
ABSTRACT
Recent studies report prevalence, phenotype, and persistence findings for a paediatric motor speech disorder in addition to childhood dysarthria and childhood apraxia of speech termed Speech Motor Delay (SMD). The aim of the present study was to determine if there is a frequent acoustic sign of SMD, with implications for theory, assessment, and treatment.
We examined the frequency of 19 acoustic signs of SMD in audio recordings of continuous speech and word-imitation tasks in three groups of speakers with SMD: 50 children (mean age 5.1 years) with idiopathic Speech Delay (SD) from 6 USA cities; 87 children, adolescents, and adults with eight types of complex neurodevelopmental disorders; and 9 children (mean age 8.8 years) with persistent idiopathic SD from a population-based study of children in the South West of England. The 19 acoustic signs of imprecise or unstable speech, prosody, and voice were standardized on typical speakers of the appropriate dialect. The criterion for a frequent acoustic sign was that it occurred in at least 50% of participants with SMD in each of the three groups.
Findings indicated that lengthened mid-vowels and diphthongs was the one sign that met criteria, occurring in 64.4% of the 146 participants with SMD, including 71% of the 87 participants with complex neurodevelopmental disorders. Findings are interpreted to support the potential of this acoustic sign, and possibly several others associated with temporal dimensions of speech sound development, to inform explication of the neuromotor substrates of SMD.
A clinical entity termed Speech Motor Delay (SMD) has recently been proposed as a classification for speakers with a delay in the development of speech motor control (Shriberg, Kwiatkowski, & Mabie, Citation2019). Initial studies of SMD, using the provisional classification Motor Speech Disorder-Not Otherwise Specified (Shriberg, Citation2017), described a measure to identify children with Speech Delay (SD) and concurrent SMD termed the Precision-Stability Index (PSI: Shriberg et al., Citation2010a). In a study using the PSI to estimate the prevalence of SMD in 415 children with idiopathic SD in six USA cities (mean age: 5.1 years; standard deviation: 1.7 years), the group-averaged prevalence of SMD concurrent with SD was 12% (Shriberg et al., Citation2019). In a study using the PSI to estimate the prevalence of SMD in 346 children, adolescents, and adults with eight types of complex neurodevelopmental disorders (CND), the group-averaged prevalence of SMD in the eight CND was 25.1% (Shriberg, Strand, Jakielski, & Mabie, Citation2019). In a retrospective longitudinal study of 14 participants in treatment for idiopathic SD, 11 (78.6%) participants normalized SMD before 9 years of age, and SMD persisted until at least late adolescence in the remaining 3 (21.4%) participants (Shriberg, Campbell, Mabie, & McGlothlin, Citation2019). The latter study provided the longitudinal support for replacing the provisional classification term Motor Speech Disorder-Not Otherwise Specified with the present term, SMD. Specifically, most children in the retrospective longitudinal study resolved SMD without direct treatment of the motor speech component, supporting the construct of a developmental delay in speech motor development. A study by Namasivayam, Granata, Huynh, and Van Lieshout (Citation2018) is the first to report treatment effects using principles of motor learning with a group of children classified descriptively as having SMD.
The SMD study by Shriberg, Campbell, et al. (Citation2019) cited above also included an analyses of the 10 most frequent perceptual or acoustic signs of SMD. The 10 signs that met the frequency criterion (over 50% of participants positive on the sign) included age-inappropriate precision and stability behaviours in speech, prosody and voice domains, with 7 of the 10 most frequent signs involving speech production. Of present interest is that 4 of the 10 signs used acoustic procedures (Shriberg, Campbell, et al., Citation2019, Table 4). Automated acoustic assessment methods in speech pathology have several attractive measurement features relative to perceptual methods, including sensitivity to continuous variables, reliability, and efficiency (cf. McAllister & Ballard, Citation2018).
Statement of purpose
The purpose of the present initial study was to determine if there is one or more prevalent acoustic signs of SMD that could be informative in studies to explicate core motor speech processes underlying SMD. A prevalent speech motor sign of SMD was defined as one on which at least 50% of speakers with SMD have a z-score greater than 1.25 standard units from the mean of typical speakers of the same age and sex. We address the question using audio-recorded speech samples from three studies, each with the potential to provide alternative sources of internal and external validity support for one or more 70 prevalent signs of SMD.
