

Abstract
Background
To evaluate outcomes of laparoscopic retroperitoneal para-aortic lymphadenectomy for stage 1b3-3b cervical cancer.
Methods
Pathology databases searched for all para-aortic lymphadenectomy cases 2005–2016. Descriptive statistics were used to analyse baseline characteristics, cox models for treatment affect after accounting for variables, and Kaplan Meier curves for survival (STATA v15).
Results
191 patients had 1b3-3b cervical cancer of which 110 patients had Para-aortic lymphadenectomy. 8 (7.3%) patients stage 1b3, 82 (74.6%) stage 2b, and 20 (18.1%) stage 3b cervical cancer. Mean lymph node count 11.7 (SD7.6). The intra-operative and post-operative 30 day complication rates were 8.8% (CI: 4.3%, 15.7%) and 5.3% (CI: 1.9%, 11.2%) respectively.
Para-aortic nodes were apparently positive on CT/MRI in 5/110 (5%) cases. Cancer was found in 10 (8.9%, CI: 4.3%, 15.7%) cases on histology, all received extended field radiotherapy. Only 2 were identified on pre-operative CT/MRI imaging. 3 of 10 suspected node-positive cases on CT/MRI had negative histology. Para-aortic lymphadenectomy led to alteration in staging and radiotherapy management in 8 (8%, CI: 3.7%, 14.6%) patients. Mean overall survival 42.81 months (SD = 31.79 months). Survival was significantly higher for women undergoing PAN (50.57 (SD 30.7) months) compared to those who didn’t (31.27 (SD 32.5) months)
Conclusion
Laparoscopic retroperitoneal para-aortic lymphadenectomy is an acceptable procedure which can guide treatment in women with locally advanced cervical cancer.
PLAIN LANGUAGE SUMMARY
We evaluated outcomes for patients with stage 1b3-3b cervical cancer that had lymph nodes removed prior to planning their chemoradiotherapy. There were 3 groups – patients that had their lymph nodes removed, those that did not and those that had their procedure abandoned so didn’t have their lymph nodes removed. We looked at the lymph nodes down the microscope to see if they contained cancer and compared this to their pre-operative imaging. 8 patients had a change to their staging and treatment because they were found to have cancer in the lymph nodes. We found that the keyhole procedure to remove lymph nodes is an acceptable procedure which can guide treatment in women with locally advanced cervical cancer.
Keywords:
Introduction
Cervical cancer is the 4th most common cancer in women globally (Jolly et al. Citation2018) and used to be clinically staged. Now presence of para-aortic lymph node metastasis is included in the latest staging classification determined by an ‘r’ or ‘p’ denoting if radiological or pathological staging respectively (Bhatla et al. Citation2019). This is because of potential discordance between using pathology or radiology for identification of para-aortic nodal metastases. The number of patients with para-aortic lymph node involvement may be significant as studies have shown 16–20% stage 1, 12–17% stage 2, 32–40% stage 3 and 33% stage 4 patients with cervical cancer have histologically proven para-aortic lymph node metastases (Leblanc et al. Citation2007, Cosin et al. Citation1998) which is a major prognostic factor influencing survival (Lanciano and Corn Citation1994, Sonoda et al. Citation2003, Denschlag et al. Citation2005, Marnitz et al. Citation2005, Leblanc et al. Citation2007).
Currently the standard treatment for stage 1b3-3b cervical cancer is concurrent pelvic radiotherapy with cisplatin chemotherapy (Keys et al. Citation1999, Morris et al. Citation1999). Additionally, patients with para-aortic nodal metastases are given extended field radiotherapy. ‘Prophylactic’ extended field radiotherapy in all patients undergoing chemo-radiotherapy to include the para-aortic nodes does not improve survival, but does increase morbidity (Haie et al. Citation1988, Rotman et al. Citation1995, Small et al. Citation2011). Therefore it is important to establish which patients have para-aortic metastases as they may benefit from extended field radiotherapy.
