

Abstract
Background
Selection of high-quality blastocysts is the most important factor determining the success of assisted reproductive technology. The objective of this study is to assess the values of blastocyst morphological quality and development speed for predicting euploidy and clinical pregnancy outcome.
Methods
A total of 155 preimplantation genetic testing cycles including 959 blastocysts and 154 euploid blastocyst transfer cycles conducted between January 2018 and December 2019 were retrospectively analysed. The associations of blastocyst morphological quality and development speed (D) with chromosomal status, clinical pregnancy rate, early miscarriage rate, and ongoing pregnancy rate were evaluated by univariate and multivariate regression.
Results
The euploidy rate of development speed D5 blastocysts was significantly greater than that of D6 blastocysts (61.4% vs. 38.1%, P < 0.001), and the euploid rate of morphologically high-grade blastocysts was significantly greater than that of non-high-grade blastocysts. Development speed D5 (OR = 1.6, 95% CI 1.2–2.2, P = 0.02) and high-grade morphology (OR = 2.1, 95% CI 1.5–2.9, P = 0.01) were independent predictors of euploidy. The ongoing pregnancy rate of D5 blastocysts was significantly higher than that of D6 blastocysts (62.3% vs. 43.8%, P = 0.04). Transfer of euploid blastocysts with high-grade morphology resulted in a greater ongoing pregnancy rate than transfer of non-high-grade euploid blastocysts (60.7% vs. 43.2%, P = 0.049). Alternatively, D6 development speed was an independent risk factor for early pregnancy loss after euploid blastocyst transfer. Multivariate regression analysis adjusting for confounding factors identified maternal age, blastocyst development speed, and blastocyst morphological grade as independent predictors of euploidy but not of clinical pregnancy.
Conclusion
The recommended sequence of embryo transfer based on the present study is D5 high-grade > D6 high-grade > D5 non-high-grade > D6 non-high-grade.
PLAIN LANGUAGE SUMMARY
Assisted reproductive technology physicians are actively exploring methods to improve the accuracy of embryo selection for successful pregnancy. We evaluated the associations of embryo morphological grade and development speed with chromosomal status and clinical outcome for couples without a history of infertility, in vitro fertilisation failure, or recurrent miscarriage receiving euploid embryo transfer. Blastocysts from females younger than 35 years, of high morphological grade, and demonstrating faster development speed were most likely to be euploid (least likely to have chromosomal abnormalities). Alternatively, patients implanted with slower developing euploid blastocysts were at higher risk of early pregnancy loss. To maximise the probability of implanting euploid embryos and minimise the risk of pregnancy loss, the selection order of embryo transferred should be based on embryo development speed followed by morphological grades.
Introduction
Embryo quality is undoubtedly the most critical factor influencing the success of in vitro fertilisation-embryo transfer (IVF-ET), so improved embryo selection is essential for increasing the probability of delivering a healthy baby. However, there are no consensus criteria for optimal embryo selection. For many years, assisted reproductive technology (ART) physicians have been actively exploring methods to improve the accuracy of embryo selection, including blastocyst culture, time-lapse imaging of embryo morphodynamics for euploidy prediction (Bamford et al. Citation2022), and preimplantation genetic testing (PGT) (Rocha et al. Citation2016). While simple, selection based on classic embryo morphology scoring is of insufficient accuracy for predicting the take-home-baby rate (Rocha et al. Citation2016).
Fluorescence in situ hybridisation (FISH)-based preimplantation genetic screening (PGS) studies have reported that the development speed of cleavage-stage embryos is associated with the risk of genetic abnormalities (Kaing et al. Citation2018, Kim et al. Citation2019). Alfarawati et al. (Citation2011) also found a weak association between aneuploidy and blastocyst morphology. However, cases were limited and the methods of embryo culture and biopsy were not optimal for detecting euploid embryos. A large-scale multi-centre retrospective study by Capalbo et al. (Citation2014) also found a moderate relationship between blastocyst morphology and embryo euploidy. However, the study subjects were of advanced maternal age and (or) had a history of recurrent unsuccessful IVF treatments or previous spontaneous abortion, limiting applicability of the results to the general IVF-ET candidate population. Therefore, the accuracy of euploid embryo selection based on conventional parameters is still unsatisfactory. Moreover, data from couples without infertility have not been reported.
