
Abstract
This study aims to explore the correlation between different social support patterns and perinatal mental health, and the mediating role of social trust in this. A cross-sectional survey was conducted in Jiangsu, China, with a sample size of 1705 pregnant respondents. Latent class analysis (LCA) was utilized to identify various social support patterns, while a multiple regression model was employed to analyze the mediating effect of social trust on the relationship between social support patterns and perinatal mental health. The study found four distinct social support patterns among the respondents: primary relationship-centric support, overall weak support, primary-secondary relationship-balanced support, and overall strong support. In the relationship between social support patterns and perinatal mental health, social trust played both a partial and full mediating role. The findings indicate that a social support system that enhances maternal trust and promotes honest disclosure of symptoms can effectively promote perinatal mental health.
Introduction
Pregnancy is a critical period that is strongly associated with an increased risk of mental health problems[Citation1]. The health of both mothers and children is closely tied to the achievement of the Millennium Development Goals (MDGs). Consequently, the mental health and well-being of women during the perinatal period have emerged as significant global health concerns [Citation2]. In China, there has been a steady increase in the prevalence of maternal mental health issues in recent years, with nearly 70% of women reporting negative emotions during the 3-6 months of pregnancy [Citation3]. The COVID-19 pandemic has further exacerbated anxiety and depressive symptoms among pregnant and puerperal individuals in China [Citation4]. However, most previous studies have primarily focused on postpartum mental health problems, such as postpartum depression, and have not given sufficient attention to prenatal mental health. There is evidence that the prevalence of prenatal mental health problems is significantly higher than postnatal mental health problems in both high-income and low-income countries [Citation5]. Vulnerable prenatal mental health not only impacts obstetric and pregnancy outcomes but also has long-term implications for the healthy development of children and families [Citation6,Citation7].
Social support plays a crucial role in promoting perinatal mental health. Having a strong support system can assist mothers in navigating challenges, enhancing their overall well-being, and reducing the risk of mental health issues [Citation8–12]. The structure of social support varies depending on demographic characteristics, socioeconomic status (SES), and cultural background. In the United States, African American and Latino women often prioritize familial support over seeking external assistance. In contrast, White and other non-Black, non-Hispanic women tend to rely more on health professionals and their partners for support, as they perceive less direct involvement from family members during pregnancy. Consequently, these women are less likely to feel frustrated by perceived lack of support from friends and family [Citation13,Citation14].
In Chinese society, maternal support networks are primarily composed of primary relationships, including kinship support and neighborhood assistance, rooted in the traditional Chinese reproductive system. These networks offer emotional, instrumental, and informational support to pregnant women [Citation15]. It is noteworthy that the structure of maternal social support networks in contemporary Chinese society is evolving from informal primary relationships to formal secondary relationships [Citation16]. Recent studies indicates a growing trend of young mothers seeking assistance from professionals like obstetricians and community general practitioners, who provide services such as maternal mental health screening, mental health services throughout pregnancy and childbirth, and guidance on preventing and treating postpartum depression [Citation17,Citation18]. Social support is derived from various sources like family members, friends, coworkers, neighbors, the Internet, health professionals, as well as community and government agencies, leading to diverse patterns of social support with heterogeneity [Citation19]. These models encompass different forms of support, such as emotional, material instrumental, informational, and evaluative support, collectively influencing women’s mental health during pregnancy. Therefore, examining the patterns of social support can offer insights into the current status and characteristics of maternal social support in China. Moreover, it can clarify the relationship between social support and perinatal mental health.
Social trust is a crucial factor in interpersonal relationships, particularly in the formation of formal support networks such as those involving health professionals, government agencies, and communities. It significantly influences the behavior of individuals within these networks, shaping their interaction experiences and impacting overall health outcomes. There is evidence that when patients trust their health professionals, they are more likely to seek care and be satisfied with their treatment. This can lead to better participation in treatment decisions and positive health behaviors, ultimately resulting in improved health outcomes [Citation20]. Conversely, when patients mistrust their doctors, they may have negative perceptions and experience low satisfaction with the treatment process, potentially affecting their mental well-being [Citation21].