There have been several reviews demonstrating sensitivities and specificities of different imaging modalities using histology (biopsy or full lymphadenectomy) as the gold standard (Selman et al. Citation2008, Smits et al. Citation2014, Liu et al. Citation2017, Luo et al. Citation2018). One included 72 studies, 5042 women (stage 1-4 cervical cancer) (Selman et al. Citation2008) and showed: CT sensitivity 57.5% (95% CI 53.5–61.4), specificity 92.3% (95% CI 91.1–93.5), MRI sensitivity 55.5% (95% CI 49.2–61.7), specificity 93.2% (95% CI 91.4–94.0) and PETCT sensitivity 74.7% (95% CI 63.3–84.0), specificity 97.6% (95% CI 95.4–98.9). Another meta-analysis demonstrated the area under the curve (AUC) of DWI-MRI (0.92) and PET or PET/CT (0.90) were better than CT (0.83), and the difference was significant (DWI-MRI vs. CT: Z = 4.61, p < 0.001; PET or PET/CT vs. CT: Z = 3.61, p = 0.001) (Liu et al. Citation2017). They concluded that among the 4 non-invasive modalities, the PET or PET/CT has the highest specificity, and DWI-MRI has the highest sensitivity (Liu et al. Citation2017).
Overall imaging has limitations and while PETCT appears to outperform other imaging modalities (Luo et al. Citation2018) it still misses a large proportion of women with positive lymph nodes leading to under treatment. A French study evaluating PETCT reported the sensitivity for detecting metastases in para-aortic lymph nodes to be as low as 33% (Leblanc et al. Citation2011). Whether pre-treatment surgical staging should be undertaken or not remains an area of debate with the majority of cancer centres using imaging to guide treatment. The latest ESGO cervical cancer guidelines state ‘Para-aortic LN dissection (PALND), at least up to inferior mesenteric artery, may be considered in locally advanced cervical cancer with negative para-aortic LN on imaging for staging purposes’ and for patients with a cervical cancer on histology following a simple hysterectomy ‘Para-aortic LN dissection, at least up to inferior mesenteric artery, may be considered for staging purposes in patients with positive pelvic nodes at imaging, or at frozen section’ (Cibula et al. Citation2023). We report on outcomes of an unselected case series of patients who have had retroperitoneal para-aortic lymph node dissection for locally advanced cervical cancer at a single cancer centre.
Methods
The study was registered as an audit at University College Hospital and complies with all ethical requirements. All women with stage 1b3-3b cervical cancer receive concurrent chemo-radiotherapy and are offered pre-treatment systematic para-aortic lymph node dissection. We report on retrospectively reviewed outcomes of retroperitoneal para-aortic lymph node dissection on all cases of stage 1b3-3b cervical cancer at University College Hospital, London. All records of women with cervical cancer from 01 January 2005 to 01 January 2016 were searched using the Gynaecology Oncology and pathology databases. Women who were unfit for surgery or extended field radiotherapy were not offered the procedure. All patients with stage 1b3-3b cervical cancer were included. Stages below 1b3 and stage 4 were excluded.
All patients had an MRI pelvis and CT for staging prior to retroperitoneal para-aortic lymphadenectomy. Size criteria for positive lymph nodes was ≥1cm measurement in short axis. If patients had histologically proven para-aortic lymph node metastases they received extended field radiotherapy to the para-aortic lymph nodes with standard concurrent cisplatin chemotherapy with pelvic radiotherapy.
A demographic and clinico-pathological data collection proforma was completed for each patient including age, stage, grade, length of surgery, lymph nodes harvested, complications, haemoglobin, time to definitive chemo-radiotherapy, details of treatment given, recurrence, and survival outcomes.