Therefore, the current study was designed to evaluate the associations of morphological grade and development speed with chromosomal status and clinical pregnancy outcomes of euploid embryo transfer among couples without a history of infertility, IVF failure, or recurrent miscarriage.
Materials and methods
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital, Sun Yat-sen University (ethical approval number: 2019[131]). All participants provided written informed consent. A total of 155 PGT cycles including 959 blastocysts biopsied for mono-genetic diseases and 154 frozen–thaw euploid embryo transfer cycles conducted at a single IVF centre between January 2018 and December 2019 were retrospectively analysed. The inclusion criteria were as follows: (i) women without a history of infertility and no obvious infertility factors, (ii) couples without chromosomal abnormalities, and (iii) PGT for aneuploidy (PGT-A) required due to a mono-genetic disease diagnosed in one or both partners. There was no restriction on age or ovulation stimulation protocol. Exclusion criteria included a history of infertility and clear infertility factors, recurrent (2 or more) spontaneous abortions, and recurrent implantation failure.
Laboratory procedures
Controlled ovarian stimulation, oocyte collection, and embryo biopsy were performed as previously described (Luo et al. Citation2017). Biopsied trophectoderm (TE) cell samples were subjected to whole genome analysis (WGA) using the Qiagen Single Cell Amplification Kit (Qiagen, Germantown, MD, USA). Chromosomal abnormalities, including aneuploidy and unbalanced segment anomalies, were detected in amplification products using the Illumina Human CytoSNP12 microarray (Illumina, Inc., San Diego, CA, USA).
Blastocyst development speed and grading
Blastocysts were observed on the 5th and 6th days after fertilisation and divided into D5 and D6 groups according to the time of blastulation (on the 5th day or 6th day post-fertilisation, respectively). Modified Gardner and Schoolcraft grading was used to assess developing blastocysts (Gardner Dk Citation1999), and morphology was categorised prior to cryopreservation according to the method of Capalbo et al. (Citation2014) as follows: high-grade (3AA–6AA, 4AB–6AB, 4BA–6BA, and 4BB–6BB), medium-grade (3BB, 3AB, 3BA), and low-grade (< 3BB, ICM and/or TE grade C).
Frozen embryo transfer and follow-up
Endometrial preparation and transfer were performed as previously described (Luo et al. Citation2017). Clinical pregnancy was defined as the presence of a gestational sac at Week 6–7, early miscarriage as pregnancy loss between Week 6 and Week 13, and ongoing pregnancy rate as number of foetuses with heart activity beyond 14 weeks of gestation per transferred cycle.
Main outcome measurements
The following associations were analysed: (1) Euploidy rates of D5 and D6 blastocysts; (2) Euploidy rates of blastocysts with low, medium, and high morphological grades; (3) Euploidy rates of blastocysts graded by combined development speed and morphological quality; (4) Values of maternal age, blastocyst development speed, and blastocyst morphological quality for predicting euploidy. The following correlations with pregnancy outcome were also analysed for transferred euploid blastocysts: (1) Clinical pregnancy rate and ongoing pregnancy rate of D5 and D6 euploid blastocysts; (2) Clinical pregnancy rate and ongoing pregnancy rate of low, medium, and high morphological grade euploid blastocysts; (3) Values of development speed and morphological quality grade for predicting clinical pregnancy outcomes.
Statistical methods
Continuous variables with normal distributions are expressed as mean ± standard deviation (SD) and compared by independent samples t-test, while continuous variables not conforming to a normal distribution are expressed as median (25% percentile, 75% percentile) and compared by Wilcoxon rank sum test and Kruskal-Wallis test. Multivariate analysis was performed by binary logistic regression to identify independent predictors of euploidy and clinical outcome. All statistical analyses were conducted using IBM SPSS 25.0, and a P < 0.05 was considered statistically significant for all tests.
