
Abstract
Objective
To study changes in supraspinatus tendon elasticity after a 448 kHz capacitive resistive monopolar radiofrequency (CRMR) intervention in professional badminton players.
Design
Double-blinded randomized clinical trial.
Setting
All participants were recruited in a private care practice. Participants were randomized to receive either a CRMR treatment (n = 19) or placebo (n = 19).
Subjects
Professional badminton players (n = 38).
Intervention
A total of nine intervention (three per week) with CRMR at 448 kHz were carried out in the experimental group. The same intervention without an active CRMR current was carried out in the control group.
Main measures
Mean values of three different regions of the supraspinatus tendon were reported at baseline (T1), immediately after the intervention (T2) and one week after the end of the whole intervention program (T3) using quantitative ultrasound strain elastography (SEL).
Results
There were statistically significant differences in the supraspinatus tendon elasticity immediately after the intervention (p= <.001) and one week after the end of the whole intervention program (p=.001).
Conclusion
CRMR at 448 kHz produces significant changes in supraspinatus tendon elasticity after an intervention program of three weeks and those changes last for a week when compared to control group. Clinical trial registration: NCT04273633 (ClinicalTrials.gov).
Introduction
Radiofrequency is a well-known technology that has been widely used in clinical settings. Tecartherapy is one of the treatments that uses radiofrequency. It is based on a device that applies a 448 kHz electric current that flows when a voltage difference is created through the body using two electrodes which are placed in diverse areas of the human body. The current, also known as capacitive resistive monopolar radiofrequency (CRMR), uses an active circular electrode that can be moved during the treatment and creates the stimulating electrical voltage, and a passive rectangular electrode which remains at the same place throughout the treatment process as the returning electrode [Citation1–3]. The capacitive electrode concentrates its energy in tissues with a higher electrolytic content (soft tissue mainly) while the resistive electrode concentrates its energy in higher resistance tissues such us bones, joints or tendons. Furthermore, both types of electrode can be used either in a thermal or non-thermal dose, based on the patient’s feedback on their perception of heating as well as on the increase of the skin temperature in respectively [Citation1,Citation2,Citation4].
CRMR has been used to treat different musculoskeletal disorders, such as osteoarthritis of the knee [Citation2], cervico-brachial pain [Citation3] and lumbago [Citation5]. Moreover, other effects have been described after a CRMR application such as an increased effect on hemoglobin saturation [Citation4] and immunological responses [Citation6,Citation7]. Shoulder pain is a very common pathology which is currently placed as the third most common musculoskeletal disorder after low back pain and neck pain [Citation8,Citation9]. Many different shoulder conditions have been described in both general and sports population [Citation10]. Within this latter group, racket sports are very common when reporting shoulder conditions, such as in badminton, where players usually suffer from both upper and lower limb injuries [Citation11]. With regard to shoulder conditions, different strategies have been used for their treatment, but better prevention strategies to avoid such injuries remain challenging [Citation12]. The elasticity of the tissue is crucial to keep the musculoskeletal system safe and functional. Based on this, research on methods which aim to reach this goal is necessary, and the use of hyperthermia appears to be a promising technique. However, a gap remains in current research about how CRMR affects the tendon elasticity being assessed by ultrasound elastography (USE).
Strain elastography (SEL) is an innovative method which improves the assessment and diagnosis in tendon healing [Citation13]. SEL defines the stiffness of both the regions of interest and the surrounding tissues [Citation14,Citation15], therefore, it goes beyond macroscopic changes and permits the evaluation of the mechanical tendon properties [Citation16]. SEL and MRI imaging techniques have been found to present significant associations in patients with supraspinatus tendinopathy [Citation17,Citation18], as well as significant correlations with clinical tests and questionnaires in patients with supraspinatus tendon tears [Citation19]. Furthermore, SEL is able to detect increased stiffness in the supraspinatus tendon elasticity and muscle elasticity in healthy participants [Citation20]. The validity of SEL in the supraspinatus tendon has been shown [Citation17–21]. Mean values of supraspinatus tendon elasticity are not currently established given the novelty of the SEL technique, nevertheless, it is understood to be around 3.75 in healthy subjects and 3.55 in subjects with supraspinatus tendinopathy according to the latest studies, with differences between studies possibly explained by age and sex [Citation21–23]. With regard to differences in SEL tendon values, the explanation may be based on differences in blood perfusion and consequent increased temperature, with stiffer tissues presenting higher values and softer tissues lower values [Citation13,Citation16,Citation24].