Descriptive statistics were used to analyse baseline characteristics. Data are expressed as mean and standard deviation (SD) for normally distributed variables. Incidence was calculated as number of events divided by total of cohort, and the result was expressed as proportion with 95% confidence interval (95% CI). Mann Whitney test was used to compare continuous variables between groups and chi-square tests used for categorical variables. Overall survival was calculated from time of surgery to time of death, with censorship at time of last follow up. The censoring date was last clinical follow up collected on 20th December 2016. Kaplan Meier survival curves were plotted for the three groups of patients: (a) No surgery; (b) PA node surgery, and (c) Abandoned surgery (procedure attempted but unsuccessful). A Cox model was fitted with surgery group as a categorical variable, and ‘No surgery’ as the reference category. A Wald test was used to compare the survival outcomes between the different groups. An additional Cox model included stage (1b3, 2, 3), grade (1, 2, 3), histology (squamous cell carcinoma; adeno-carcinoma, other) and age at diagnosis. All analyses were performed using Stata 15.1.
Results
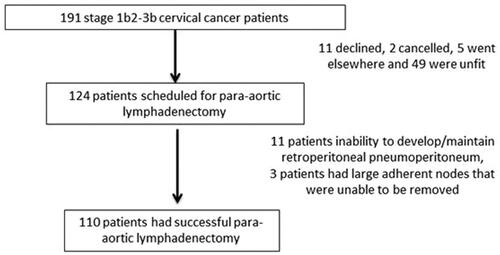
191 patients were diagnosed with stages 1b3-3b cervical cancer between 2005 and 2016. Retroperitoneal para-aortic lymphadenectomy was scheduled for 124/191 patients. Of the remainder, 11 declined (patient choice), 2 cancelled, 5 elected to go elsewhere and 49 were unfit due to comorbidities/performance status of 3. In total 67 patients did not have retroperitoneal lymphadenectomy. The procedure was abandoned at the outset in 14/124 (11.3%, CI: 5.0–16.2) patients: 11/124 (8.9%) patients had inability to develop/maintain retroperitoneal pneumoperitoneum and 3/124 (2.4%) patients had large densely adherent nodes that were technically unable to be removed. Patients with extremely densely adherent nodes that were unable to be removed had chemoradiotherapy with extended field radiotherapy to the para-aortic region. In total 110 patients underwent para-aortic lymphadenectomy (see ).
Figure 1. Flow diagram illustrating the patients that did not have successful para-aortic lymphadenectomy.
shows the characteristics of patients in the cohort who underwent laparoscopic retroperitoneal para-aortic lymphadenectomy, and those who did not. The majority of patients in the para-aortic lymph node surgery group (75%) had stage 2 cervical cancer and 68% had squamous cell carcinoma. There were approximately half with grade 2 and the other half had grade 3 cervical cancer. The patients with no surgery were more likely to have stage 4 disease 6% vs 0%; and were older mean age 64 (SD 15.4) years vs 45.2 (SD 12.2) years vs 49.9 (SD 8.4) years for no surgery, successful surgery and abandoned surgery respectively.
Table 1. Characteristics of patients undergoing laparoscopic retroperitoneal para-aortic lymphadenectomy, and those with abandoned or no surgery NB.
The intra-operative and post-operative complication rates at 30 days were 8.8% (95%CI: 4.3%, 15.7%) and 5.3% (95%CI: 1.9%, 11.2%) respectively. These included 3 vascular injuries (Clavien-Dindo 3), 8 symptomatic lymphocysts (Clavien-Dindo 3), and 1 bowel and ureteric injury (Clavien-Dindo 3) (Clavien et al. Citation1992). The mean operative time was 135 mins, and mean drop in haemoglobin was 1.3 g/dl. The mean time from successful surgery to chemo-radiotherapy was 23 days (SD 17.9) demonstrating that para-aortic lymphadenectomy does not delay definitive treatment. The mean length of stay for successful surgery was 1.4 days (SD 0.7).
Patients with abandoned or no surgery were offered a CTPET scan to determine lymph node status. In the no surgery group 13 patients had positive para-aortic lymph nodes on CT or MRI and a further 5 were positive on CTPET. All were considered for extended field radiotherapy but only 7 received extended field radiotherapy as the remaining 11 patients were not fit enough. In addition 18 patients did not receive any treatment as they were not fit (performance status 3) and all died shortly after diagnosis. In the abandoned surgery group 4 patients had positive para-aortic lymph nodes on CT or MRI and a further 3 were positive on CTPET. Only 4 received extended field radiotherapy as the remaining 3 patients were not fit.