Method
Participants
includes descriptive information for three groups of participants whose audio-recorded speech samples were analysed for the present study, and three groups of typically-developing speakers used to standardize participant scores on the measures to be described. All participants were assented and/or consented using procedures approved by Internal Review Boards at the University of Wisconsin-Madison, the Mayo Clinic-Rochester, Minnesota, the University of Bristol (ALSPAC Ethics and Law Committee and the Local Research Ethics Committees), and collaborative research sites in five other USA cities (Cincinnati, Cleveland, Dallas, Denver, and Pittsburgh).
Table 1. Description of target participants in three groups of speakers with Speech Motor Delay (SMD) and control participants in two of the three groups. The lower three rows include information on participants in three databases of speakers with typically-developing speech used to standardize measures.
USA group
Participants in the USA group were identified from a database of 415 children recruited for research in SD in six USA cities (Shriberg, Kwiatkowski, & Mabie, Citation2019). All participants met criteria for idiopathic SD using Speech Disorders Classification System (SDCS) software (Shriberg, Citation1993, Appendix). As shown in , 50 of these participants also met criteria (to be described) for concurrent SMD and 341 participants from this database used as a control group met criteria for No Motor Speech Disorder. Participants’ average ages in the USA participant and control groups, respectively, were 5.1 years (1.7) and 4.8 years (1.7). All participants had General (i.e., mainstream) American dialects. The approximately two-hour assessment protocol for the six samples included a five to eight minute audio-recorded conversational speech task. For participants in three of the six USA cities, the protocol included two audio-recorded vowel/diphthong word-imitation tasks presented by computer. The first task included pictures of words containing the four corner vowels (beet, bat, boot, pot) in four randomized lists, with each picture accompanied by an audio recording of each word spoken by an experienced female speech pathologist. The second task included 11 CVC words containing six mid-vowels (bit, pet, putt, Bert, put, bought) and the five diphthongs (bite, bait, boat, boy, pout) presented in four randomized lists accompanied by an audio recording of each word spoken by the same speech pathologist. Stimuli were presented free field at a comfortable loudness level. Participants were asked to repeat each word exactly the way the woman said it.
Complex Neurodevelopmental Disorders group
A total of 87 participants with SMD were identified from a database of 346 children, adolescents, and adults with one of eight types of CND recruited for speech-genetics and behavioural speech research (Shriberg, Strand, et al., Citation2019). As shown in , 181 of the 346 participants met criteria for No Motor Speech Disorder. Participants’ average chronological age was 15.4 years (11.2) in the CND SMD group and 11.7 years (10.6) in the CND No Motor Speech Disorder group. All participants had General American dialects. CND participants completed assessment protocols similar to the protocol used for participants in the USA group, which included a conversational speech sample for all participants. Because the vowel tasks were developed relatively recently, only some participants in three of the smaller size CND groups had been administered the two word-imitation tasks.
Avon Longitudinal Study of Parents and Children group
The Avon Longitudinal Study of Parents and Children (ALSPAC) dataset (Wren, McLeod, White, Miller, & Roulstone, Citation2013; Wren, Miller, Peters, Emond, & Roulstone, Citation2016; Wren, Roulstone, & Miller, Citation2012) provided an opportunity to examine acoustic signs of SMD in children with idiopathic SD who differed in several ways from the participants in the USA and CND groups. ALSPAC is a large-scale longitudinal prospective population study which has followed the health and development of a cohort of children from pre-birth into adulthood. Pregnant women resident in the geographical area previously known as Avon in the South West of England, UK, with expected dates of delivery 1st April 1991 to 31st December 1992 were invited to take part in the study. The initial number of pregnancies enrolled was 14,541. Of these initial pregnancies, there was a total of 14,676 foetuses, resulting in 14,062 live births and 13,988 children who were alive at 1 year of age (Boyd et al., Citation2013; Fraser et al., Citation2013). The study website contains details of all the data that is available through a fully searchable data dictionary and variable search tool and references the following webpage: http://www.bristol.ac.uk/alspac/researchers/our-data/
At age 8, all children in the cohort were invited to attend a clinic to undertake a battery of assessments measuring health and development across a number of domains, including speech and language. Audio-recorded speech samples were available from 156 children who met ALSPAC investigators criteria for Persistent Speech Disorder from the total of 7390 children who attended the 8-year assessment clinic. Thus, participants in this cohort differed from the USA cohorts in that they were sampled from a population-based study, spoke a different dialect of English than General American, had been classified as having idiopathic Persistent Speech Disorder using a research protocol administered and transcribed by a different group of speech-language researchers, and were approximately 4 years older at assessment than participants in the USA group.