Professional trust in doctors in Chinese society is closely linked to the public’s trust in the social system, reflecting the level of in social institutions [Citation22]. This social trust has broad implications beyond the doctor-patient relationship, extending to government and community support, as well as other social networks. Social trust, encompassing trust in colleagues, citizens and institutions, can positively impact an individual’s psychological well-being by promoting reliable interactions, reducing transaction costs, and alleviating suspicion-related stress [Citation23,Citation24]. Additionally, social trust can foster engagement participation in social activities, facilitate relationship-building, and provide access to resources and information, all of which enhance resilience to health risks [Citation25]. Conversely, individual-level social trust can also influence socio-political circumstances, ultimately affecting the mental health of individuals [Citation26].
Existing research has established a strong correlation between social support and prenatal mental health. However, there is a lack of studies in China that explore the influences of different social support patterns on prenatal mental health, and the underlying mechanisms of these associations remain unclear. Given the significant relationship and predictive impacts between these factors, it is essential to construct a theoretical model to elucidate the link between social support patterns and perinatal mental health. Building upon previous research, this study aims to investigate the impact of social support patterns on mental health during pregnancy for mothers, while also examining whether social trust plays a mediating role in this relationship. The findings of this study will provide empirical evidence and important information for the development of policy options and practical service strategies to enhance maternal social support and perinatal mental health. This study proposes three research hypotheses as follows:
H1. There are several different social support patterns among Chinese mothers based on the multiple social support sources.
H2. Different social support patterns have distinct impacts on perinatal mental health. A pattern with multiple sources and high levels of support has a beneficial effect on perinatal mental health. Oppositely, a pattern with few resources and low level of support has a negative impact on perinatal mental health.
H3. Social trust plays mediating roles in the relationship between different social support patterns and perinatal mental health.
Methods
Participants
This study surveyed three public hospital obstetrics departments located in Wuxi, Jiangsu Province. These hospitals were all tertiary hospitals with strong comprehensive capabilities, and had annual birth rates of more than 10,000, 5,000, and 4,000 respectively. These numbers accurately reflect the delivery situation of obstetrics departments in China. A questionnaire survey was conducted among pregnant women attending three hospitals, with gestational age ranging from 3 weeks to before delivery. The survey was conducted through face-to-face interviews using a quota sampling method. The survey lasted for 6 months during which 1899 questionnaires were distributed and subsequently returned. After eliminating invalid questionnaires, 1705 questionnaires were used in the statistical analysis. Participant characteristics can be found in and .
Measurement
Social support source
This study measured the social support sources available to pregnant women, including medical professionals, family, friends/colleagues, community, pregnant mother’s group, Internet, and Government agencies. Participants were asked to rate the level of support they received from each source on a 6-point Likert scale ranging from 1 (not at all) to 6 (always).
Perinatal mental health
The Body-Mind-Spirit Well-Being Inventory (BMSWBI) scale, developed by Ng et al. [Citation27], was utilized to assess prenatal mental health. Currently, there is no standardized assessment tool in China for assessing perinatal mental health [Citation18]. Considering the somatization of mental health issues in the Chinese population [Citation28], it is crucial to recognize that mental health is a multifaceted system that includes cognition, emotions, values, morals, beliefs, and their interactions with the body. Therefore, to obtain a comprehensive understanding of the mental health status of Chinese mothers, the authors opted for the dynamic systems scale, which is more suitable for this purpose [Citation29]. BMSWBI consists of three dimensions: body health, mind health, and spirit health, and includes 20 items such as headaches, back pain, rib pain, pubic pain, losing direction in life due to pregnancy, feeling happy with everything after pregnancy, and others. Participants rated each item on a 6-point Likert scale, from 1 (strong disagreement) to 6 (strong agreement). The overall reliability coefficient (Cronbach’s a) for the scale was 0.87. The reliability coefficients for the physical, emotional, and mental health sub-factors were 0.82, 0.81, and 0.78, respectively.
Social trust
Social trust was measured using a single question from the World Values Survey (WVS) that assesses social trust. The item was phrased as follows “Generally speaking, would you say that most people can be trusted or that you need to be very careful in dealing with people?” (Social Capital, Trust & Organizational Membership section, q57). Participants were required to assess their level of trust using a 6-point Likert scale, where 1 indicates complete distrust and 6 represents complete trust. A higher scores on the scale signifies a higher levels of social trust.
In this study, socio-demographic data tables were utilized to gather information on pregnant women. The data collected included age, gestational age, marital status, education, employment status, household income, household registration, and number of pregnancies. These variables were later included as control variables in the final regression analysis.
