any episode of endocarditis after the application of IUD-IPs. No IUD-IP migration, pelvic inflammatory disease or uterine perforation was observed during the follow-up. Secondary effects were reported in 43% of the patients with IUD-IPs, the most frequent being amenorrhoea (35.8%) (see ). At the time of insertion, patients were warned of this effect, even if not having harmful consequences for health; however, nobody considered it a reason for withdrawal. Other secondary effects were spotting during the first months (13.2%) and hypermenorrhea (1.9%). Of the patients with IUD-IPs, 79.0% maintained the method. No short-term withdrawal was observed (during first three months). A total of 11 patients (21.0%) withdrew it prior to complete 60-month duration. Notable reasons for withdrawal included device expulsion (7.5%) and recurrent vaginal infection (3.8%).
No significant differences were observed in the results of the cytology test. However, the presence of simple follicles was higher than in the POPs and non-treated group, as observed by ultrasound (p < .001).
Patients with an SI-IP implant
A total of 36 patients received SI-IPs (49 SI-IPs were implanted). The mean age was 26.3 ± 7.4 years, significantly lower than the rest of the groups (p < .01), and the BMI was 23.7 ± 5.2. The mean duration of the treatment was 53 ± 38 months.
In comparison with the overall population, a significantly higher percentage of these patients (19.4%) received antiplatelet treatment (p < .001), indicating a higher proportion of patients with Fontan’s circulation. To initially observe the response to progestogens, most patients (72.0%) received treatment with POPs prior to implantation. The mean duration of the treatment with POPs before SI-IPs was 18 ± 2.4 months, depending on the presence of liver disease related to Fontan’s circulation, and on the doubts about therapeutic adherence.
Secondary effects during long-term follow-up for SI-IPs are indicated in . All implants could be removed without complications, and no cases of migration or infection occurred. shows short-term complications during SI-PI insertion. A total of six patients (12.2%) of the implants, had their implants withdrawn early. The primary reasons of withdrawal were spotting (in 9.0% of the cases), and the desire for pregnancy (in the rest of the cases). There was no vagal reaction, syncope or sedation requirement. Lastly, no pregnancies were reported during follow-up.
Discussion
This is the first study that provides data on the safety and efficacy of progestogen-containing contraceptives, both SARCs and LARCs, in the long term, in patients with CHD.
The secondary effect most frequently reported by patients under treatment with either POPs, IUD-IPs or SI-IPs was irregular bleeding. Considering the high percentage of patients receiving antiplatelets or anticoagulants, this was the main reason for abandonment of POPs. Other series in patients without heart disease under treatment with POPs showed a considerable spotting rate (Palacios et al. Citation2020). This is the main limitation of their use, although it is sometimes possible to control bleeding by transiently doubling the dose. In most patients, spotting occurs at the beginning and subsequently disappears. Among patients with SI-IPs, we found an incidence of spotting and hypermenorrhea comparable to what reported in the meta-analysis by Moray et al. (Citation2021). Among patients with IUD-IPs, the rate of hypermenorrhea was lower than in patients treated with POPs (albeit statistically not significant), not being a reason for withdrawal in any case, despite the higher incidence of chronic anticoagulation.
Pearl’s index in patients treated with SARCs was 0.0045, which is lower than what previously reported for SARCs (Lindley et al. Citation2021) but higher than for LARCs, still not statistically significant. Therefore, to minimise the risk of pregnancy authors postulate that it is essential for patients with CHD to use LARCs.
The SI-IPs abandonment rate was 13.0% in a 3-year follow-up, much lower than previously reported (Runyan et al. Citation2021). First, the initiation of POPs before implantation may have played a pivotal role in enhancing patient adherence and reducing abandonment. Additionally, we implemented a strategy of temporarily administering oral progestogens in cases of spotting, which is in line with the approach described by Moray et al. (Citation2021). This proactive management of side effects likely contributed to the overall lower dropout rate in our patient population. The expulsion rate of the IUD-IP was 7.5%, with a mean follow-up of 59 months, similar to previously reported (Cox M et al. Citation2002).