The assessment data for the ALSPAC study included audio-recorded continuous speech from three picture description activities (Wren et al., Citation2013). For the first picture, the child was asked to describe a community scene as if to someone who was not present and therefore could not see the scene. For the second picture the child was shown a map and asked to describe the shortest directions from one location to another. For the third task which also used pictures, the child was asked to explain the sequence of steps in putting batteries into a flashlight (torch). For the present study, as described in following sections, a file that included the three continuous speech samples was used to classify participants’ status on the acoustic items of the measure used to identify speakers with SMD.
Reference databases
The database used to standardize measures for USA participants included 150 3- to 18-year-old typically-developing children with mainstream General American dialects (Potter et al., Citation2012). The reference data for the CND group included the 150 children and adolescents, plus data from 50 20- to 80-year-old adults with General American dialects, including approximately 10 participants per decade (Scheer-Cohen et al., Citation2013). The assessment protocols for both standardization samples included a conversational sample and the two word-imitation tasks. The database used to standardize the three continuous speech samples from the ALSPAC group included audio-recordings of the three picture description activities by 25 8-year-old typically-developing speakers from the same Avon, UK region (Wren et al., Citation2013).
Data reduction
Four research specialists completed narrow phonetic transcription, prosody-voice coding, and acoustic analyses of the audio-recorded conversational speech samples and the two word-imitation tasks in the USA and CND groups using procedures developed for research in speech sound disorders (Shriberg et al., Citation2010b). For the three types of data reduction, randomly selected, 20% intrajudge and interjudge point-to-point percentages of agreements for 26 perceptual and acoustic variables ranged from 74.9% to 97.3% for the USA samples (Shriberg, Kwiatkowski, & Mabie, Citation2019) and 69.7% to 97.5% for the CND samples (Shriberg, Strand, et al., Citation2019).
Because pilot studies indicated that dialectal differences precluded reliable narrow phonetic transcription and prosody-voice coding of the ALSPAC picture task data by the American research specialists, only data from the acoustic analyses of the ALSPAC files were processed for the present study (to be described). An interjudge reliability estimate reported previously was obtained for the four British transcribers who transcribed all eight-year assessment data by having a transcriber who participated in previous years’ assessments transcribe 48 randomly selected files from the eight-year assessment (Wren et al., Citation2013). Chronbach’s alpha coefficients were 0.78 for the Percentage of Consonants Correct-Adjusted and 0.87 for the Percentage of Consonants Correct Late-8.
Speech and motor speech classification
USA and CND groups. Participants in the USA and CND groups met perceptual-based
criteria for Normal Speech Acquisition, SD, or Persistent SD (if older than 9 years of age), using a prior version of the Speech Disorders Classification System (Shriberg, Austin, Lewis, McSweeny, & Wilson, Citation1997, Appendix A). Participants in both groups also met perceptual and acoustic criteria for one of five concurrent, mutually exclusive motor speech classifications described in a previous paper in this issue (Shriberg, Kwiatkowski, & Mabie, Citation2019): No Motor Speech Disorder, Speech Motor Delay, Childhood Dysarthria (CD), Childhood Apraxia of Speech (CAS), or concurrent Childhood Dysarthria and Childhood Apraxia of Speech (CD & CAS). The Speech Disorders Classification System software for motor speech disorders uses findings from three standardized perceptual-acoustic measures – the Precision-Stability Index, the Dysarthria Index, and the Pause Marker (Shriberg et al., Citation2017a) – to classify children into one of the five motor speech classifications. A Supplement for this research series provides detailed information on classification methods and measures [Supplementary Data].
is a manual copy of the PSI assessment form, the measure used to identify speakers with early or persistent SMD. The PSI includes 13 perceptual and 19 acoustic signs of imprecise and/or unstable speech, prosody and voice in continuous speech. As shown in , the 32 signs are subsumed within ten linguistic domains. Performance on a sign greater than 1.25 standard deviations in the negative direction from typical speakers of same age and sex is coded as positive for the sign. Speakers with more than 30% positive signs are classified as SMD. Speakers who are positive for CD and/or CAS may also be positive for SMD. For such outcomes, the classification software assigns the motor speech classification to the putatively more severe motor speech classification (i.e., CD and/or CAS). Thus, the 50 participants in the present USA group and 87 in the present CND group met motor speech classification criteria for only SMD.
Figure 1. The Precision-Stability Index (PSI).