Statistical analyses
The statistical analysis in this study was conducted in two stages. First, latent class analysis was utilized to identify various social support patterns for pregnant women based on the source of social support. An exploratory stepwise addition approach was employed to construct a range of latent class models. The fit index of each model was compared to comprehensively determine the optimal number of latent classes, which represent the number of social support patterns. The indicators used to determine the optimal number of latent classes included AIC (Akaike’s Information Criterion), BIC (Bayesian Information Criterion), adBIC (sample-size-adjusted Bayesian Information Criterion), and Entropy. Smaller values of AIC, BIC, and adBIC indicate better model fit, while a statistically significant VLRT value suggests a better fit for the K model over the K-1 model. An Entropy closer to 1 indicates higher classification accuracy [Citation30]. When considering the representativeness of subgroups, models with a sample proportion of latent class greater than 5% will be preferred [Citation31]. In the second stage, multiple regression models examined the mediating effect of social trust on the relationship between social support patterns and perinatal mental health. The mediating role of social trust was assessed using the Bootstrapping method. Statistical analysis was performed using SPSS 25.0 and Mplus 8.0 software.
Result
Latent class analysis of social support patterns
After a comprehensive comparison of each model fit indicator, it was determined that the optimal number of subgroups for social support patterns in pregnant women is 4 (refer to ). This conclusion was based on the relatively small AIC and BIC values for the 4-class models, the Entropy value approaching 1, and the proportion of samples in subgroups exceeding 5%. The participants exhibited four distinct social support patterns, as depicted in . These patterns were categorized into four classes based on their characteristics. Class 1, comprising 51.1% (N = 872), was labeled as primary relationship-centric support. This class relied mainly on intimate relationships such as family and close friends for social support. Class 2, overall weak support, represented a socially disadvantaged group with a low overall level of social support (N = 265, 15.6%). Class 3, referred to as primary & secondary relationship balanced support (N = 443, 25.9%), received a relatively high and balanced level of support from intimate relationships (family and friends) and social relationships (health care professionals, government, community, Internet, and maternity organizations and so on). Class 4, accounting for 7.4% of the sample (N = 125), was named overall strong support. This group of mothers received substantial support from various sources, making it the most favorable form of social support. It is indicated that there are several different patterns of social support among Chinese mothers, providing support for H1.
Figure 1. Four latent classes of social support.
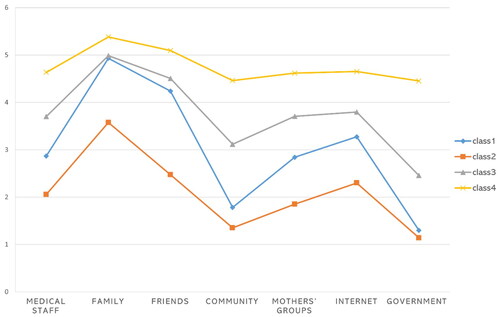
Table 1. Latent class analysis model fit (N = 1705).
Mediating effects of perception of support
Multiple regression analysis models were used to examine the mediating effect of social trust on support patterns affecting perinatal mental health. The analysis of mediating effects model involved encoding the independent variable (social support patterns) as a dummy variable, while the mediating variable (social trust) and the dependent variable (perinatal mental health) were continuous variables. All variables had tolerances above 0.1 (ranging from 0.476 to 0.987) and VIF values below 10 (ranging from 1.013 to 2.101), indicating the absence of multicollinearity issues.
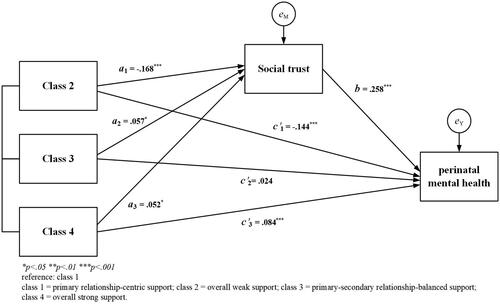
The results of the regression analysis are presented in . Firstly, the analysis revealed a significant effect of social support patterns on social trust (path a), even after controlling for other potential influencing factors. The overall weak support (class 2, B = −0.530, p < 0.001) had lower social trust compared to the primary relationship-centric support (class 1), while the primary & secondary relationship balanced support (class 3, B = 0.161, p < 0.05) and overall strong support (class 4, B = 0.272, p < 0.05) had higher social trust. Secondly, In regard to path b, social trust has a significant positive impact on health during pregnancy, indicating that higher societal trust leads to better health outcomes for pregnant women. Finally, in path c, the overall weak support (class 2, B = −0.305, p < 0.001) negatively influenced perinatal mental health, while the overall strong support (class 4, B = 0.233, p < 0.001) had a positive impact. The primary & secondary relationship balanced support (class 3, B = 0.044, p = 0.547) did not show a statistically significant influence on perinatal mental health (refer to step 1). When both social support patterns and social trust were considered together (refer to step 2), the impact of overall weak support on perinatal mental health was reduced by approximately 23%, and the influence of overall strong support was reduced by about 16%. However, the primary & secondary relationship balanced support still had no significant impact on perinatal mental health. Therefore, the results partially supporting H2.