Results
A total of 2715 oocytes were obtained, yielding 1855 2pn embryos and 1970 Day 3 embryos (). In total, 987 blastocysts were available for biopsy, and chromosomal analysis results were obtained for 959 (97.1%). The clinicodemographic characteristics of patients with oocyte retrieval are summarised in . A total of 154 PGT-M cycles with frozen-thawed euploid embryo transfer were included in the analysis. The clinicodemographic characteristics of all patients receiving euploid embryo transfer are shown in .
Figure 1. Study flowchart.
PGT, preimplantation genetic testing.
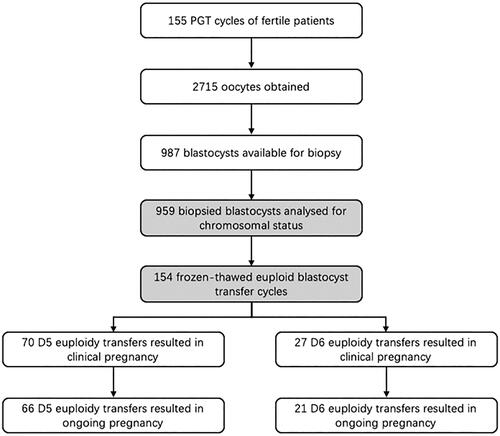
Table 1. Clinicodemographic characteristics of patients with oocyte retrieval.
Table 2. Clinicodemographic characteristics of patients receiving blastocyst transfer.
Associations of embryo morphological grade and developmental speed with euploid rate
Euploid rates were first compared between the 516 D5 blastocysts and 443 D6 blastocysts (See in Supplementary Figure S1). There was no significant difference in age between D5 and D6 patients (mean of 31.7 years vs. 31.9 years), while the euploid rate of D5 blastocysts was significantly greater than that of D6 blastocysts (61.4% vs. 38.1%, P < 0.01). Euploid rates were also compared among embryos of different morphological grades (See in Supplementary Figure S2). Again, there were no significant differences in age among groups with low-, medium-, and high-grade blastocysts (31.6, 32.0, and 32.6 years, respectively), but the euploid rate increased significantly with higher morphological grade (36.8% vs. 48.1% vs. 62.4%, P < 0.01).
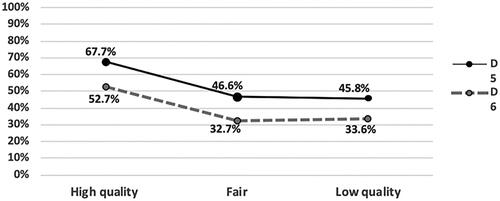
We then examined euploid rates among blastocysts graded by combined development speed and morphological grade (). Euploid rate was greater for high-quality blastocysts of either D5 or D6 development speed compared to non-high-quality D5 or D6 blastocysts, while there was no difference in mean patient age. In contrast, there was no significant difference in the euploid rate between medium- and low-grade groups. The rank order of euploid rates was as follows: D5 high-grade (68%) > D6 high-grade (53%) > D5 non-high-grade (47%) > D6 non-high-grade (33%). Multivariate regression analysis revealed that female age, blastocyst development speed (D5/D6), and morphological grade were independent predictors of blastocyst euploidy. The probability of euploidy was significantly higher in blastocysts from females younger than 35 years (OR2.3, 95% CI:1.1–3.1, P = 0.015), of high morphological grade (OR2.1, 95% CI:1.5–2.9, P = 0.01), and of D5 development speed (OR1.6, 95% CI:1.2–2.2, P = 0.02).
Figure 2. Euploidy rate according to blastocyst development speed and morphology grade.