ALSPAC group
Due to the reliability constraints on the narrow phonetic transcription and prosody-voice coding of the British speech samples by the USA transcribers, the transcriptions could not be classified using the USA transcriptions. Rather, the speech classification of the 156 ALSPAC speakers used in the present study were the speech classifications reported in Wren et al. (Citation2013). Specifically, classification of participants as Persistent Speech Disorder was based on the speech assessment measures and criteria described in Wren et al. (Citation2013) and Wren et al. (Citation2016), and classification of the delay as idiopathic was based on the extensive developmental data obtained for each participant in the same publications.
Acoustic analyses of the 156 ALSPAC participants with Persistent Speech Disorder were used to determine which participants met SDCS acoustic criteria for concurrent SMD. First, each participant’s responses to the three picture tasks were combined into one digital file. Second, two of the four USA research specialists completed acoustic analyses of the 19 acoustic items of the PSI () using the same procedures as used for acoustic analyses of participants in the USA and CND groups. ALSPAC participants who were positive on more than 30% of the acoustic signs (i.e., who had a PSI score lower than 70% on the 19 signs) using the Bristol reference data () were classified as positive for SMD. It is important to note that due to this accommodation (i.e., using only the 19 acoustic signs in the PSI) the number of ALSPAC participants with SMD (n = 9) is not an estimate of the prevalence of SMD concurrent with idiopathic Persistent Speech Disorder in this population-based sample.
Results
A frequent sign of speech motor delay
includes findings for the question posed: is there one or more frequent acoustic signs of SMD that could be informative in studies to explicate the core motor speech processes underlying SMD? The numbers below each bar in correspond to the numbered signs in , and the rounded percentage above each bar is the percentage of participants in each group positive on the sign. For the present purposes, the 19 acoustic signs are aggregated into eight speech, prosody, and voice domains, with each domain including 1–3 acoustic signs. The left-to-right sequence of the eight domains and the signs within each domain are ordered approximately by the highest percentage of total participants in the three groups or in just the USA and CND groups positive on the domain.
Figure 2. Acoustic signs of Speech Motor Delay in three study groups. The groups are USA = United States of America, CND = Complex Neurodevelopmental Disorders, and ALSPAC = Avon Longitudinal Study of Parents and Children.
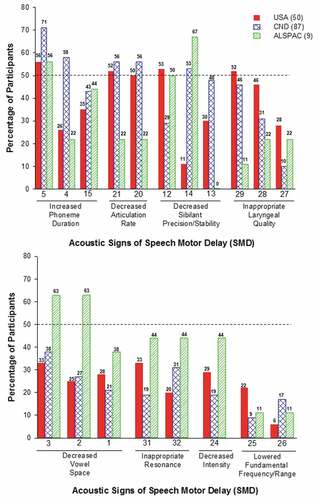
As shown in , the most frequent of the 19 acoustic signs of SMD in the continuous speech of participants in the three groups was PSI Sign No. 5: Increased Duration of Mid-Vowels (Monophthongs) and Diphthongs (cf., ). This acoustic sign was the only one of the 19 on which over 50% of participants with SMD in the three groups were positive. As shown, 71% of participants with SMD in the CND group had longer durations averaged over the 11 phonemes in the continuous speech samples than typical speakers of their chronological age and sex. Inspection of the CND samples indicated that this was the case for 12 of the 12 (100%) participants with Down syndrome, 7 of the 7 (100%) participants with Galactosemia, 5 of the 6 (83.3%) participants with Autism Spectrum Disorder, 4 of the 5 (80%) participants with 22q11.2 deletion syndrome, 22 of the 30 (73.3%) participants with 16p11.2 deletion, and 5 of the 8 (62.5%) participants with fragile X syndrome. Other signs of SMD in (to be discussed) met the >50% criteria for one or two of the three groups, including other vowel signs and signs associated with reduced rate, but PSI Sign No. 5 was the only sign meeting the three-group criterion for a frequent acoustic sign of SMD.
Vowel/diphthong durations in conversational speech and in a word-imitation task
includes descriptive and inferential statistical findings for PSI Sign No. 5:Increased Duration of Mid-Vowels and Diphthongs for participants in the two groups (USA and CND) in each of the speech tasks (continuous speech and word-imitations). Unlike the word-imitation task in the Madison Speech Assessment Protocol that assesses corner vowels (Vowel Task 1), the word-imitation task that assesses mid-vowels and diphthongs had been administered to only three of the CND groups yielding only 11 participants with SMD in each group with available data on this task.