No significant differences were observed in the results of the cervical cytology test and cytological alterations (ASCUS, LSIL, HSIL, carcinomas, etc.) between the different groups. Moreover, the percentage of positive results of the HPV test for high-risk viruses among non-treated CHD patients in our study was 4.4%, lower than in the general population (17.0%). This suggests that patients with heart disease better protect themselves by using a barrier method (Fry et al. Citation2015). However, more reversible benign lesions (ovarian cysts) were observed in patients treated with IUD-IPs and SI-IPs, in comparison to patients treated with POPs and non-treated population. Therefore, for the former, we suggest ultrasound and clinical follow-up.
Regarding the cardiovascular side effects in the CHD population, no episode of endocarditis occurred after IUD-IP insertion. Bacterial endocarditis prophylaxis was only performed before IUD-IP insertion in the first cases of the series, since BE guidelines had not been modified yet. Posteriorly due to chance in BE guidelines and the scarce documentation of episodes of BE connected to IUD insertion in the literature (Habib et al. Citation2015, Meyerowitz et al. Citation2019), no BE prophylaxis was performed. During the insertion of the IUD-IP, we consider it essential to avoid vagal reaction, especially syncopal, so the threshold for the use of sedation is low between CHD patients.
Finally, regarding myocardial infarction stroke or AIT, only a coronary acute syndrome was observed in a patient with already coronary heart disease. No significant increase of TIA was observed compared to our patient population without treatment. Embolic and thromboembolic phenomena increase with the use of CHC, especially in the presence of obesity and hypertension. Data on the association of use of CHCs with embolic and thromboembolic phenomena are not specifically available for patients with CHD; however, the WHOMEC classification advises against the use of CHCs for some of these patients, despite few information about safety in CHD population. Although more long-term follow-up is required, in our study, the incidence of stroke was not higher in women treated with progestogen contraceptive than in untreated ones. We observed significantly more requirement of cardiac transplantation between patients with SI-IP implants, according to patient population higher risk profile (i.e. more Fontan circulation patients).
The recent review by Abarbanell et al. (Citation2019) evaluated multiple studies and revealed a scarcity of robust evidence, indicating poor quality, regarding contraceptive safety in women with CHD. While several published guidelines and expert reviews exist, offering insights into the theoretical risks associated with contraceptive methods in women with specific types of CHD, the available evidence remains limited.
Collaboration and open communication between a woman’s cardiologist and her contraceptive provider could significantly enhance the quality of counselling. This joint approach facilitates a more comprehensive discussion regarding the potential risks and benefits of various contraceptive methods, allowing for a comparison with the risks associated with unintended pregnancy.
According to a recent review, oral progesterone methods do not pose cardiological contraindications. However, due to the POP’s reduced efficacy without perfect use, it is not recommended for patients with ESC3 or ESC4 classifications, wherein pregnancy is contraindicated. For these patients, the primary focus should be on counselling about high-efficacy methods, such as LARCs.
The IUD-PI stands as a preferred method for many patients due to its high efficacy. However, caution is advised, particularly for high-risk individuals, such as those with conditions like pulmonary hypertension, where the absence of sedation during implantation could potentially trigger a serious cardiac event due to a vasovagal reaction. Research by Trinh et al. (Citation2023) suggests that vasovagal reactions occur in up to 5% of women following cervical manipulation during IUD placement.
Our study represents the largest single-centre series with the most extended follow-up duration published to date. Despite current guideline recommendations, until now there was a notable absence of published information regarding the long-term safety and outcomes of use of progestogen-only contraception.
This is a retrospective study, and the series belongs to a third-level CHD unit in adolescents and adults, that include patients with very complex CHD who undergo exhaustive follow-up. However, our results would be applicable to similar tertiary CHD patient populations. CHD cardiologists, both paediatrics and adults are aware of the importance of preconceptional counselling and contraception, so active referral to preconceptional clinic is performed. These findings further support AHA (American Heart Association) recommendations to coordinate efforts between cardiologists and obstetrics and gynaecologist providers to improve knowledge, access and utilisation of effective contraceptive methods early and often for women with CHD who wish to avoid pregnancy (Warnes et al. Citation2008, Cannobio et al. Citation2017).
Conclusions
Our results show that multidisciplinary consultations for contraceptive and reproductive advice allow safe contraception with a low pregnancy rate in patients with CHD. Contraceptive methods are better adjusted to the guidelines after consultation, with a higher rate of patients in the TIER 1 group. Because of their safety, efficacy and adherence, and of the few complications associated with their application, LARCs specifically IUD-IPs and SI-IPs, should be considered first-line methods in patients with CHD. Future studies evaluating contraceptive safety among women with CHD would help quantify the risks, beyond that of the general population.