Para-aortic nodes were positive on CT/MRI in 5/110 cases and all received extended field radiotherapy (). Cancer was found in 10 (8.9%, CI: 4.3%, 15.7%) cases, all of whom received extended field radiotherapy. Only 2 of these were identified on pre-operative CT/MRI imaging. The sensitivity, specificity, PPV and NPV for CT/MRI in our cohort was 20% (95% CI 2.52%–55.61%), 97% (95% CI 91.48%–99.38%), 40% (95%CI 11.18%–77.93%), 92.38% (95%CI 89.88%–94.31%) respectively. The overall mean lymph node count was 11.7 (SD7.6) but this increased following a learning curve and varied between 4.3 (SD 1.7) in 2005 to 15.3 (SD 6.64) in 2014. Assuming a learning curve of 20 cases, it also took 24 months exactly to reach the 20th case. Four patients had negative PALN histology and received extended field radiotherapy (2 had poor prognostic features (high grade carcinoma and lymphovascular space invasion present with positive pelvic nodes on imaging), 2 patients had low nodal count (both had 2) but positive on imaging who had their surgery in 2005 during the early part of the learning curve. Para-aortic lymphadenectomy led to alteration in radiotherapy management in 8 (8%, CI: 3.7%, 14.6%) patients. The mean overall survival of the entire cohort was 42.81 months (SD 31.79 months). The overall survival for patients who had a laparoscopic retroperitoneal lymphadenectomy was 50.57 (SD 30.7) months and those with no surgery was 31.27 (SD 32.5) months. While those patients that had surgery abandoned had an overall survival of 35.35 (SD 12.6) months. The Kaplan-Meier survival curves are given in . Univariate Cox-models showed no significant impact of grade or age on survival. However, adenocarcinoma histology had better prognosis (HR 0.24, CI 0.09 0.67, p = 0.007) and nonsquamous/nonadeno histology had worse prognosis (HR 4.1, CI 1.4 11.5, 0 = 0.008). The multvariate Cox model adjusted for covariates of stage, age, grade and histology. Compared to the referent no surgery group, survival outcomes were better in the PALN surgery (HR 0.33, CI:0.16, 0.68 p = 0.003) and abandoned surgery (HR 0.31, CI:0.01 0.9, p = 0.043) groups.
Figure 2. Differences of overall survival between patients with no surgery, abandoned and successful para-aortic lymphadenectomy.
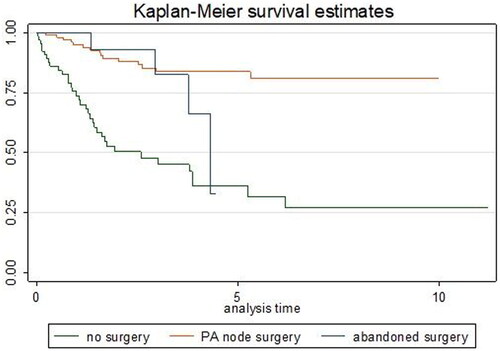
Table 2. Outcome of MRI/CT imaging and histological assessment of para-aortic lymph node metastases.
Discussion
In a single institution experience, using a well defined protocol, we show that systematic para-aortic lymphadenectomy using minimal access surgery is safe and may be used to improve triage for extended field radiotherapy and optimise treatment for patients with locally advanced cervical cancer who are fit for surgery. This potentially impacts two thirds of patients presenting with stage 1b3-3b cervical cancer. Eight of 13 (61.5%) patients receiving extended field radiotherapy in our cohort would have been missed without undertaking para-aortic lymphadenectomy. Minimal access surgery is associated with short stay in hospital quick recovery time and does not add significant delay to onset of primary chemo-radiotherapy. The procedure has an acceptable morbidity and complication rate. Like any surgical technique this procedure has a learning curve, demonstrated by our increase in lymph-node count with time. While our study design cannot specifically address this issue, one can hypothesise or speculate whether this may lead to a survival advantage. Our study given a cohort design has biases, and our groups are unbalanced. There are selection biases and difficulties of comparative analysis considering the control group is based on a historical series and includes patients with stage IV (6%) and worse clinical performance. Ideally a RCT design is needed to adjust for all confounders between groups and address this issue comprehensively. Nevertheless, the current ESGO cervical cancer guidelines suggest that this option can be considered.