Table 2. PSI Sign No. 5 findings for participants in the USA and Complex Neurodevelopmental Disorder (CND) groups with idiopathic Speech Delay and Speech Motor Delay (SMD) compared to control participants with idiopathic Speech Delay and No Motor Speech Disorder (No MSD) in two speech tasks.
As indicated in , three of the four comparisons of PSI Sign No. 5 findings yielded significant differences in the average duration of vowels/diphthongs, as determined by confidence intervals that did not cross 0.00. The primary finding in is that when sampled in continuous speech, the average durations of the 11 mid-vowels/diphthongs were significantly longer for the participants with SMD than for participants with No Motor Speech Disorder in both the USA (effect size = 0.63) and CND (effect size = 0.43) groups. A secondary finding was that as sampled in the word-imitation task, participants in the CND group with SMD had significantly longer average durations of the 11 mid-vowels/diphthongs than participants in the CND group with No Motor Speech Disorder (effect size = 1.16).
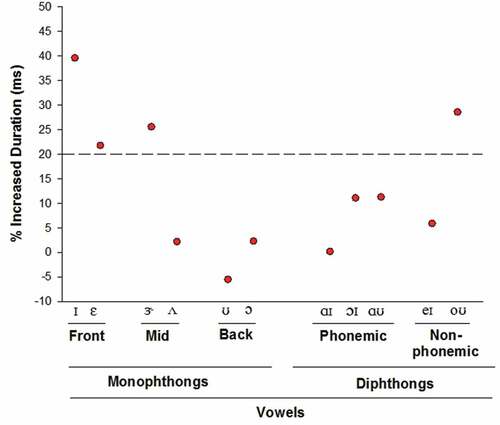
provides a graphic summary of the averaged percentage of increased durations of the six vowels and five diphthongs from the continuous speech samples of participants with SD and SMD, compared to durations of these phonemes from the continuous samples of participants with SD and No Motor Speech Disorder. The plotted values are the averaged percentage of increased duration for each phoneme (i.e., Mean Duration for participants with No Motor Speech Disorder – Mean Duration for participants with SMD/Mean Duration for participants with No Motor Speech Disorder x 100). The dashed line at 20% is an arbitrary visual aid that demarcates the four phonemes with the longest durations from the data points for the remaining seven phonemes. As shown, participants with SMD averaged 39.6% and 21.8% longer durations on the two lax front vowels /ɪ/ and /ɛ/, respectively, 25.6% longer durations on the stressed mid vowel /ɝ/, and 28.6% longer durations on the non-phonemic diphthong /oʊ/.
Figure 3. Average duration (ms) of the 11 phonemes in PSI 5: Increased Duration of Mid-Vowels and Diphthongs in the continuous speech tasks from participants with idiopathic Speech Delay (SD) and Speech Motor Delay compared to durations of these phonemes from the continuous speech of participants with SD and No Motor Speech Disorder (see text).
Discussion and conclusion
Findings
The primary finding for the question posed is that compared to participants with No Motor Speech Disorder, increased duration of mid-vowels and diphthongs was a frequent sign of SMD in children with idiopathic SD. The finding was supported in participants with some types of CND. Findings suggest that additional research focused on the durations of the front vowels, /ɪ/ and /ɛ/ may be particularly informative for theory. Unlike the maximal spatial positions of the jaw, tongue, and lips required for the four tense corner vowels (PSI Sign No. 4) and the complex tongue and lips configurations required of the rhotic /ɝ/ and spatiotemporal requisites of the diphthong /oʊ/(), the lax monophthongs /ɪ/ and /ɛ/ are made with neutral tongue, jaw, and lip positions (Shriberg, Kent, McAllister, & Preston, Citation2019). Because the spatial requisites of /ɪ/ and /ɛ/ are not difficult in continuous speech, research on their temporal control in motor speech development may provide insights into core speech motor control processes in SMD. One possibility is that the increased durations of vowels in speakers with SMD is due to difficulties in planning the phonological phrase. As reported in a study of childhood apraxia of speech by Nijland et al. (Citation2003), whereas children with typical speech learn to shorten the duration of an unstressed syllable in a prosodically weak position, children with childhood apraxia of speech (and perhaps SMD) have substantial difficulty acquiring the appropriate durations of unstressed syllables (e.g., Arciuli & Ballard, Citation2017; Kehoe, Stoel-Gammon, & Buder, Citation1995). Comparative research is needed to determine if the increased durations of /ɪ/ and /ɛ/ in children with SMD are similar to the increased durations of these phonemes in the speech of children with CAS, perhaps reflecting developmental constraints in feedforward processes in speech motor development (Terband, Maassen, Guenther, & Brumberg, Citation2014). As described in Shriberg, Kwiatkowski, and Mabie (Citation2019) and Shriberg, Campbell, et al. (Citation2019), a speculation is that false positive diagnoses of CAS could be due, in part, to such overlaps in the phenotypes of childhood apraxia of speech and SMD.