Associations of embryo morphological grade and development speed with pregnancy outcomes
The clinical outcomes of 154 euploid blastocyst transfer cycles were then analysed for associations with blastocyst development speed and morphological grade (). The mean age of patients implanted with euploid blastocysts was 30.7 years, the overall clinical pregnancy rate was 63.0%, and the overall ongoing pregnancy rate was 56.5%. Clinical pregnancy rate did not differ significantly between patients receiving D5 or D6 euploid blastocysts (66.0% vs. 56.3%), but the ongoing pregnancy rate was higher following transfer of D5 euploid blastocysts compared to D6 euploid blastocysts (62.3% vs. 43.8%, P = 0.04). Similarly, clinical pregnancy rate also did not differ between high-grade and non-high-grade blastocysts (66.7% vs. 51.4%, P = 0.078), but ongoing pregnancy rate was significantly higher after implantation of high-grade blastocysts compared to non-high-grade blastocysts (60.7% vs. 43.2%, P = 0.049). For successful implantation, the rank order of selection was D5 high-grade (69.3%) > D6 high-grade (58.6%) > D6 non-high-grade (52.6%) ≈ D5 non-high-grade (50.0%) (). Thus, D5 euploid blastocysts of high-grade morphology were significantly more likely to be implanted than other types (P = 0.024). Similarly, the rank order for ongoing pregnancy was D5 high-grade (65.9%) > D6 high-grade (44.8%) ≈ D5 non-high-grade (44.4%) ≈ D6 non-high-grade (42.1%). According to multivariate regression analysis assuming that all blastocysts were euploid, female age, D5 or D6 development speed, and morphological grade were not independent predictors of clinical pregnancy, but D6 development speed was an independent risk factor for early pregnancy loss (OR 2.1, 95% CI:1.02–4.1, P = 0.046). Moreover, neither female age nor morphological grade effectively predicted ongoing pregnancy.
Figure 3. Associations of developmental speed and morphological grade with pregnancy outcome after euploid blastocyst transfer.
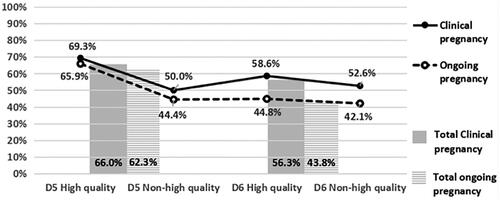
Table 3. Comparison of pregnancy outcomes between D5 and D6 euploidy transfers with different morphological grades.
Discussion
Appropriate embryo selection is essential for further improving IVF efficiency. An ideal system of embryo selection should have the following characteristics: high accuracy, relatively simple application, and little effect on individual embryos (Rocha et al. Citation2016). Embryo morphology grade is currently the most widely used evaluation method in clinical practice (Rocha et al. Citation2016) due to simplicity of application using a conventional light microscope. In addition, Arce et al. (Citation2006) reported satisfactory inter- and intra-observer agreement for the main embryo quality morphological parameters. Nonetheless, morphological grading is still subjective and likely to limit achievable observer agreement.
Appearance alone may be insufficient to judge the probability of successful implantation and full-term pregnancy. In fact, these outcomes are more strongly related to genetic status, especially euploidy (Coonen et al. Citation2020). On the other hand, the embryo must be structurally and functionally normal to interact effectively with the endometrium for implantation and to develop fully for live birth. However, aside from euploidy, few factors have been confirmed as strongly predictive of outcome. The morphological and developmental characteristics of blastocyst can reflect euploidy and predict implantation potential to some extent (Magli et al. Citation2007, Basile et al. Citation2014, Capalbo et al. Citation2014, Barash et al. Citation2017, Kaing et al. Citation2018, Kim et al. Citation2019). For example, development speed in the cleavage stage is related to chromosomal status and embryo viability (Magli et al. Citation2007), while the total amount and distribution of embryonic fragments can reflect the developmental potential (Basile et al. Citation2014). The association between morphology grade and developmental potential is strongest in the blastocyst stage (Capalbo et al. Citation2014, Barash et al. Citation2017, Kaing et al. Citation2018, Kim et al. Citation2019), but few studies have explored the precise associations of blastocyst morphology grade and development speed with embryonic euploidy status and implantation potential. Further, most such studies have included relatively small sample sizes and reported inconsistent results (Capalbo et al. Citation2014, Barash et al. Citation2017, Kaing et al. Citation2018, Kim et al. Citation2019). For example, the reported relationship between development speed and euploid status has differed across studies. Most of these studies have also enrolled IVF candidates with special medical histories such as, advanced maternal age, history of recurrent IVF failure, and (or) recurrent spontaneous abortion, so applicability to the general patient population is uncertain. Thus, data from patients without infertile history or recurrent failure of pregnancy are needed.