Table 2. Multiple regression analysis for moderating effect.
To further calibrate the mediating effect of social trust between social support patterns and Perinatal mental health, Bootstrapping was utilized. The bootstrap method estimated the standard errors of the direct and indirect effects of the mediating variables, displaying confidence interval values. If the confidence interval value did not contain 0, it indicated statistical significance of the indirect or direct effect of the mediating variable [Citation32]. The results of the bootstrapping test are shown in : When referencing the primary relationship-centric support group, the path from weak support to social trust to pregnancy had a mediating effect value of −0.081 (95% CI = −1.128 – −0.051), which was statistically significant. Upon inclusion of mediating variables, the direct effect of overall weak support on perinatal mental health was −0.237 (95% CI = −0.333 - −0.133), indicating significance. This indicates that social trust partially mediates the relationship between overall weak support and perinatal mental health. The mediated effect of social trust between primary & secondary relationship balanced support and perinatal mental health was significant at .026 (95% CI = 0.004 − 0.040). The direct effect of primary & secondary relationship balanced support on perinatal mental health was not significant (95% CI = −0.063 − 0.101) when mediating variables were included, suggesting that social trust fully mediated the relationship. A statistically significant mediating effect (coef. = 0.041, 95% CI = 0.004 − 0.040) was observed for the path from overall strong support to perinatal mental health through social trust. Furthermore, the direct effect of overall strong support on perinatal mental health was also significant (coef. =0.199, 95% CI = 0.060 − 0.327). This highlights the partial mediating role of social trust in the relationship between primary & secondary relationship balanced support and perinatal mental health. Therefore, the H3 was supported, indicating that social trust plays a significant mediating role in the association between different patterns of social support and perinatal mental health.
Table 3. Testing mediating effect by bootstrap method.
Discussion and conclusion
This study explores the social support patterns of pregnant women and investigates how social trust mediates the impact of these patterns on perinatal mental health. We classifiedsocial support into four distinct patterns based on their sources: primary relationship-centric support (class 1), overall weak support (class 2), primary & secondary relationship-balanced support (class 3), and overall strong support (class 4). Class1 exhibits the highest number of individuals across all four social support patterns. This finding aligns with the moral and ethical principles of Chinese social behavior, which emphasizes strong bonds based on blood and geographical ties. As a result, informal support, primarily in the form of family and neighborhood support (referred to as primary relationships), is the most prevalent type of support sought by Chinese women [Citation33,Citation34]. However, with the influence of modernization, globalization, and industrialization, traditional Confucian cultural values have been subject to some modifications [Citation35]. In China, the social support structure for pregnant women is gradually shifting from a focus on primary relationships to a more balanced combination of primary and secondary relationships. Thus, the second-highest number of individuals fell into the primary & secondary relationship balanced class.
The mediating effect test revealed that social trust acted as a mediator in the relationship between social support patterns and perinatal mental health. Firstly, it was found that overall weak support had a direct negative effect on perinatal mental health compared to primary relationship-centric support, However, the negative impact of overall weak support on perinatal mental health was found to be mitigated by social trust. Overall strong support (class 4) has significantly higher levels of perinatal mental health (B = 0.233, p < 0.001). Social trust partially mediated the relationship between these two patterns (class 2 & class 4) and perinatal mental health. This This highlights the importance of social trust in enhancing the mental well-being of pregnant women by counteracting the negative effects of insufficient social support. Our study’s findings align with previous research indicating that trust in the social system plays a crucial role in establishing and nurturing social connections among women, fostering a supportive and mutually beneficial environment [Citation24,Citation25].