Although they did not meet the arbitrary criterion for a frequent sign of SMD (i.e., >50% occurrence in participants in all three research groups), other findings in support the potential deficits in temporal processes implied in the significant findings for PSI Sign No. 5. A total of 58% of participants with CND were positive on PSI Sign No. 4: Increased Duration of Corner Vowels and 50%-56% of participants in the USA and CND studies were positive on PSI Sign No. 21: Increased Syllable Length and/or PSI Sign No. 20: Reduced Syllables per second (without pauses). Decreased articulation rate (i.e., speaking time – pause time) can be a function of increased vowel and consonant lengths. The remaining PSI signs on which over 50% of participants in at least one group were positive do not suggest immediate interpretation. Notably, for the widely studied domain of vowel space in the motor speech literature, neither of the two larger of the three groups had over 50% of participants positive on any of the three PSI signs of decreased vowel space.
Research and clinical directions
Studies to replicate and extend the present initial findings with participants selected to control for relevant threats to internal and external validity would appear to be warranted. Specifically, replication studies of PSI Sign No. 5 should be undertaken in studies with sufficient statistical power to control for possible associations of SMD with relevant demographic, sensory, cognitive, speech, language, and treatment history variables. If the present and/or additional acoustic signs are cross-validated, clinical directions for assessment and treatment of SMD include the possible development of automated assessment applications.
Conclusion
As proposed in the first three articles in the present research series, the precision and stability deficits in SMD are posited to result from processing constraints at the execution stage of speech production (Shriberg, Kwiatkowski, & Mabie, Citation2019, ). The present findings, however, are more consistent with the conclusion in Shriberg, Campbell, et al. (Citation2019) that there likely are common neurodevelopmental pathways underlying the four SDCS classifications of motor speech disorder phenotypes – SMD, CD, CAS, and CD & CAS. Prevalence estimates in Shriberg, Strand, et al. (Citation2019) indicated that CD & CAS was at least as prevalent as CAS in some of the study groups, suggesting common genomic and neurodevelopmental pathways. In the present study, the high percentage of children with SMD with increased durations of vowels that are not difficult to articulate could reflect transcoding (planning/programming) deficits associated with stress that are similar to the transcoding deficits proposed in CAS (Shriberg et al., Citation2017b). The likelihood of identifying causal genes and copy number variants for SMD that confer risk for pleiotropic effects within and among speech, language, and motor domains is consistent with contemporary trends in genomic research in verbal trait disorders (e.g., Lewis, Iyengar, & Stein, Citation2018; Miscimarra et al., Citation2007; Peter, Matsushita, & Raskind, Citation2012; Smith, Pennington, Boada, & Shriberg, Citation2005; Stein et al., Citation2006, Citation2004; Truong et al., Citation2016).
Supplemental Material
Download PDF (801 KB)Acknowledgments
This research was supported by National Institute on Deafness and Other Communication Disorders Grant DC000496 and in part by a core grant to the Waisman Center from the National Institute of Child Health and Human Development (U54 HD090256). Core support for ALSPAC is provided by the UK Medical Research Council and Wellcome Trust (Grant ref: 102215/2/13/2) and the University of Bristol. Funding for the preliminary analysis of the speech data used in ALSPAC was provided by the UK Medical Research Council (Grant ref: G0501804 ID 76829). A comprehensive list of grants funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf). This publication is the work of the authors, and Shriberg and Wren will serve as guarantors for the contents of this paper.
We thank each of the following colleagues for her or his contribution to this research: Marios Fourakis, Sheryl Hall, Heather Karlsson, Heather Mabie, Jane McSweeny, Christie Tilkens, and David Wilson. We are extremely grateful to all the families who took part in the ALSPAC study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. We also thank the speech team who carried out the UK transcription and Sue Roulstone and Sue Loader who were instrumental in ensuring the data were collected.
Supplemental data
Supplemental data for this article can be accessed here.
Disclosure Statement
The authors report no declarations of interest.