We performed a bilateral dissection of the para-aortic lymph nodes up to the inferior mesenteric artery and not up to the renal vein. Studies have shown the very low rates of skip nodal metastasis with only 3% of patients with positive para-aortic nodal metastases above the inferior mesenteric artery (Leblanc et al. Citation2016).
Our complication rates are similar to other series (Gil-Moreno et al. Citation2011, Del Pino et al. Citation2013). The risk of vascular and major visceral injuries is low (3.6%). The overall morbidity is acceptable and consistent with other major gynaecological oncology surgery (Iyer et al. Citation2015). Para-aortic lymphadenectomy appears to be well tolerated and did not significantly alter time to chemo-radiotherapy in our cohort.
Advantages of our study include a standardised surgical protocol with inclusion of all cases presenting with stage 1b3-3b cervical cancer. Procedures were performed by a small group of trained surgeons from a single institution with little variation in surgical technique. There were good nodal counts after the learning curve. We have also demonstrated an acceptable time to receive chemo-radiotherapy from time of surgery.
Limitations of the study include its retrospective cohort design and lack of PETCT imaging for all patients to enable comparison of histological assessment with the most accurate imaging modality. Additionally a non-randomised design cannot adjust for all confounders and conclusively address the issue of impact of surgical para-aortic lymphadenectomy on survival.
Our metastatic para-aortic lymph node rate was 10/110 patients (9.0%) which is slightly lower than 16.3–27% from other case series using histology as the gold standard (Cosin et al. Citation1998, Leblanc et al. Citation2007, Leblanc et al. Citation2011). 8/10 patients with positive para-aortic lymph node metastases were not identified by pre-operative CT/MRI imaging, confirming that histological diagnosis remains the gold standard for diagnosis. PETCT is considered to perform better than CT or MRI for detection of para-aortic lymph node metastases () but its sensitivity has limitations and ranges from 33% to 75% in the larger series (Selman et al. Citation2008, Liu et al. Citation2017, Luo et al. Citation2018). However we did not undertake PETCT given additional cost implications (compared to standard CT), and its use does not change the management of our patients undergoing surgery.
Consistent with previous literature reports we found stage and histology to be independent factor associated with survival (Vinh-Hung et al. Citation2007). Non squamous/adenocarcinoma histology had four times worse prognosis. However, there was a suggestion that adenocarcinoma histology has better prognosis (HR 0.24 to 0.35 on univariate and combined Cox models). Of note, adenocarcinoma patients were more likely to have had PALN being much commoner in the surgical (31%) compared to no-surgery (7%) arm. Adenocarcinoma is not previously known to have better prognosis than squamous cell carcinoma, with some literature reports pointing to poorer outcomes with adenocarcinoma (Vinh-Hung et al. Citation2007).