This analysis of PGT-M patients without infertile history or recurrent failure of pregnancy revealed that blastocyst development speed and morphological grade as well as maternal age are associated with euploid status. The euploid rate of D5 blastocysts with high-grade morphology was close to 70%, followed in rank order by D6 high-grade, D5 non-high-grade, and D6 non-high-grade, consistent with the findings of Barash et al. (Citation2017). Alternatively, Capalbo et al. (Citation2014) and Wang et al. (Citation2018) found that only embryo morphology grade predicted euploidy, while development speed (D5 or D6) was related to maternal age but not euploidy. Kim et al. (Citation2019) also found that morphology grade was significantly related to euploidy, but the sample size was too small for further subgroup analysis of D5/D6 embryos (Kim et al. Citation2019). On the contrary, Kaing et al. reported that blastocyst development speed (D5 or D6) rather than morphology was related to euploidy. These inconsistencies may be related to the use of different classification standards for morphology. Various such classification methods have been proposed, but there have been no systematic comparisons for predictive utility. The current results suggest that both blastocyst development speed and morphological grade are independent predictors of blastocyst euploidy after adjusting for female age, although the influence of morphological grade appears predominant.
Morphological grade and development speed were not significant predictors of pregnancy outcomes following euploid blastocyst transfer among this patient group (without advanced age and/or recurrent IVF failure and/or recurrent miscarriage) despite the relatively large sample size. Again, previously studies have drawn different conclusions, possibly due to insufficient sample size (Savio Figueira Rde et al. Citation2015, Barash et al. Citation2017, Kim et al. Citation2019, Viñals Gonzalez et al. Citation2019, Boynukalin et al. Citation2020). Consistent with the current findings, Kim et al. (Citation2019), Wang et al. (Citation2018) and Savio Figueira Rde et al. (Citation2015) found no significant associations between euploid embryo implantation rate and age, development speed, or morphological grade. However, a larger-sample study by Barash and others (Citation2017) found that ongoing pregnancy rate and live birth rate were significantly higher following implantation of D5 euploid blastocysts than D6 euploid blastocysts, and Boynukalin et al. (Citation2020) found that both development speed and morphological grade influenced pregnancy outcomes, with higher spontaneous abortion rate and lower live birth rate following D6 euploid embryo implantation in women with poor reproductive history. Therefore, these factors may not predict pregnancy outcome in patients without reproductive failure, although our sample size may have been insufficient to detect a smaller effect. In the current study, implantation potential was independent of development speed (D5 or D6) and morphology grade as long as the blastocyst was euploid. However, after adjusting for confounders, D6 development speed was a risk factor for early miscarriage. Thus, our results are basically consistent with most previous studies reporting that morphological characteristics and development speed do not predict implantation potential (independent of euploidy), although once implanted, D5 euploid blastocysts are more likely to yield live births than D6 euploid blastocysts.
Considering both morphological quality and development speed, the priority selection sequence for embryo transfer should be D5 high-grade, D6 high-grade, D5 non-high-grade, and D6 non-high-grade. Blastocysts of high-grade morphology should be selected for transfer, and D5 blastocysts should be selected among non-high-grade blastocysts to maximise the probability of euploidy and minimise the probability of early miscarriage.
This study is limited by the retrospective design, which precludes analysis of other potential confounders, and possibly also by insufficient sample size to detect small differences in outcome among blastocyst grades. Therefore, a prospective study with a larger sample size is needed for confirmation.
In conclusion, blastocyst development speed (D5/D6) and morphological grade are independent predictors of blastocyst euploidy but are not significant predictors of euploid blastocyst implantation in patients without prior artificial or natural reproductive failure. The risk of early pregnancy loss is increased by D6 euploidy transfer regardless of morphological grade. To maximise the probability of selecting euploid embryos and minimise the risk of pregnancy loss, the recommended sequence for embryo transfer is D5 high-grade > D6 high-grade > D5 non-high-grade > D6 non-high-grade. The IVF community should work towards establishing a unified classification standard for the grading of embryo morphology to increase comparability among studies and guide clinical decisions.