Additional information
Funding
References
- Arciuli, J., & Ballard, K. J. (2017). Still not adult-like: Lexical stress contrastivity in word productions of eight- to eleven-year-olds. Journal of Child Language, 44, 1274–1288. doi:10.1017/S0305000916000489
- Boyd, A., Golding, J., Macleod, J., Lawlor, D. A., Fraser, A., Henderson, J., … Davey Smith, G. (2013). Cohort profile: the ‘children of the 90s’; the index offspring of the Avon Longitudinal Study of Parents and Children (ALSPAC). International Journal of Epidemiology, 42, 111–127. doi:10.1093/ije/dys064
- Fraser, A., Macdonald-Wallis, C., Tilling, K., Boyd, A., Golding, J., Davey Smith, G., … Lawlor, D. A. (2013). Cohort Profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. International Journal of Epidemiology, 42, 97–110. doi:10.1093/ije/dys066
- Hedges, L. V., & Olkin, I. (1985). Statistical methods for metaanalysis. Boston, MA: Academic Press.
- Kehoe, M., Stoel-Gammon, C., & Buder, E. H. (1995). Acoustic correlates of stress in young children’s speech. Journal of Speech and Hearing Research, 38, 338–350.
- Lewis, B. A., Iyengar, S. K., & Stein, C. M. (2018). Genetics of speech sound disorders and comorbid disorders: A new era of discovery. Paper presented at the Annual Convention of the American Speech-Language-Hearing Association, Boston, MA.
- McAllister, T., & Ballard, K. J. (2018). Bringing advanced speech processing technology to the clinical management of speech disorders. International Journal of Speech-Language Pathology, 20, 581–679. (Eds.). doi:10.1080/17549507.2018.1510034
- Miscimarra, L., Stein, C., Millard, C., Kluge, A., Cartier, K., Freebairn, L., … Iyengar, S. K. (2007). Further evidence of pleiotropy influencing speech and language: Analysis of the DYX8 region. Human Heredity, 63, 47–58. doi:10.1159/000098727
- Namasivayam, A. K., Granata, F., Huynh, A., & Van Lieshout, P. H. H. M. (2018, November). Randomized control trial of PROMPT intervention for children with severe speech sound disorders. Paper presented at the Annual Convention of the American Speech-Language-Hearing Association, Boston, MA.
- Nijland, L., Maassen, B., van der Meulen, S., Gabreëls, F., Kraaimaat, F. W., & Schreuder, R. (2003). Planning of syllables in children with developmental apraxia of speech. Clinical Linguistics & Phonetics, 17, 1–24. doi:10.1080/0269920021000050662
- Peter, B., Matsushita, M., & Raskind, W. H. (2012). Motor sequencing deficit as an endophenotype of speech sound disorder: A genome-wide linkage analysis in a multigenerational family. Psychiatric Genetics, 22, 226–234. doi:10.1097/YPG.0b013e328353ae92
- Potter, N. L., Hall, S., Karlsson, H. B., Fourakis, M., Lohmeier, H. L., McSweeny, J. L., … Shriberg, L. D. (2012). Reference Data for the Madison Speech Assessment Protocol (MSAP): A Database of 150 Participants 3-to-18 Years of Age with Typical Speech. ( Technical Report No. 18). Phonology Project, Madison, WI: Waisman Center, University of Wisconsin–Madison. Retrieved from Phonology Project website: http://www.waisman.wisc.edu/phonology/
- Scheer-Cohen, A. R., Holt, A. S., Karlsson, H. B., Mabie, H. L., McSweeny, J. L., Tilkens, C. M., & Shriberg, L. D. (2013). Reference Data for the Madison Speech Assessment Protocol (MSAP): A Database of Fifty 20-to-80 year old Participants with Typical Speech. (Technical Report No. 20). Phonology Project, Madison, WI: Waisman Center, University of Wisconsin–Madison. Retrieved from Phonology Project website: http://www.waisman.wisc.edu/phonology/
- Shriberg, L. D. (1993). Four new speech and prosody-voice measures for genetics research and other studies in developmental phonological disorders. Journal of Speech and Hearing Research, 36, 105–140. doi:10.1044/jshr.3601.105
- Shriberg, L. D. (2017, July). Motor speech disorder-not otherwise specified: Prevalence and phenotype. Paper presented at the 7th International Conference on Speech Motor Control, Groningen, the Netherlands.
- Shriberg, L. D., Austin, D., Lewis, B. A., McSweeny, J. L., & Wilson, D. L. (1997). The Speech Disorders Classification System (SDCS): Extensions and lifespan reference data. Journal of Speech, Language, and Hearing Research, 40, 723–740. doi:10.1044/jslhr.4004.723
- Shriberg, L. D., Campbell, T. F., Mabie, H. L., & McGlothlin, J. H. (2019). Initial studies of the phenotype and persistence of Speech Motor Delay (SMD). Manuscript submitted for publication.