Whether para-aortic lymph node dissection in locally advanced cervical cancer to guide radiotherapy treatment improves overall survival is an unanswered question. It is possible that minimal-access para-aortic lymphadenectomy to remove nodal metastasis in patients with locally advanced cervical cancer might offer a direct therapeutic benefit in itself (Cosin et al. Citation1998, Kupets et al. Citation2002, Cheung et al. Citation2011). However, this benefit has not been confirmed by other studies (Lai et al. Citation2003, Tammela et al. Citation2004). There are only 2 prospective randomised controlled trials comparing clinical staging (CT or PETCT scan) with surgical staging (either intra-peritoneal or retroperitoneal para-aortic lymphadenectomy). In the first one published in 2003 (Lai et al. Citation2003) recruited only 63 women and stopped prematurely because women in the surgical staging arm appeared to have a poorer progression free survival and higher recurrence rates. However, there have been criticisms of this study. The para-aortic lymph node count was low which may be insufficient to exert a positive effect on survival. There were more poor prognostic features in patients in the surgical staging arm compared to patients in the clinical staging arm which could have affected the outcome (Lai et al. Citation2003). In the second prospective randomised controlled international mutli-centre trial called Uterus-11 (Marnitz et al. Citation2020b) 255 patients with stage IIB-IVa cervical carcinoma were randomised to surgical staging (para-aortic lymphadenectomy) or clinical staging using CT or PETCT. In the clinical staging arm paraaortic node biopsy was performed in patients with suspicious nodes on imaging. Patients had extended field radiotherapy if histologically positive lymph nodes and followed up for 90 months. No difference in disease-free survival (p = 0.084), however there was a significant difference in disease-free survival for surgical staging in patients with stage 2B disease (HR 0.51, 95% CI 0.30 to 0.86, p = 0.011). In the post-hoc analysis, surgical staging was associated with better cancer-specific survival (HR 0.61, 95% CI 0.40 to 0.93, p = 0.020), although the study was inadequately powered for this sub-group analysis. This underpins the importance of accurate staging as there were a high percentage of distant metastases in both groups and this study did not have central imaging review. Both groups had CT and MRI but only 47 patients in total had a CTPET.
Holcomb et al. (Citation1999) found significantly higher survival of 29 months in 89 patients with pre-treatment lymph node staging, compared to 19 months (P = 0.01) in 179 patients without pre-treatment staging. This was in keeping with our study that demonstrated an overall survival of 43.56 months for those patients who had a laparoscopic retroperitoneal lymphadenectomy compared to 28.8 months for those that had no surgery. However, these results are confounded by patients undergoing surgical staging being a better prognostic group as they were younger, had better performance status, and were more likely to be stage 2 or 3 than stages 3 or 4. Marnitz et al. (Citation2020a) found that patients with positive results of surgical para-aortic lymph node staging, whose chemoradiotherapy had been tailored to the extension of their disease, had survival rates equivalent to those of patients with negative results. A randomised trial concluded that there is a benefit of extended field Radiotherapy over pelvic Radiotherapy for patients with locally advanced cervical cancer and high risk features (Rotman et al. Citation1995). However other small retrospective studies suggest that lymphadenectomy-tailored radiotherapy may not provide a survival benefit for patients with locally advanced cervical cancer (Hong et al. Citation2010, Rajasooriyar et al. Citation2011).
The PAROLA trial (PARa-aOrtic LymphAdenectomy in locally advanced cervical cancer) is a randomised controlled trial to demonstrate if chemoradiation with tailored external beam radiation field based on surgical staging and pathologic examination of the para-aortic lymph node is associated with improved 3-year disease-free survival compared with patients staged with PET/CT staging only. The trial has just started recruiting with results due 2030 (Martinez et al. Citation2023)
Our cohort study shows surgical para-aortic lymphadenectomy triage for optimising extended field radiotherapy is both possible and safe. However, there remains uncertainty and debate in the literature of the definite benefit of this approach. We also speculate whether this may be more beneficial for women with adenocarcinoma. This is an interesting issue that needs addressing in the future. A pilot Dutch study assessing safety and feasibility of undertaking a RCT to address this issue is also ongoing (Tax et al. Citation2018). Given paucity of randomised trial data and criticisms of the only trials so far, it is important for further research and an appropriately powered and designed RCT to address this issue. Such a trial will need to be multicentre and will need to adequately control for surgical quality. This will need buy in and support of the broader clinical community. At present we feel it is reasonable to offer carefully selected women will locally advanced cervical cancer a retroperitoneal para-aortic lymphadenectomy followed by extended field radiotherapy if para-aortic metastases are confirmed on histology.
Ethical statement
The study was registered as an audit at University College Hospital. I confirm that all the research meets ethical guidelines and adheres to the legal requirements of the UK.
Acknowledgements
We would like to acknowledge the University hospitals Bristol and Weston NHS foundation trust library for their help with the literature review.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, RM upon reasonable request.