The physiological effects of hyperthermia on soft tissues are well established, showing changes in both superficial and deep tissues, at cellular and systemic levels [Citation1–3]. Moreover, hyperthermia can also change the nature of connective tissues by altering the properties of tendons and ligaments [Citation1–3]. The extent of the physiological effect may vary depending on the level of exposure [Citation25]. Some of these reactions, such as the increase in blood perfusion, are known to be linked to a temperature increase, but others, such as the enhanced cell proliferation, seem to be mainly related to the passage of the current [Citation26–28].
Therefore, the hypothesis of the present study is that the application of 448 kHz CRMR can produce changes in supraspinatus tendon elasticity measured by SEL. This can be explained through the relationship between vascularization, viscoelasticity and temperature increase [Citation24,Citation27]. Furthermore, it is currently known that there are structural changes and alterations in the tendon morphology of healthy people when assessed by ultrasound [Citation29]. These alterations may indicate weak points of the soft tissue that is likely to suffer from injury, although pain may not be present [Citation13,Citation29]. However, such changes may be better evaluated by tendon elasticity measurements such as SEL [Citation13,Citation21]. The confirmation of changes in supraspinatus tendon elasticity after the application of 448 kHz CRMR may elicit new approaches for both the prevention and the rehabilitation of shoulder injuries.
The aim of the study is to assess SEL changes in supraspinatus tendon after 448 kHz CRMRF treatment in healthy professional badminton players.
Materials and methods
Design
This is a double-blinded, randomized, placebo-controlled clinical trial with blinding of participants and researcher to active or placebo CRMR intervention.
Setting
Participants were recruited in a private care practice in Malaga, Spain. Referrals were informed of the trial through formal meetings and trial information sheets. Informed written and verbal consent were obtained from all participants before enrollment and baseline demographic and clinical data were collected. The study was approved by a Medical Research Ethics Committee (984/CEIH/2019), registered in ClinicalTrials.gov (NCT04273633) and conducted in accordance with the Declaration of Helsinki. This study is reported in line with the standard protocol items of the CONSORT Statement [Citation30,Citation31].
Participants
Participants were screened to determine whether they met the following inclusion and exclusion criteria.
Inclusion criteria
Participants (i) had to be aged between 18 and 64 years; (ii) to be healthy badminton players; and (iii) without shoulder pain or shoulder injuries within the last year.
Exclusion criteria
(i) Participants presenting any painful and inflammatory process; (ii) neurological or (iii) orthopedic disease which can alter balance, hearing and vision, or cognitive impairment, which might impact on their ability to answer questions.
Allocation
Participants were randomized to receive either a hyperthermia treatment or placebo using a random-number generator and concealed allocation by a researcher assistant. An experienced physiotherapist who collaborated in the research carried out all the interventions. Participants and the statistician were blinded to the allocation of the subjects.
Patients were required not to receive or participate in any other study or treatment regime during the study period.
The interventions are described following Template for Intervention Description and Replication (TIDieR) Checklist recommendations [Citation19].
Sample size calculation
The sample size was determined by application of the EPIDAT program. Based on previous studies, using an average of 1.1 mm as the expected supraspinatus mean difference and the corresponding standard deviation of 1.0 mm, significance set at α = 0.05, a power analysis for t tests indicated a simple size of n = 19 per group for 90% power [Citation32–34].
Intervention description
Experimental group
Patients received three 448 kHz CRMR interventions weekly for 3 weeks, having a total of nine interventions. The patient’s position was lying laterally with the shoulder of interest on the upper side, so that the main neural and vascular structures were stimulated [Citation27,Citation35]. CRMR at 448 kHz was delivered using ‘INDIBA® Activ 8 equipment, with a peak power of 200 W and 450 VA. Capacitive (CAP) and resistive (RES) waves, using metallic electrodes via a coupling medium were applied. The CAP mode was delivered as a thermal dose (according to patient feedback on his/her perception of heat, with the perception expected by the patient being eight out of 10) in the muscles around the shoulder. CAP mode was used for a total of 10 min for all shoulder muscles. The RES mode was delivered as a thermal dose (hyperthermia) applied in a continuous wave. The RES mode was delivered for 10 min, following manufacturer’s indications. The return electrode was held by the patient in the hand on the side of the treated shoulder.