- Shriberg, L. D., Fourakis, M., Hall, S., Karlsson, H. B., Lohmeier, H. L., McSweeny, J. L., … Wilson, D. L. (2010a). Extensions to the Speech Disorders Classification System (SDCS). Clinical Linguistics & Phonetics, 24, 795–824. doi:10.3109/02699206.2010.503006
- Shriberg, L. D., Fourakis, M., Hall, S., Karlsson, H. B., Lohmeier, H. L., McSweeny, J. L., … Wilson, D. L. (2010b). Perceptual and acoustic reliability estimates for the Speech Disorders Classification System (SDCS). Clinical Linguistics & Phonetics, 24, 825–846. doi:10.3109/02699206.2010.503007
- Shriberg, L. D., Kent, R. D., McAllister, T., & Preston, J. L. (2019). Clinical phonetics (5th ed.). Boston, MA: Pearson Education.
- Shriberg, L. D., Kwiatkowski, J., & Mabie, H. L. (2019). Estimates of the prevalence of motor speech disorders in children with idiopathic speech delay. Manuscript submitted for publication.
- Shriberg, L. D., Strand, E. A., Fourakis, M., Jakielski, K. J., Hall, S. D., Karlsson, H. B., … Wilson, D. L. (2017a). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: I. Development and description of the Pause Marker. Journal of Speech, Language, and Hearing Research, 60, S1096–S1117.
- Shriberg, L. D., Strand, E. A., Fourakis, M., Jakielski, K. J., Hall, S. D., Karlsson, H. B., … Wilson, D. L. (2017b). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: III. Theoretical coherence of the Pause Marker with speech processing deficits in Childhood Apraxia of Speech. Journal of Speech, Language, and Hearing Research, 60, S1135–S1152.
- Shriberg, L. D., Strand, E. A., Jakielski, K. J., & Mabie, H. L. (2019). Estimates of the prevalence of speech and motor speech disorders in persons with complex neurodevelopmental disorders. Manuscript submitted for publication.
- Smith, S. D., Pennington, B. F., Boada, R., & Shriberg, L. D. (2005). Linkage of speech sound disorder to reading disability loci. Journal of Child Psychology and Psychiatry, 46, 1057–1066. doi:10.1111/j.1469-7610.2005.01534.x
- Stein, C. M., Millard, C., Kluge, A., Miscimarra, L. E., Cartier, K. C., Freebairn, L. A., … Iyengar, S. (2006). Speech sound disorder influenced by a locus in 15q14 region. Behavior Genetics, 36, 858–868. doi:10.1007/s10519-006-9090-7
- Stein, C. M., Schick, J. H., Taylor, H. G., Shriberg, L. D., Millard, C., Kundtz-Kluge, A., … Iyengar, S. K. (2004). Pleiotropic effects of a chromosome 3 locus on speech-sound disorder and reading. American Journal of Human Genetics, 74, 283–297. doi:10.1086/381562
- Terband, H., Maassen, B., Guenther, F. H., & Brumberg, J. (2014). Auditory-motor interactions in pediatric speech disorders: Neurocomputational modeling of disordered development. Journal of Communication Disorders, 47, 17–33. doi:10.1016/j.jcomdis.2014.01.001
- Truong, D. T., Shriberg, L. D., Smith, S. D., Chapman, K. L., Scheer-Cohen, A. R., DeMille, M. M. C., … Gruen, J. R. (2016). Multipoint genome-wide linkage scan for nonword repetition in a multigenerational family further supports chromosome 13q as a locus for verbal trait disorders. Human Genetics, 135, 1329–1341. doi:10.1007/s00439-016-1717-z
- Wren, Y., McLeod, S., White, P., Miller, L. L., & Roulstone, S. (2013). Speech characteristics of 8-year-old children: Findings from a prospective population study. Journal of Communication Disorders, 46, 53–69. doi:10.1016/j.jcomdis.2012.08.008
- Wren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language, and Hearing Research, 59, 647–673. doi:10.1044/2015_JSLHR-S-14-0282
- Wren, Y., Roulstone, S., & Miller, L. L. (2012). Distinguishing groups of children with persistent speech disorder: Findings from a prospective population study. Logopedics Phoniatrics Vocology, 37(1), 1–10. doi:10.3109/14015439.2011.625973