Additional information
Funding
References
- Bhatla, N., et al., 2019. Revised FIGO staging for carcinoma of the cervix uteri. International Journal of Gynaecology and Obstetrics, 145 (1), 1–8.
- Cheung, T.H., et al., 2011. Debulking metastatic pelvic nodes before radiotherapy in cervical cancer patients: a long-term follow-up result. International Journal of Clinical Oncology, 16 (5), 546–552.
- Cibula, D., et al., 2023. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer – Update 2023. International Journal of Gynecologic Cancer, 33 (5), 649–666.
- Clavien, P.A., Sanabria, J.R. and Strasberg, S.M., 1992. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery, 111 (5), 518–526.
- Cosin, J.A., et al., 1998. Pretreatment surgical staging of patients with cervical carcinoma: the case for lymph node debulking. Cancer, 82 (11), 2241–2248.
- Del Pino, M., et al., 2013. Laparoscopic lymphadenectomy in advanced cervical cancer: prognostic and therapeutic value. International Journal of Gynecological Cancer, 23 (9), 1675–1683.
- Denschlag, D., et al., 2005. Evaluation of patients after extraperitoneal lymph node dissection for cervical cancer. Gynecologic Oncology, 96 (3), 658–664.
- Gil-Moreno, A., et al., 2011. Pretherapeutic extraperitoneal laparoscopic staging of bulky or locally advanced cervical cancer. Annals of Surgical Oncology, 18 (2), 482–489.
- Haie, C., et al., 1988. Feasibility study of an alternating schedule of radiotherapy and chemotherapy in advanced uterine cervical carcinoma. Radiotherapy and Oncology, 12 (2), 121–127.
- Holcomb, K., et al., 1999. The impact of pretreatment staging laparotomy on survival in locally advanced cervical carcinoma. European Journal of Gynaecological Oncology, 20 (2), 90–93.
- Hong, D.G., et al., 2010. Survival benefit of laparoscopic surgical staging-guided radiation therapy in locally advanced cervical cancer. Journal of Gynecologic Oncology, 21 (3), 163–168.
- Iyer, R., et al., 2015. Predictors of complications in gynaecological oncological surgery: a prospective multicentre study (UKGOSOC-UK gynaecological oncology surgical outcomes and complications). British Journal of Cancer, 112 (3), 475–484.
- Jolly, S., et al., 2018. Improving Global Outcomes in Cervical Cancer: The Time Has Come for International Federation of Gynecology and Obstetrics Staging to Formally Incorporate Advanced Imaging. Journal of Global Oncology, 4, 1–6.
- Keys, H. M., 3rd., et al., 1999. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. The New England Journal of Medicine, 340 (15), 1154–1161.
- Kupets, R., Thomas, G.M. and Covens, A., 2002. Is there a role for pelvic lymph node debulking in advanced cervical cancer? Gynecologic Oncology, 87 (2), 163–170.
- Lai, C.-H., et al., 2003. Randomized trial of surgical staging (extraperitoneal or laparoscopic) versus clinical staging in locally advanced cervical cancer. Gynecologic Oncology, 89 (1), 160–167.
- Lanciano, R.M. and Corn, B.W., 1994. The Role of Surgical Staging for Cervical Cancer. Seminars in Radiation Oncology, 4 (1), 46–51.
- Leblanc, E., et al., 2007. Therapeutic value of pretherapeutic extraperitoneal laparoscopic staging of locally advanced cervical carcinoma. Gynecologic Oncology, 105 (2), 304–311.
- Leblanc, E., et al., 2011. Accuracy of 18-fluoro-2-deoxy-D-glucose positron emission tomography in the pretherapeutic detection of occult para-aortic node involvement in patients with a locally advanced cervical carcinoma. Annals of Surgical Oncology, 18 (8), 2302–2309.
- Leblanc, E., et al., 2016. Should systematic infrarenal para-aortic dissection be the rule in the pretherapeutic staging of primary or recurrent locally advanced Cervix cancer patients with a negative preoperative para-aortic PET Imaging? International Journal of Gynecological Cancer, 26 (1), 169–175.