Secondly, the primary & secondary relationship balanced support had no significant direct effect on perinatal mental health, but it was a crucial distal factor whose influence was entirely mediated by social trust. Compared to a primary relationship-centric support network, a primary & secondary relationship balanced support network has expanded margins. However, whether it can have significant health gain effects depends on women’s trust in the social system. Presently, in Chinese society, there is a shift toward seeking from non-family members in addition to family-centered relationships [Citation16]. Nevertheless, building trust among members of society during the transition from a traditional kinship model to social trust is a challenging task. The lack of trust is further amplified by systemic issues such as inadequacies in public policy reform and the healthcare system. This crisis of social confidence presents a paradoxical situation where the need to expand social support networks coexists with the challenge of fostering trust. The interplay between social trust and personal anxiety is a notable characteristic of contemporary China [Citation36]. These factors not only hinder the positive impact of social support on maternal health during pregnancy but also contribute to various mental health issues.
In the context of today’s globalized world, the rapid development of internet technology has contributed to a notable increase in individuals’ social connections. This phenomenon is not exclusive to Chinese society but is observed across various cultures. However, traditional cultural norms often collide with contemporary social interaction trends, potentially impeding the establishment and efficacy of an individual’s social support system. Therefore, it is crucial to explore how expanded social networks can be optimized to function as effective sources of social support, ultimately leading to positive health outcome. Particularly for pregnant women, who are vulnerable to personal and social pressures, social support from a variety of sources can be effective in improving maternal mental health. Our study indicates that social trust plays a crucial role in mediating the correlation between various social support patterns and perinatal mental health in Chinese women. Consequently, enhancing women’s trust in social institutions and practices, alongside improving both the quantity and quality of their social support networks, is essential. Our study proposes three strategies to achieve these objectives:
First, maternal medical and health services can be effectively promoted and regulated through public health campaigns and policies. By improving maternal satisfaction with access to care and increasing trust in health professionals through quality and standardized healthcare services, mothers are more likely to actively participate in treatment decision-making, adopt positive health behaviors, and achieve better health outcomes. Second, to improve perinatal mental health, it is important to raise public awareness of maternal mental health issues and create a safe and healthy social environment. This can be achieved through various approaches such as maternal health education and promoting therapeutic optimism. Additionally, expanding maternal support networks and connections to social services, both formal and informal can help overcome barriers to seeking diverse social support during the perinatal period. Strengthening social support systems that mothers trust and encouraging open communication about symptoms can effectively promote mental health. Third, to enhance public trust, it is crucial to strengthen integrity systems and improve social and public monitoring mechanisms. Policy makers and government agencies can achieve this by transparently and efficiently delivering health services to the public [Citation37].
There are still some limitations to be addressed in this study. First, the study was conducted only in Wuxi City, Jiangsu Province, and the results may not be fully generalizable given the geographical diversity of China. In future studies, we plan to expand the geographical area of the survey and increase the diversity of the sample in order to further validate the generalizability of the study results. Second, this study utilized cross-sectional data for analysis, which hinders the establishment of causal relationships between variables. Specifically, it is difficult to determine the temporal sequence among the independent, mediating, and dependent variables. To overcome this limitation and improve the credibility of the findings, future research could employ longitudinal data analysis or conduct behavioral experiments with randomized experimental/control groups to validate causal relationships among the factors. This would allow for a more precise examination of the association between social support, social trust, and perinatal mental health. Third, the study employed a regression model-based approach to analyze the mediating effects with multicategory independent variables. While this method offers greater model stability and the ability to include multiple covariates simultaneously to mitigate the impact of confounding variables on the results’ reliability, it has its limitations. For instance, all variables in the regression model were considered manifest variables, potentially underestimating the mediating effect due to the oversight of measurement error. Furthermore, the constraints of using regression models to assess the mediation effect do not permit testing an equivalent model. Given the numerous advantages of structural equation modeling in analyzing mediation models, a future study could consider utilizing structural equation modeling for mediation effect analysis with multicategory independent variables to address these limitations. Fourth, although this study considered a mediating model of social trust, there may still be other mediating or moderating variables (e.g. Stigma, level of perceived support, doctor-patient relationship, family relationship, etc.). Therefore, future research could expand the model of effects on perinatal mental health to provide evidence for improving maternal health.
Ethical approval
This paper has been approved by Jiangnan University Medical Ethics Committee (JNU20211217IRB01). The participants were informed about the purpose of this research and provided written informed consent before administering the questionnaire. To maintain confidentiality, personal identifiers were omitted from the questionnaires and the collected data were stored in a secure, password-protected database without identifiers.