Author contributions
FB and AP designed the project, and wrote the manuscript; MG and LDS supervised the work, performed data acquisition. BM, LP and ES performed data analysis and IF and EC interpretation of results and direction of the work. All the authors read and approved the manuscript.
Supplemental Material
Download MS Word (22.6 KB)Acknowledgements
The authors thank Valeria Di Giacomo from ThePaperMill for the English version of the document and Claudia Alvarez for the statistical support.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data regarding any of the subjects in the study have not been previously published unless specified. Data will be made available to the editors of the journal for review or query upon request.
Additional information
Funding
References
- Abarbanell, G., et al., 2019. Safety of contraceptive use among women with congenital heart disease: a systematic review. Congenital Heart Disease, 14 (3), 1–8.
- Anon, et al., 2015. WHO guidelines approved by the guidelines review committee. Medical eligibility criteria for contraceptive use. Geneva: World Health Organization.
- Bédard, E., Dimopoulos, K., and Gatzoulis, M.A., 2009. Has there been any progress made on pregnancy outcomes among women with pulmonary arterial hypertension? European Heart Journal, 30 (3), 256–265.
- Cannobio, M., et al., 2017. Management of pregnancy in patients with complex congenital heart disease: a scientific statement for healthcare professionals from the American Heart Association. Circulation, 135, e50–e87.
- Cox, M., et al., 2002. Clinical performance of the levonorgestrel intrauterine system in routine use by the UK Family Planning and Reproductive Health Research Network: 5-year report. Journal of Family Planning and Reproductive Health Care, 28 (2), 73–77.
- Fry, K.M., et al., 2015. Lifetime prevalence of sexual intercourse and contraception use at last sex among adolescents and young adults with congenital heart disease. Journal of Adolescent Health, 56 (4), 396–401.
- Giang, K.W., et al., 2021. Burden of ischemic stroke in patients with congenital heart disease: a nationwide, case-control study. Journal of the American Heart Association, 10 (13), e020939.
- Habib, G., et al., 2015. ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European Heart Journal, 36 (44), 3075–3128.
- Lindley, K., et al., 2021. Contraception and reproductive planning for women with cardiovascular. Journal of the American College of Cardiology, 77 (14), 1823–1834.
- Mansour, D., et al., 2010. Efficacy of contraceptive methods: a review of the literature. European Journal of Contraception & Reproductive Health Care, 15 (1), 4–16.
- Marelli, A.J., et al., 2014. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation, 130 (9), 749–756.
- Meyerowitz, E.A., et al., 2019. Endocarditis following IUD insertion in a patient with tetralogy of Fallot. BMJ Case Reports, 12 (2), e227962.
- Miner, P., et al., 2017. Contraceptive practices of women with complex congenital heart disease. American Journal of Cardiology, 119 (6), 911–915.
- Moray, K.V., et al., 2021. A systematic review on clinical effectiveness, side-effect profile and meta-analysis on continuation rate of etonogestrel contraceptive implant. Reproductive Health, 18 (1), 4.
- Palacios, S., et al., 2020. Bleeding profile of women using a drospirenone-only pill 4 mg over nine cycles in comparison with desogestrel 0.075 mg. PLOS One, 15 (6), e02318.
- Pijuan-Domènech, A., et al., 2013. Usefulness of progesterone-only components for contraception in patients with congenital heart disease. American Journal of Cardiology, 112 (4), 590–593.
- Regitz-Zagrosek, V., 2018. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. European Heart Journal, 39 (35), 3241–3269.
- Roos-Hesselink, J.W., et al., 2015. Contraception and cardiovascular disease. European Heart Journal, 36 (27), 1728–1734.
- Runyan, L., et al., 2021. Acting reversible contraception: placement continuation, and removal rates at an inner-city academic medical center clinic. Journal of Clinical Medicine, 10 (9), 1918.
- Thorne, S., et al., 2006. Risks of contraception and pregnancy in heart disease. Heart (British Cardiac Society), 92 (10), 1520–1525.
- Trinh, A., et al., 2023. Contraception and cardiovascular effects: what should the cardiologist know? Current Cardiology Reports, 25 (11), 1489–1498.
- Warnes, C.A., et al., 2008. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Circulation, 118, e714–e833.