- Liu, B., Gao, S. and Li, S., 2017. A comprehensive comparison of CT, MRI, positron emission tomography or positron emission tomography/CT, and diffusion weighted imaging-MRI for detecting the lymph nodes metastases in patients with cervical cancer: a meta-analysis based on 67 studies. Gynecologic and Obstetric Investigation, 82 (3), 209–222.
- Luo, Q., Luo, L. and Tang, L., 2018. A network meta-analysis on the diagnostic value of different imaging methods for Lymph Node metastases in patients with cervical cancer. Technology in Cancer Research & Treatment, 17, 1533034617742311. PMID: 29343205; PMCID: PMC5784560.
- Marnitz, S., et al., 2005. Is there a benefit of pretreatment laparoscopic transperitoneal surgical staging in patients with advanced cervical cancer? Gynecologic Oncology, 99 (3), 536–544.
- Marnitz, S., et al., 2020. Surgical versus clinical staging prior to primary chemoradiation in patients with cervical cancer FIGO stages IIB-IVA: oncologic results of a prospective randomized international multicenter (Uterus-11) intergroup study. International Journal of Gynecological Cancer, 30 (12), 1855–1861. Dec PMID: 33293284; PMCID: PMC7788482.
- Martinez, A. et al., 2023. PARa-aOrtic LymphAdenectomy in locally advanced cervical cancer (PAROLA trial): a GINECO, ENGOT, and GCIG study. International Journal of Gynecologic Cancer, 33 (2), 293–298.
- Morris, M., et al., 1999. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. The New England Journal of Medicine, 340 (15), 1137–1143.
- Rajasooriyar, C., et al., 2011. Patterns of failure and treatment-related toxicity in advanced cervical cancer patients treated using extended field radiotherapy with curative intent. International Journal of Radiation Oncology, Biology, Physics, 80 (2), 422–428.
- Rotman, M., et al., 1995. Prophylactic extended-field irradiation of para-aortic lymph nodes in stages IIB and bulky IB and IIA cervical carcinomas. Ten-year treatment results of RTOG 79-20. JAMA, 274 (5), 387–393.
- Small, W., et al., 2011. Extended-field irradiation and intracavitary brachytherapy combined with cisplatin and amifostine for cervical cancer with positive para-aortic or high common iliac lymph nodes: results of arm II of Radiation Therapy Oncology Group (RTOG) 0116. International Journal of Gynecological Cancer, 21 (7), 1266–1275.
- Selman, T.J., et al., 2008. Diagnostic accuracy of tests for lymph node status in primary cervical cancer: a systematic review and meta-analysis. CMAJ: Canadian Medical Association Journal = Journal de L’Association Medicale Canadienne, 178 (7), 855–862.
- Smits, R.M., Zusterzeel, P.L. and Bekkers, R.L., 2014. Pretreatment retroperitoneal para-aortic lymph node staging in advanced cervical cancer: a review. International Journal of Gynecological Cancer, 24 (6), 973–983. Jul PMID: 24978708.
- Sonoda, Y., et al., 2003. Prospective evaluation of surgical staging of advanced cervical cancer via a laparoscopic extraperitoneal approach. Gynecologic Oncology, 91 (2), 326–331.
- Tammela, J., Bundy, B. and Odunsi, K., 2004. Reassessment of pelvic lymph node debulking in advanced cervical cancer. Gynecologic Oncology, 92 (3), 1014–1015.
- Tax, C., et al., 2018. Para-aortic lymphadenectomy in advanced stage cervical cancer, a protocol for comparing safety, feasibility and diagnostic accuracy of surgical staging versus PET-CT; PALDISC trial. Pilot and Feasibility Studies, 4 (1), 27.
- Vinh-Hung, V., et al., 2007. Prognostic value of histopathology and trends in cervical cancer: a SEER population study. BMC Cancer, 7 (1), 164. PMID: 17718897; PMCID: PMC1994954.