Acknowledgements
We would like to thank the doctors and midwives from the surveyed hospitals, as well as the moms who participated in the study, without whose trust, assistance, and involvement we would not have been able to complete this study. Thanks to our colleagues for their important suggestions on the smooth progression of our project.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Additional information
Funding
References
- Fatori D, Zuccolo PF, Polanczyk GV. A global challenge: maternal depression and offspring mental disorders. Eur Child Adolesc Psychiatry. 2020;29(5):1–9. doi:10.1007/s00787-020-01556-x
- Fisher JR, de Mello MC, Izutsu T, et al. The Ha Noi expert statement: recognition of maternal mental health in resource-constrained settings is essential for achieving the millennium development goals. Int J Ment Health Syst. 2011;5(1):2. doi:10.1186/1752-4458-5-2
- Zhou C, Ogihara A, Chen H, et al. Social capital and antenatal depression among chinese primiparas: a cross-sectional survey. Psychiatry Res. 2017;257:533–539. doi:10.1016/j.psychres.2017.07.058
- Bo H-X, Yang Y, Chen J, et al. Prevalence of depressive symptoms among pregnant and postpartum women in China during the COVID-19 pandemic. Psychosom Med. 2021;83(4):345–350. doi:10.1097/PSY.0000000000000904
- Gelaye B, Rondon MB, Araya R, et al. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and Middle-income countries. Lancet Psychiatry. 2016;3(10):973–982. doi:10.1016/S2215-0366(16)30284-X
- Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. World Psychiatry. 2020;19(3):313–327. doi:10.1002/wps.20769
- Rejnö G, Lundholm C, Öberg S, et al. Maternal anxiety, depression and asthma and adverse pregnancy outcomes – a population based study. Sci Rep. 2019;9(1):13101. doi:10.1038/s41598-019-49508-z
- Gao L, Qu J, Wang AY. Anxiety, depression and social support in pregnant women with a history of recurrent miscarriage: a cross-sectional study. J Reprod Infant Psychol. 2020;38(5):497–508. doi:10.1080/02646838.2019.1652730
- Kang YJ, Kim T, Lee D, et al. Self-rated health trajectory changes according to employment transition: a Korean prospective cohort study. J Occup Environ Med. 2020;62(7):532–537. doi:10.1097/JOM.0000000000001890
- Mori E, Iwata H, Maehara K, et al. Relationship between the mode of conception and depressive symptoms during the first 6 months post-partum in Japan. Reprod Med Biol. 2018;17(3):275–282. doi:10.1002/rmb2.12101
- Shwartz N, Shoahm-Vardi I, Daoud N. Postpartum depression among Arab and Jewish women in Israel: ethnic inequalities and risk factors. Midwifery. 2019;70:54–63. doi:10.1016/j.midw.2018.12.011
- Yu M, Sampson M, Liu Y, et al. A longitudinal study of the stress-buffering effect of social support on postpartum depression: a structural equation modeling approach. Anxiety Stress Coping. 2021;34(6):751–765. doi:10.1080/10615806.2021.1921160
- Kruse JA, Williams RA, Seng JS. Considering a relational model for depression in women with postpartum depression. Int J Childbirth. 2014;4(3):151–168. doi:10.1891/2156-5287.4.3.151
- Negron R, Martin A, Almog M, et al. Social support during the postpartum period: mothers’ views on needs, expectations, and mobilization of support. Matern Child Health J. 2013;17(4):616–623. doi:10.1007/s10995-012-1037-4
- Tang L, Zhu R, Zhang X. Postpartum depression and social support in China: a cultural perspective. J Health Commun. 2016;21(9):1055–1061. doi:10.1080/10810730.2016.1204384
- Li T, Fung HH. Age differences in trust: an investigation across 38 countries. J Gerontol B Psychol Sci Soc Sci. 2013;68(3):347–355. doi:10.1093/geronb/gbs072
- Jiang H, Jin L, Qian X, et al. Maternal mental health status and approaches for accessing antenatal care information during the COVID-19 epidemic in China: cross-sectional study. J Med Internet Res. 2021;23(1):e18722. doi:10.2196/18722
- Zhao H, Zhai J, Zhang Z, et al. Analysis of the influencing factors of mental health of advanced pregnant women with the second child and the investigation of the healthcare needs of these women. Chin J Fam Plann. 2023:31(5):1036.