Control group
Participants received both the same number of interventions and time of duration in each session. The whole intervention program was replicated, nevertheless, the intervention was only manual using the electrodes but without any active current.
SEL measurements
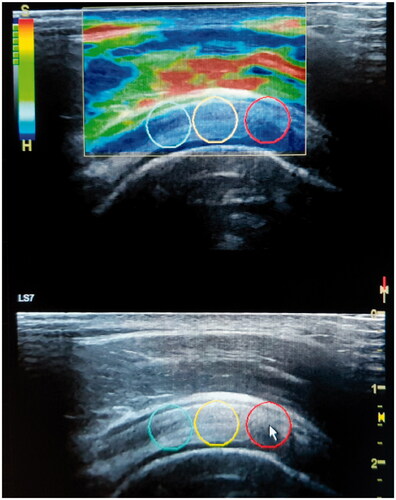
All measurements were performed with the Logiq S7 using a 15 MHz linear probe (GE Healthcare, Milwaukee, WI) by a physiotherapist expert in musculoskeletal ultrasound imaging with 9 years of experience in ultrasound imaging. The SEL was obtained with the patient sitting in an erect posture with the arm internally rotated, with the patient's palm placed over their iliac wing or ‘back pocket’ with the elbow flexed and directed medially [Citation36]. A transverse glide was then performed at the site to determine the exact position where the observer evaluated the tendon thickness at its maximum. Measurements were taken 2 cm laterally from the biceps tendon, where supraspinatus tendon thickness is usually assessed [Citation9,Citation37]. At this point, the tissue was compressed approximately 2–5 mm [Citation15], and a software incorporated quality control (expressed as one to five green bars being displayed, with five bars being the most acceptable) was used to evaluate the recommended compression size. The exact raw strain value (0–6; with 0 being softest and 6 being the hardest tissue) was calculated using a 5 mm circular region in a soft part of the area of interest, as indicated by the manufacturer’s instructions and shown in previous studies [Citation21]. There were three different points of measurements to evaluate the tendon to get the most complete information.
A mean of the three measured areas at each point (being a total of nine measurements) of the supraspinatus tendon was calculated in order to minimize intra-observer variation. Only sequences with the highest image quality (with green bars on the quality assessment) were used as recommended by the manufacturer ().
Figure 1. Supraspinatus tendon elasticity measurement by quantified elastography.
Statistical analysis
SPSS® Statistics version 21.0 (IBM, Chicago, IL) was used for all analyses. The Shapiro–Wilk test was used to verify data distribution normality. To compare the two groups (CRMR intervention and control groups) at baseline and follow-ups regarding clinical characteristics, a three-way repeated measures ANOVA was conducted, with three levels corresponding to each time of assessment (T0, T1 and T2), and the two intervention groups as independent factors. A p values <.05 was considered to be statistically significant. Bonferroni’s adjustments for multiple comparisons were used. Between group effect sizes for all quantitative variables were measured with the Cohen d coefficient. An effect size greater than 0.8 was considered large, around 0.5 moderate and less than 0.2 small [Citation30].
Results
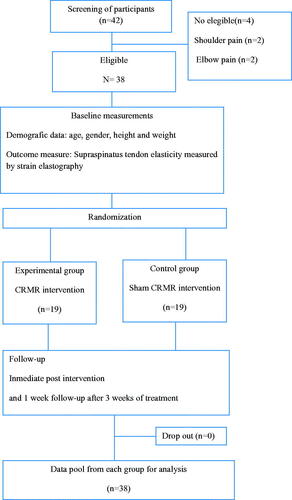
The recruitment included a total of 42 participants, with eight participants who did not follow the inclusion criteria because of shoulder (n = 2) and elbow pain (n = 2). A final number of 38 participants were enrolled in the experimental (n = 19) and the control group (n = 19) and completed the baseline assessment. All the participants were assessed at baseline (T0), immediately after receiving the whole 3-week intervention (T1) and one week after the end of the program intervention (T2) (). After the recruitment of the necessary sample size and once comparisons between groups before and after the intervention were analyzed, the study reached its goal and was ended. The control group was not expected to be harmed by being given the placebo intervention (without temperature), whereas the control group may present dermatological responses due to the hyperthermia used during treatment. This information was reported through formal meetings and trial information sheets. None of the participants suffered from any harm during the study.