Authors’ contributions
KD and LL conceived and designed the study. KD and CW analysed the data. KD and LL wrote the first draft of the manuscript and revised it. XH and YZ participated in study implementation and manuscript revision. All authors have read and approved the final manuscript.
Supplemental Material
Download PNG Image (80.2 KB){kind=link}
Supplemental Material
Download PNG Image (63.7 KB){kind=link}
Acknowledgments
We thank all study participants and staff of the Centre of Reproductive Medicine for their support.
Data availability statement
Data supporting the results of this study will be shared upon reasonable request to the corresponding author.
Additional information
Funding
References
- Alfarawati, S., et al., 2011. The relationship between blastocyst morphology, chromosomal abnormality, and embryo gender. Fertility and Sterility, 95 (2), 1–7.
- Arce, J.C., et al., 2006. Interobserver agreement and intraobserver reproducibility of embryo quality assessments. Human Reproduction (Oxford, England), 21 (8), 2141–2148.
- Bamford, T., et al., 2022. Morphological and morphokinetic associations with aneuploidy: a systematic review and meta-analysis. Human Reproduction Update, 28 (5), 656–686.
- Barash, O.O., et al., 2017. Association between growth dynamics, morphological parameters, the chromosomal status of the blastocysts, and clinical outcomes in IVF PGS cycles with single embryo transfer. Journal of Assisted Reproduction and Genetics, 34 (8), 1007–1016.
- Basile, N., et al., 2014. Increasing the probability of selecting chromosomally normal embryos by time-lapse morphokinetics analysis. Fertility and Sterility, 101 (3), 699–704.
- Boynukalin, F.K., et al., 2020. Parameters impacting the live birth rate per transfer after frozen single euploid blastocyst transfer. PLoS One, 15 (1), e0227619.
- Capalbo, A., et al., 2014. Correlation between standard blastocyst morphology, euploidy and implantation: an observational study in two centers involving 956 screened blastocysts. Human Reproduction (Oxford, England), 29 (6), 1173–1181.
- Coonen, E., et al., 2020. ESHRE PGT Consortium good practice recommendations for the detection of structural and numerical chromosomal aberrations. Human Reproduction Open, 2020 (3), hoaa017.
- Gardner Dk, S.W.B., 1999. In vitro culture of human blastocyst. In: Towards reproductive certainty: infertility and genetics beyond 1999.
- Kaing, A., et al., 2018. Earlier day of blastocyst development is predictive of embryonic euploidy across all ages: essential data for physician decision-making and counseling patients. Journal of Assisted Reproduction and Genetics, 35 (1), 119–125.
- Kim, M.K., et al., 2019. Correlation between morphologic grading and euploidy rates of blastocysts, and clinical outcomes in in vitro fertilization preimplantation genetic screening. Journal of Korean Medical Science, 34 (4), e27.
- Luo, L., et al., 2017. Early miscarriage rate in lean polycystic ovary syndrome women after euploid embryo transfer – a matched-pair study. Reproductive Biomedicine Online, 35 (5), 576–582.
- Magli, M.C., et al., 2007. Embryo morphology and development are dependent on the chromosomal complement. Fertility and Sterility, 87 (3), 534–541.
- Rocha, J.C., et al., 2016. Methods for assessing the quality of mammalian embryos: How far we are from the gold standard? JBRA Assisted Reproduction, 20 (3), 150–158.
- Savio Figueira Rde, C., et al., 2015. Blastocyst morphology holds clues concerning the chromosomal status of the embryo. International Journal of Fertility & Sterility, 9 (2), 215–220.
- Viñals Gonzalez, X., et al., 2019. Euploid blastocysts implant irrespective of their morphology after NGS-(PGT-A) testing in advanced maternal age patients. Journal of Assisted Reproduction and Genetics, 36 (8), 1623–1629.
- Wang, A., et al., 2018. Euploidy in relation to blastocyst sex and morphology. Journal of Assisted Reproduction and Genetics, 35 (9), 1565–1572.