- Sufredini F, Catling C, Zugai J, et al. The effects of social support on depression and anxiety in the perinatal period: a mixed-methods systematic review. J Affect Disord. 2022;319:119–141. doi:10.1016/j.jad.2022.09.005
- Müller E, Zill JM, Dirmaier J, et al. Assessment of trust in physician: a systematic review of measures. Gupta V, editor. PLoS One. 2014;9(9):e106844. doi:10.1371/journal.pone.0106844
- Li L, Zhu L, Zhou X, et al. Patients’ trust and associated factors among primary care institutions in China: a cross-sectional study. BMC Prim Care. 2022;23(1):1–9. doi:10.1186/s12875-022-01709-8
- Niu G, Liu J. Between trust and distrust: an empirical analysis of citizen’s abnormal trust in doctors. Sociol Stud. 2021;36:157–179.
- WHO. Social determinants of mental health [internet]. Geneva, Switzerland: World Health Organization and Calouste Gulbenkian Foundation.; 2014 [cited 2023 Apr 25]. Available from: https://www.who.int/publications-detail-redirect/9789241506809.
- Zhang W, Yu Y. The effects of social networks, social status and social trust on the mental health of residents. J Fujian Normal Univ (Philosophy and Soc Sci Edition). 2020:100–111. (in Chinese).
- Folland S. An economic model of social capital and health. Health Econ Policy Law. 2008;3(4):333–348. doi:10.1017/S1744133108004532
- Rostila M. Social capital and health in European welfare regimes: a multilevel approach. J Eur Soc Policy. 2007;17(3):223–239. doi:10.1177/0958928707078366
- Ng SM, Yau JKY, Chan CLW, et al. The measurement of body-mind-spirit well-being: toward multidimensionality and transcultural applicability. Soc Work Health Care. 2005;41(1):33–52. doi:10.1300/J010v41n01_03
- Kleinman A. Neurasthenia and depression: a study of somatization and culture in China: report number one of the university of Washington—Hunan medical college collaborative research Project111222. Cult Med Psychiatry. 1982;6(2):117–190. doi:10.1007/BF00051427
- Ng SM, Chan CL, Leung PP, et al. Beyond survivorship: achieving a harmonious dynamic equilibrium using a Chinese medicine framework in health and mental health. Social Work in Mental Health. 2008;7(1–3):62–81. doi:10.1080/15332980802072405
- McLachlan GJ, Peel D. Finite mixture models | wiley [internet]. New York, NY: John Wiley & Sons; 2004. [cited 2023 Apr 25]. Available from: https://www.wiley.com/en-nl/Finite+Mixture+Models-p-9780471006268.
- Wickrama K, Mancini JA, Kwag K, et al. Heterogeneity in multidimensional health trajectories of late old years and socioeconomic stratification: a latent trajectory class analysis. J Gerontol B Psychol Sci Soc Sci. 2013;68(2):290–297. doi:10.1093/geronb/gbs111
- Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods. 2002;7(4):422–445. doi:10.1037/1082-989X.7.4.422
- Ward C, Lin E-Y. There are homes at the four corners of the seas: acculturation and adaptation of overseas Chinese. The Oxford handbook of Chinese psychology. New York, NY: Oxford University Press; 2010. p. 657–677.
- Wong J, Fisher J. The role of traditional confinement practices in determining postpartum depression in women in Chinese cultures: a systematic review of the English language evidence. J Affect Disord. 2009;116(3):161–169. doi:10.1016/j.jad.2008.11.002
- Kulich SJ, Zhang R. The multiple frames of ‘Chinese’ values: from tradition to modernity and beyond. In: Bond MH, editor. Oxford handbook of Chinese psychology [internet]. 1st ed. New York, NY:Oxford University Press; 2012. p. 241–278. [cited 2023 Apr 20]. Available from: https://academic.oup.com/edited-volume/38605/chapter/334713731.
- Fung HH, Lai P, Ng R. Age differences in social preferences among Taiwanese and mainland Chinese: the role of perceived time. Psychol Aging. 2001;16(2):351–356. doi:10.1037/0882-7974.16.2.351
- Taylor LA, Nong P, Platt J. Fifty years of trust research in health care: a synthetic review. Milbank Q. 2023;101(1):126–178. doi:10.1111/1468-0009.12598
Appendices
Appendix Figure 1. Mediating effect model.
Appendix Table 1. Participants’ socio-demographic characteristics.
Appendix Table 2. Participants’ social support, social trust and perinatal mental health status.