Figure 2. Flow diagram of participants.
Sample characteristics
Demographic characteristics are shown in . There were no significant differences between groups in terms of age, gender, height, weight and supraspinatus tendon elasticity.
Table 1. Baseline demographic characteristics.
Between groups differences on supraspinatus tendon elasticity
Comparisons between groups are described in detail in . There were statistically significant differences in the supraspinatus tendon elasticity immediately after the intervention program (T1) and one week after its end (T2).
Table 2. Between groups differences on supraspinatus tendon elasticity at baseline, after the intervention and at one week follow-up (95%CI).
Discussion
Statistically significant differences in supraspinatus tendon elasticity were found between groups after the intervention treatment program and one week after the intervention.
Previous studies have reported the benefits of using CRMR for musculoskeletal disorders [Citation2,Citation3,Citation5], while others have shown supraspinatus tendon properties and its assessment by elastography [Citation17–21]. However, this study is the first analyzing changes in tendon elasticity after a radiofrequency intervention (hyperthermia), therefore comparisons with other studies are difficult. Values of supraspinatus tendon elasticity assessed by SEL have been shown in both healthy and pathological conditions (rotator cuff tendinopathy) [Citation21,Citation22], which are in line with ours.
It is of great importance to carry out studies in healthy subjects to better understand what normal physiological responses should be taking place when using CRMR. In this regard, the current can generate warming of deep muscle tissues and in turn improve hemoglobin saturation, an increase in deep and superficial blood flow, vasodilation and increase in temperature [Citation24,Citation38], causing responses such as increased blood perfusion and therefore a temperature increase, which can explain viscoelastic changes in tendon measured by SEL.
On the other hand, healthy supraspinatus tendon has been shown to present impoverished vascular supply at the insertion region, which may lead to tissue degeneration [Citation27,Citation39]. This fact, in addition to a compressive factor in the vessel which lasts over time and comes from myofascial and/or metabolic factors, may hinder tissue regeneration [Citation40]. The provision of techniques which enhances blood perfusion and decreases myofascial and metabolic stress as well as its accumulative damage effect, may keep the tissue healthy and prevent it from the development of degeneration [Citation4].
To make changes in tendon properties by using hyperthermia can be of huge importance, since it may be possible to improve tendon quality. This would mean better adaptation to loads and proper directions in collagen fibers, as well as to induce adequate immunological responses in order to modulate inflammation when repetitive activities or potential injuries occur. These hypothesis are based on several studies:
Use of hyperthermia at 448 kHz to stimulate cell proliferation, collagen remodulation and increased quality of the tissue.
Proliferation of precursor cells is crucial in tissue regeneration. Mesenchymal stem cells are present in almost all tissues and play a key role in the proliferative phase. Electrical stimulation has been shown to influence the regulation of morphological and phenotypic processes involved in the differentiation and proliferation of different cell types. The use of CRMR at 448 kHz has been shown to induce upregulation of the mitogen-activated protein kinase – extracellular signal-regulated kinases 1 and 2 (MAPK – ERK1/2) pathway and promoting proliferation in mesenchymal stem cells. Furthermore, the use of heat stress to improve extracellular matrix remodeling has been shown. This can be explained through the modulation of the MMP-2/TIPM-2 ratio and the decrease of the TGF-b1 protein expression, which has been associated with the induction of heat shock protein 72 expression among others biomarkers. This matrix remodeling means to increase procollagen type I instead of procollagen type III [Citation26,Citation41–44].
Use of hyperthermia to initiate an immunological response
Several studies have analyzed the effects of the immune response after a stimulation with hyperthermia. Since mesenchymal stem cells directly intervene in the control of inflammatory processes by secreting anti-inflammatory interleukins in the damaged region, CRMR might be useful in anti-inflammatory responses through its ability to increase the local population of mesenchymal stem cells. This would mean a better modulation of inflammatory responses and therefore better adaptation to loads and repetitive movements [Citation6,Citation7,Citation26].
This study presents strengths that should be mentioned. Similar demographic characteristics in our two groups were present, and the study is the first to report changes in the supraspinatus tendon elasticity after a intervention with CRMR at 448 kHz. Moreover, a careful assessment was carried out using SEL by an expert in musculoskeletal ultrasound imaging, assuring the high quality of the values obtained. Finally, the vascularity of the subacromial bursa and rotator cuff tendons is a key factor in the pathogenesis of subacromial bursitis and impingement syndrome, rotator cuff tendinitis, and rotator cuff tears, and also alters the ratio between subacromial space and supraspinatus tendon [Citation45]. Hence, we decided that the patient should lie laterally with the shoulder of interest on the upper side, where the main vascular and neural structures were stimulated [Citation35]. However, the present study has some limitations that should be recognized. First, the person who carried out the treatment was aware that the subject was either from a control or experimental group, so triple-blinding was not achieved. Second, the follow up measurements were only in the short-term and so mid- and long-term assessments should be done to strengthen the study. Third, the presented findings have relevant clinical implications. Based on our results, the application of CRMR at 448 kHz around the whole shoulder makes changes in the supraspinatus tendon elasticity, in contrast to common massage using the same electrodes without any current. As explained before, this may improve tendon quality not only structurally but also immunologically. The addition of this kind of intervention within sport training, as well as to the active therapeutic exercise in those suffering from tendinopathy, may increase their improvements. Also, differences in SEL supraspinatus tendon between healthy subjects and those with shoulder pain may be explained based on differences in blood perfusion and its consequent increased temperature, which leads to an increased viscoelasticity and therefore a decreased SEL value. This may help in shoulder assessment in a clinical setting. However, this is only speculation and more studies in this line are needed to corroborate these findings. Furthermore, studies analyzing changes in the type of collagen and inflammatory cell populations after a CRMR intervention are needed.
Conclusion
The intervention with CRMR at 448 kHz produces changes in supraspinatus tendon elasticity which can last for a week. This may be useful to improve both structural and functional tendon quality. Further studies assessing changes in the short-, mid- and long-term, not only in supraspinatus elasticity but also in neuro-endocrine-immune pathways, are necessary.
Acknowledgements
The authors express our gratitude to all individuals that have kindly collaborated with our research project.
Disclosure statement
The authors report no conflicts of interest.
References
- Spottorno J, Gonzalez de Vega C, Buenaventura M, et al. Influence of electrodes on the 448 kHz electric currents created by radiofrequency: a finite element study. Electromagn Biol Med. 2017;36(3):306–314.
- Kumaran B, Watson T. Treatment using 448 kHz capacitive resistive monopolar radiofrequency improves pain and function in patients with osteoarthritis of the knee joint: a randomised controlled trial. Physiotherapy. 2019;105(1):98–107.
- Takahashi K, Suyama T, Takakura Y, et al. Clinical effects of capacitive electric transfer hyperthermia therapy for cervico-omo-brachial pain. J Phys Ther Sci. 2000;12(1):43–48.
- Tashiro Y, Hasegawa S, Yokota Y, et al. Effect of capacitive and resistive electric transfer on haemoglobin saturation and tissue temperature. Int J Hyperthermia. 2017;33(6):696–702.
- Takahashi K, Suyama T, Onodera M, et al. Clinical effects of capacitive electric transfer hyperthermia therapy for lumbago. J Phys Ther Sci. 1999;11(1):45–51.
- Mace TA, Zhong L, Kokolus KM, et al. Effector CD8+ T cell IFN-γ production and cytotoxicity are enhanced by mild hyperthermia. Int J Hyperthermia. 2012;28(1):9–18.
- Knippertz I, Stein MF, Dörrie J, et al. Mild hyperthermia enhances human monocyte-derived dendritic cell functions and offers potential for applications in vaccination strategies. Int J Hyperthermia. 2011;27(6):591–603.
- Luime J, Koes B, Hendriksen I, et al. Prevalence and incidence of shoulder pain in the general population: a systematic review. Scand J Rheumatol. 2004;33(2):73–81.
- Navarro-Ledesma S, Struyf F, Falla D, et al. Non-traumatic chronic shoulder pain is not associated with changes in rotator cuff interval tendon thickness. Clin Biomech. 2019;63:147–152.
- Lewis JS. Rotator cuff tendinopathy: a model for the continuum of pathology and related management. Br J Sports Med. 2010;44(13):918–923.
- Bravo-Sánchez A, Abián-Vicén J, Jiménez F, et al. Influence of badminton practice on calcaneal bone stiffness and plantar pressure. Phys Sportsmed. 2020;48(1):98–104.
- Asker M, Brooke HL, Waldén M, et al. Risk factors for, and prevention of, shoulder injuries in overhead sports: a systematic review with best-evidence synthesis. Br J Sports Med. 2018;52(20):1312–1319.
- Prado-Costa R, Rebelo J, Monteiro-Barroso J, et al. Ultrasound elastography: compression elastography and shear-wave elastography in the assessment of tendon injury. Insights Imaging. 2018;9(5):791–814.
- Dietrich C, Barr R, Farrokh A, et al. Strain elastography – how to do it? Ultrasound Int Open. 2017;3(4):E137–E149.
- Garra BS. Elastography: history, principles, and technique comparison. Abdom Imaging. 2015;40(4):680–697.
- Fusini F, Langella F, Busilacchi A, et al. Real-time sonoelastography: principles and clinical applications in tendon disorders. a systematic review. Muscles Ligaments Tendons J. 2017;7(3):467–477.
- Lee SU, Joo SY, Kim SK, et al. Real-time sonoelastography in the diagnosis of rotator cuff tendinopathy. J Shoulder Elb Surg. 2016;25(5):723–729.
- Seo JB, Yoo JS, Ryu JW. Sonoelastography findings of supraspinatus tendon in rotator cuff tendinopathy without tear: comparison with magnetic resonance images and conventional ultrasonography. J Ultrasound. 2015;18(2):143–149.
- Tudisco C, Bisicchia S, Stefanini M, et al. Tendon quality in small unilateral supraspinatus tendon tears. Real-time sonoelastography correlates with clinical findings. Knee Surg Sports Traumatol Arthrosc. 2015;23(2):393–398.
- Muraki T, Ishikawa H, Morise S, et al. Ultrasound elastography-based assessment of the elasticity of the supraspinatus muscle and tendon during muscle contraction. J Shoulder Elb Surg. 2015;24(1):120–126.
- Brage K, Hjarbaek J, Kjaer P, et al. Ultrasonic strain elastography for detecting abnormalities in the supraspinatus tendon: an intra- and inter-rater reliability study. BMJ Open. 2019;9(5):e027725.
- Brage K, Hjarbaek J, Boyle E, et al. Discriminative and convergent validity of strain elastography for detecting tendinopathy within the supraspinatus tendon: a cross-sectional study. JSES Int. 2020;4(2):310–317.
- Brage K, Juul-Kristensen B, Hjarbaek J, et al. Strain elastography and tendon response to an exercise program in patients with supraspinatus tendinopathy: an exploratory study. Orthop J Sport Med. 2020;8:1–11.
- López-de-Celis C, Hidalgo-García C, Pérez-Bellmunt A, et al. Thermal and non-thermal effects off capacitive-resistive electric transfer application on the Achilles tendon and musculotendinous junction of the gastrocnemius muscle: a cadaveric study. BMC Musculoskelet Disord. 2020;21(1):46.
- Kumaran B, Watson T. Thermal build-up, decay and retention responses to local therapeutic application of 448 kHz capacitive resistive monopolar radiofrequency: a prospective randomised crossover study in healthy adults. Int J Hyperthermia. 2015;31(8):883–895.
