
ABSTRACT
The goal of this research was to assess the support for motor speech disorders as explanatory constructs to guide research and treatment of reduced intelligibility in persons with Down syndrome (DS). Participants were the 45 adolescents with DS in the prior paper who were classified into five mutually-exclusive motor speech classifications using the Speech Disorders Classification System. An ordinal index classified participants’ percentage of intelligible words in conversation as High (≥ 85%), Moderate (80% – 84.9%), or Low (< 80%). Statistical analyses tested for significant differences in intelligibility status associated with demographic, intelligence, and language variables, and intelligibility status associated with motor speech classifications and speech, prosody, and voice variables.
For the 10 participants who met criteria for concurrent Childhood Dysarthria and Childhood Apraxia of Speech at assessment, 80% had reduced (Moderate or Low) intelligibility and 20% had High intelligibility (significant effect size: 0.644). Proportionally more of the 32 participants who met criteria for either dysarthria or apraxia had reduced intelligibility (significant effect size: 0.318). Low intelligibility was significantly associated with across-the-board reductions in phonemic and phonetic accuracy and with inappropriate prosody and voice.
Findings are interpreted as support for motor speech disorders in adolescents with DS as explanatory constructs for their reduced intelligibility. Pending cross-validation of findings in diverse samples of persons with DS, studies are needed to assess the efficacy of motor speech classification status to guide selection of treatment methods and intelligibility targets.
Abbreviations: CAS: Childhood Apraxia of Speech; CD: Childhood Dysarthria; DS: Down syndrome; II: Intelligibility Index; No MSD: No Motor Speech Disorder; OII: Ordinal Intelligibility Index; PSD: Persistent Speech Delay; SDCS: Speech Disorders Classification System; SMD: Speech Motor Delay
Down syndrome and intelligibility
Speech intelligibility challenges are a major concern for individuals with Down syndrome (DS). In a widely-cited survey, 95% of parents of children with DS were concerned about their child’s ability to be understood by listeners (Kumin, Citation1994). Since 2000, representative research reviews and clinical proposals to increase the intelligibility and comprehensibility of persons with DS include Barnes et al. (Citation2009); Camarata, Yoder, and Camarata (Citation2006); Coppens-Hofman, Maassen, van Schrojenstein Lantman-de Valk, and Snik (Citation2012); Coppens-Hofman, Terband, Snik, and Maassen (Citation2016); Kent and Vorperian (Citation2013); Kumin (Citation2006); McDaniel and Yoder (Citation2016); Roberts, Price, and Malkin (Citation2007); Rvachew and Folden (Citation2018); Wild, Vorperian, Kent, Bolt, and Austin (Citation2018); Yoder, Camarata, and Woynaroski (Citation2016); and Yoder, Woynaroski, and Camarata (Citation2016). Although a variety of factors have been proposed to explain the intelligibility challenges of individuals with DS, the interactive contributions of multiple factors need to be modeled in a coherent explanatory framework to guide treatment. The following brief review includes examples of cognitive-linguistic, craniofacial, sensorimotor, and hearing factors that place persons with DS at increased risk for the speech, prosody, and voice deficits associated with reduced intelligibility.
Risk factors for reduced intelligibility in people with Down syndrome
Cognitive-linguistic
The cognitive profiles common to the phenotype of DS are well-documented, with IQs typically in the moderately to severely impaired range (Carr, Citation2012; Connolly, Citation1978; Pennington, Moon, Edgin, Stedron, & Nadel, Citation2003). Unlike consistent IQ scores observed across time in typically-developing children, decreasing IQs, reflecting a slowing of cognitive growth, have been reported in some samples of individuals with DS (see Pennington et al., Citation2003, for review), with other studies reporting minimal change during adulthood (21–45 years; Carr, Citation2012). Kent and Vorperian (Citation2013) have reviewed how short-term memory deficits common in individuals with DS can affect speech and language performance. Notwithstanding considerable research on cognitive characteristics of persons with DS, associations between specific cognitive impairments and linguistic ability are not well understood (McDuffie, