
ABSTRACT
Background
Most aphasia research is published in international, peer-reviewed journals in a format that is inaccessible for people with aphasia (PWA). Video presents an ideal format for disseminating information to PWA in an accessible digital format. No research has explored the preferred format for aphasia research videos from the perspectives of PWA.
Aims
To explore the format preferences of PWA for aphasia-accessible research videos.
Methods and procedures
The study involved three stages; all used a semi-structured focus group design. Stage 1 (n = 16 PWA) developed the topic guide. PWA shared opinions about which questions they considered important for Stage 2 interview questions. Stage 2 gathered the votes of PWA (n=40) using these questions. Stage 3 (n = 6 PWA) reviewed the voting results of Stage 2 and collected opinions from PWA about an example video that adhered to the identified preferences. Data analysis for all stages used descriptive statistics (e.g., counts) and qualitative content analysis.
Outcomes and results
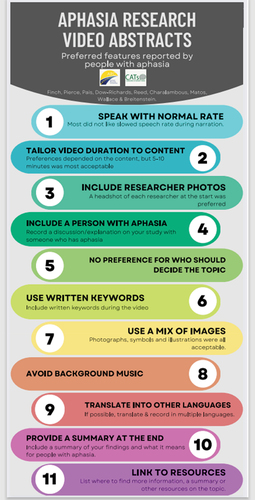
We identified 11 consumer-informed preferences for aphasia-accessible research videos: 1-Speak with normal rate; 2-Tailor video duration to content: 5-10 minutes was most acceptable; 3-Include researcher photos; 4-Use written keywords; 5-Use a mix of images; 6-Include a PWA; 7-No preference for deciding topic; 8-Avoid background music; 9-Provide a summary at the end; 10-Translate into other languages; and 11-Link to resources.
Conclusion
These preferences should guide the development of aphasia-accessible research videos, assisting researchers to bridge the evidence-knowledge gap in the aphasia community. Further research is required, including with non-English participants and family members of PWA.
Introduction
There is a substantial body of research into aphasia assessment and interventions, yet most of this research is published in international, peer-reviewed journals in a format that is inaccessible for non-professionals – in particular, people with aphasia (PWA) and their families. The complex nature of the academic language used in these journal articles is a major barrier to keeping them informed about the latest research. Thus, many PWA and their families lack sufficient knowledge to make informed decisions about their own healthcare (Brady et al., 2013).
To reduce the information barriers experienced by PWA and their families, previous research has developed guidelines and criteria to make information more accessible to this population (termed “aphasia-friendly” or “aphasia-accessible” information) (Brennan et al., Citation2005; Rose et al., Citation2003; Rose et al., Citation2011). This valuable body of work has focused predominantly on written information (Brennan et al., Citation2005; Rose et al., Citation2003; Rose et al., Citation2011) and website/graphics guidelines (Language-Light UX, http://languagelightux.org/). No research has explored the preferences of PWA for other non-written formats such as research videos. Given the high prevalence of reading difficulties in aphasia (Webster et al., Citation2013), video coupled with audio may be an ideal format for disseminating information to PWA. Unfortunately, there is no information about the features of a ‘good’ research video abstract from the perspective of PWA (i.e., aphasia-accessible videos). Thus, there is an urgent need to explore their preferences for video format.
Aim
The primary aim of this qualitative study was to explore the format preferences of PWA for aphasia-accessible aphasia research videos.
Materials and methods
Design: A multi-stage qualitative study design was used with three stages of online semi-structured focus groups. As per Pearl and Cruice (Citation2017), it was critical that PWA were integrally involved to ensure that the final output (format preferences) genuinely reflected the needs of the end users (PWA). To ensure the right questions were asked about the research videos, the stage 1 focus groups sought advice from PWA about which questions to ask about aphasia research videos. In stage 2, these questions were asked in focus groups to determine PWA’s preferences for the format of aphasia research videos. An exemplar video, based on the preferences identified in Stage 2, was then presented in stage 3 and PWA provided their perspectives about it.
Research Team
Our multi-national, multi-stakeholder research team represented a collaboration between PWA and their families, speech-language pathologists and aphasia researchers and was a partnership between the Collaboration of Aphasia Trialists (CATs; an international group of aphasia researchers https://www.aphasiatrials.org) and Aphasia Recovery Connection (ARC; a US-based international non-profit organisation offering online communication platforms for PWA and their families https://aphasiarecoveryconnection.org).
Participants
English-speaking PWA were recruited via email snowball sampling of the research team’s networks and posting on CATs and ARC social media (e.g., Facebook, Twitter). Inclusion criteria were: (1) aged at least 18 years; (2) self-identified diagnosis of aphasia, (3) chronic phase (at least 6 months post onset of a stroke); (4) no hearing or vision difficulties that would interfere with communication (self-reported by the PWA). The exclusion criterion was: (1) self-identified inability to participate in a focus group with communication support due to severe cognitive-linguistic impairments.
Participants could participate in more than one stage of the project as each stage had a different focus. Participant demographic information, along with aphasia severity is presented in . Aphasia severity was rated offline using the ‘Aphasia Severity Rating Scale’ (ASRS from the Diagnostic Aphasia Examination, BDAE; Goodglass et al., Citation2000) based on a communication sample from each focus group.
Table 1. Participant demographic and aphasia severity information
Procedure
Ethical approval was obtained from The University of Queensland Human Research Ethics Committee (2021/HE001575). All focus groups were conducted online and were moderated by 1-2 research team members (all of whom were experienced in facilitating communication with PWA). Each focus group lasted approximately one hour. All participants gave verbal consent to participate. The general format of all focus groups involved: discussion of the study aims and procedure, watching 2-3 minutes of short aphasia research videos in different formats to provide context (the videos are available here: Video Abstracts of Newly Published Aphasia Research - YouTube; Aphasia Answers from CATs and ARC: Introduction - YouTube), and responding to the study topic guide questions. The draft topic guide was developed by the research team to provide a series of visual, structured questions to guide PWA’s perceptions about what might be important in aphasia-accessible videos (e.g., “Do you like a photograph of the researchers at the start?” – With options: Yes, No, Don’t know/Unsure). PWA were encouraged to explain their opinions and/or add additional information considered pertinent. All focus groups were video recorded for analysis and checking.
Following each focus group, two members of the research team independently rated participants’ aphasia severity on the ASRS, then met together to discuss their ratings and resolve any discrepancies.
Stage 1: The purpose of Stage 1 was to develop the topic guide for Stage 2. Participants were shown a list of potential questions and asked whether each question was a good question to ask PWA about aphasia research videos (e.g., Should we ask “What talking speed is good?” with options: Yes, No, Don’t know/Unsure). Participants were shown three aphasia research videos produced by international aphasia researchers on a topic of their expertise. The videos were invited by the CATs Dissemination team and differed in length, format (presentation style versus interactive conversation), talking speed, number and types of images used, use of accompanying words, inclusion of the speaker’s head and a list of resources. During the focus group, participants had the opportunity to suggest additional or modify existing questions. After the focus group, participants received an aphasia-accessible summary of all responses, with the invitation to suggest further modifications. Following completion of the focus groups and after the opportunity to provide further feedback had ended, questions with agreement from PWA (defined as a vote of “yes” by ≥ 75% of participants, with the exception of “Should PWA be involved in the video?” which was included by the research team as 50% of participants voted yes for inclusion while the remaining 50% voted don’t know/unsure) were incorporated into the topic guide for Stage 2.
Stage 2: Stage 2 aimed to gather the opinions of PWA about their preferred format of aphasia videos using the questions from Stage 1. Participants watched three aphasia research videos (to provide examples of the different features of videos such as length, use of icons/images, presentation vs. interview formats. Two videos were distinct from stage 1, one video was identical in stages 1 and 2; Aphasia Answers from CATs and ARC: Introduction - YouTube). PWA responded to the questions using 3-point response scales (e.g., “Do you like keywords?” – With options: Yes, No, Don’t know/Unsure. Note: The video duration question was a 5-point scale to provide more fine-grained response options. For 4 questions in Stage 2 participants requested an additional response option – See ).
Table 2. Questions and participant responses during the three focus group stages
Stage 3: Preferences identified in Stage 2 were used by a research team member (JP) to develop an aphasia-accessible research video (available at https://youtu.be/rqxItoSGH4c). PWA were shown the results (response frequencies from Stage 2) at the beginning of the focus group session, then watched the custom-produced video. They rated format features of the video using 3-point response scales (e.g., “Was the talking speed good?” – With options: Yes, No (too slow), No (too fast)).
Data analysis
Focus group data from all stages were analysed using two levels of analysis. The first level of analysis involved a descriptive analysis of responses to each question (counts and percentages). The available case analysis approach described by Piggott (2001) was used, i.e., there was no substitution/imputation for missing data. The second level involved qualitative content analysis of participants’ verbal comments which were transcribed from the session’s videorecording. During the content analysis, one member of the research team read the focus group transcripts multiple times and identified meaning units within the transcripts. Meaning units were labelled with a code and grouped into categories and subcategories (as per Graneheim & Lundman, Citation2004). To ensure rigour, the codes, subcategories and categories were reviewed by a second member of the research team. Any discrepancies were resolved by discussion between the two research team members.
Results
Due to the online nature of the focus groups to maximise international reach and minimise COVID-19 risks, some participants left focus groups early or arrived late resulting in missing data. Forty-three participants were included in the original data set; however, three participants were removed during data checking (n = 2 due to participation in more than one group scheduled for a single stage, n = 1 due to not responding to questions due to technological issues). Four participants participated in two stages. Visual inspection of the data did not indicate that responses from these four participants differed from the responses of participants who took part in one stage only. All other participants participated in one stage only. Quantitative results are presented in along with participant quotes relating to each question. lists only the most frequent and second most frequent response given in Stage 2. The results from the content analysis from all three stages are presented in Supplementary table 1. Stage 1 resulted in 11 questions which formed the topic guide for Stage 2 (these questions and their response options are presented in ). Four of the eleven questions were added by PWA during stage 1. Quantitative analysis of Stage 2 data resulted in clear preferences for accessible aphasia research videos for PWA that involved a normal talking speed, a photo of the researchers at the start, listed keywords, a mix of images, lack of background music, inclusion of a summary at the end and a list of resources related to the theme of the video, and availability in different languages. Participants did not have strong preferences about whether PWA alone should decide the topic of the video or whether the topic decision should be a joint decision of PWA and researchers; however, over two-thirds of participants voted that a PWA should be part of the video. Participants responded that the preferred length of the video depended on factors such as the content of the video; however, 5 – 10 minutes was the most acceptable duration.
In Stage 3, participants concurred with the summarised results from Stage 2 (See ). Participants had favourable perceptions towards the aphasia research video developed according to the preferences identified in Stage 2. Participants strongly preferred eight features of the aphasia research video (including the talking speed, use of key words, and concluding summary), but raised improvements for two features. Specifically, while participants preferred the photos of the researchers at the start, they requested more time to view the photos so they could see all the researchers. The second feature that participants commented about a change was with respect to the used images. Approximately half of the participants commented that they initially did not understand the box plot graph; however, this was well-explained by the researcher in the video which negated their initial confusion. The final preferences for aphasia research videos were collated by the research team and synthesised into a single graphical figure to aid dissemination (See ).
Figure 1. Preferences of people with aphasia about the features of aphasia research videos.
Discussion
The current study explored the format preferences of PWA for aphasia research videos. We identified 11 consumer-informed preferences for aphasia research videos encompassing speech rate, duration, use of images and keywords, inclusion of PWA in the video and topic selection, background music, and inclusion of summaries and resource links. These preferences add another puzzle piece to the growing body of research focused on developing recommendations for aphasia-accessible information (e.g., Brennan et al., Citation2005; Rose et al., Citation2003; Rose et al., Citation2011; Language-Light UX, http://languagelightux.org/). Specifically, the current research extends previous recommendations about aphasia-accessible written information (Brennan et al., Citation2005; Rose et al., Citation2003; Rose et al., Citation2011) and websites (Language-Light UX, http://languagelightux.org/) to include preferences for video formats. This is highly relevant not only for the increasingly virtual world following the global COVID-19 pandemic, but also for helping bridge the evidence-knowledge gap in the aphasia community. The current list of preferences may be another step in reducing the information barriers experienced by PWA and their families, enabling greater participating in healthcare decisions by PWA. This research may stimulate further research into identifying preferences for other non-print information provision formats for PWA, such as podcasts.
Limitations and future directions
The study was impacted by several limitations. For feasibility reasons, we limited participants to English-speaking countries. Despite widespread online dissemination efforts via CATs and ARC social media, there was unequal representation across countries, with a preponderance of participants from the US. Future research should replicate the results in PWA who speak languages other than English. It must also be acknowledged that participants were a self-selecting group, representing only a fraction of the post-stroke aphasia population age-wise (majority were ≤ 65 years old), and less likely to have very severe aphasia (“No usable speech or auditory comprehension” according to the ASRS: 0 participants), thus limiting generalizability. It was not possible to provide an aphasia severity rating for all participants as some participants had insufficient verbal communication during the focus group. Furthermore, it is possible that the pattern of preferences may change with larger samples of PWA. We cannot discount skewing of the results by the missing responses for some of the items, due to participants arriving late or leaving the online groups early. Finally, we acknowledge the use of the ASRS for grading aphasia severity did not follow the standard assessment procedure which involves a semi-standardized 10-minute interview. We are confident though, that we generally achieved our main goal of including PWA of various aphasia severities by rating their verbal communication abilities during the focus group session. Future research could include a more standardized evaluation of aphasia severity and subtype, and their impacts on aphasia research video preferences. Including a person with PWA as moderator instead of as a commentator (such as in our Stage 3 example video) in the research video may be an additional preference of PWA which should be examined in future research.
Conclusion
In academia and health research, there is increasing awareness that people with the lived experience of aphasia should have access to key research findings about their condition. This will enable consumers to decide upon their unmet research needs and inform their routine care treatment decisions. One way of achieving this is through dissemination of research findings in a format that is easily accessible to patients. Our research project developed a set of 11 consumer-informed preferences for aphasia-accessible research videos that can be used by aphasia researchers to guide the development of aphasia research videos for PWA (and their families). Accessible aphasia research videos may additionally assist clinical stakeholder groups, such as aphasia therapists, to bridge the current evidence-practice gap in aphasia management. Further research is required with larger and better described samples of PWA, and should also include perspectives of non-English speaking PWA.
Data availability
The focus group guide is available from (https://osf.io/fmg7q/, Centre for Open Science). The data collected from participants is not available for sharing publicly due to ethical restrictions.
Acknowledgements
We would like to thank the PWA who gave their valuable time to share their perspectives. We are grateful for the support of Prof Cathy Price (University College London, Great Britain) and Dr Helen Kelly (University College Cork, Ireland) in recruiting participants for the online focus groups in Stage 2. Special thanks go to the members of Aphasia Recovery Connection. We acknowledge the support of the Collaboration of Aphasia Trialists which is funded by COST and the Tavistock Trust for Aphasia in fostering international aphasia research collaboration. Sarah J. Wallace is supported by a National Health and Medical Research Council (NHMRC) Investigator Grant (1175821).
Disclosure statement
The authors report there are no competing interests to declare.
References
- Aarnio, K., Rodriguez-Pardo, J., Siegerink, B., Hardt, J., Broman, J., Tulkki, L., … & Putaala, J. (2018). Return to work after ischemic stroke in young adults: A registry-based follow-up study. Neurology, 91(20), e1909–e1917. doi:10.1212/WNL.0000000000006510
- Brennan, A., Worrall, L., & McKenna, K. (2005). The relationship between specific features of aphasia-friendly written material and comprehension of written material for People with aphasia: An exploratory study. Aphasiology, 19(8), 693–711. doi:10.1212/WNL.0000000000006510
- Goodglass, H., Kaplan, E., & Baressi, B. (2000). The Assessment of Aphasia and Related Disorders (3rd ed.). Lippincott, Williams, & Wilkins.
- Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105–112. doi:10.1016/j.nedt.2003.10.001
- Pearl, G., & Cruice, M. (2017). Facilitating the involvement of people with aphasia in stroke research by developing communicatively accessible research resources. Topics in Language Disorders, 37(1), 67–84. doi: 10.1097/TLD.0000000000000112
- Pedersen, P. M., Stig Jørgensen, H., Nakayama, H., Raaschou, H. O., & Olsen, T. S. (1995). Aphasia in acute stroke: Incidence, determinants, and recovery. Annals of Neurology, 38(4), 659–666. doi: 10.1002/ana.410380416
- Pigott, T. D. (2001). A review of methods for missing data. Educational Research and Evaluation, 7(4), 353–383. doi: 10.1076/edre.7.4.353.8937
- Rose, T. A., Worrall, L. E., Hickson, L. M., & Hoffmann, T. C. (2011). Aphasia friendly written health information: Content and design characteristics. International Journal of Speech-Language Pathology, 13(4), 335–347. doi: 10.3109/17549507.2011.560396
- Rose, T., Worrall, L., & McKenna, K. (2003). The effectiveness of aphasia‐friendly principles for printed health education materials for people with aphasia following stroke. Aphasiology, 17(10), 947–963. doi: 10.1080/02687030344000319
- Simmons-Mackie, N., Raymer, A., Armstrong, E., Holland, A., & Cherney, L. R. (2010). Communication partner training in aphasia: A systematic review. Archives of Physical Medicine and Rehabilitation, 91(12), 1814–1837. doi:10.1016/j.apmr.2010.08.026
- Simmons-Mackie, N., Raymer, A., & Cherney, L. R. (2016). Communication partner training in aphasia: An updated systematic review. Archives of Physical Medicine and Rehabilitation, 97(12), 2202–2221. doi: 10.1016/j.apmr.2016.03.023
- Tomkins, B., Siyambalapitiya, S., & Worrall, L. (2013). What do People with aphasia think about their health care? Factors influencing satisfaction and dissatisfaction. Aphasiology, 27(8), 972–991. doi: 10.1080/02687038.2013.811211
- Vasileiou, K., Barnett, J., Thorpe, S., & Young, T. (2018). Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BioMed Central Medical Research Methodology, 18(1), 1–18. doi: 10.1186/s12874-018-0594-7
- Webster, J., Morris, J., Connor, C., Horner, R., McCormac, C., & Potts, A. (2013). Text level reading comprehension in aphasia: What do we know about therapy and what do we need to know?. Aphasiology, 27(11), 1362–1380. doi: 10.1080/02687038.2013.825760