- Hernández-Bule ML, Paíno CL, Trillo MÁ, et al. Electric stimulation at 448 kHz promotes proliferation of human mesenchymal stem cells. Cell Physiol Biochem. 2014;34(5):1741–1755.
- Fenwick SA, Hazleman BL, Riley GP. The vasculature and its role in the damaged and healing tendon. Arthritis Res. 2002;4(4):252–260.
- Rodríguez-Sanz J, Pérez-Bellmunt A, López-de-Celis C, et al. Thermal and non-thermal effects of capacitive–resistive electric transfer application on different structures of the knee: a cadaveric study. Sci Rep. 2020;10(1):1–9.
- McAuliffe S, McCreesh K, Purtill H, et al. A systematic review of the reliability of diagnostic ultrasound imaging in measuring tendon size: is the error clinically acceptable? Phys Ther Sport. 2017;26:52–63.
- Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 Explanation and Elaboration: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010;63(8):e1–e37.
- Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016;2(1):1–32.
- Michener LA, Subasi Yesilyaprak SS, Seitz AL, et al. Supraspinatus tendon and subacromial space parameters measured on ultrasonographic imaging in subacromial impingement syndrome. Knee Surg Sports Traumatol Arthrosc. 2013;23(2):1–7.
- Joensen J, Couppe C, Bjordal JM. Increased palpation tenderness and muscle strength deficit in the prediction of tendon hypertrophy in symptomatic unilateral shoulder tendinopathy: an ultrasonographic study. Physiotherapy. 2009;95(2):83–93.
- Cholewinski JJ, Kusz DJ, Wojciechowski P, et al. Ultrasound measurement of rotator cuff thickness and acromio-humeral distance in the diagnosis of subacromial impingement syndrome of the shoulder. Knee Surg Sports Traumatol Arthrosc. 2008;16(4):408–414.
- Põldoja E, Rahu M, Kask K, et al. Blood supply of the subacromial bursa and rotator cuff tendons on the bursal side. Knee Surg Sports Traumatol Arthrosc. 2017;25(7):2041–2046.
- Beggs I, Bueno A, Cohen M, et al. Musculoskeletal ultrasound technical guidelines I. Shoulder. European Society of MusculoSkeletal Radiology; 2015. http://www.essr.org/html/img/pool/shoulder.pdf
- Corazza A, Orlandi D, Fabbro E, et al. Dynamic high-resolution ultrasound of the shoulder: how we do it. Eur J Radiol. 2015;84(2):266–277.
- Rodríguez-Sanz J, López-de-Celis C, Canet-Vintró M, et al. Are the effects in temperature and current flow dependent on the areas of electrode application of capacitive-resistive electric transfer on the shoulder? A cadaveric study. Mater Sci. 2021;7:1–13.
- Codman EA, Akerson IB. The pathology associated with rupture of the supraspinatus tendon. Ann Surg. 1931;93(1):348–359.
- Garving C, Jakob S, Bauer I, et al. Impingement syndrome of the shoulder. Dtsch Arztebl Int. 2017;114(45):765–776.
- Hirunsai M, Srikuea R, Yimlamai T. Heat stress promotes extracellular matrix remodelling via TGF-β1 and MMP-2/TIMP-2 modulation in tenotomised soleus and plantaris muscles. Int J Hyperthermia. 2015;31(4):336–348.
- Dams SD, de Liefde-van Beest M, Nuijs AM, et al. Pulsed heat shocks enhance procollagen type I and procollagen type III expression in human dermal fibroblasts. Skin Res Technol. 2010;16:354–364.
- Dams SD, De Liefde-van Beest M, Nuijs AM, et al. Heat shocks enhance procollagen type I and III expression in fibroblasts in ex vivo human skin. Skin Res Technol. 2011;17(2):167–180.
- Trillo MÁ, Martínez MA, Úbeda A. Effects of the signal modulation on the response of human fibroblasts to in vitro stimulation with subthermal RF currents. Electromagn Biol Med. 2020;40(1):1–9.
- Navarro-Ledesma S, Fernandez-Sanchez M, Luque-Suarez A. Differences in supraspinatus occupation ratio between the symptomatic, the contralateral asymptomatic shoulder and control subjects. Medicine (Baltimore). 2021;100(6):e24734.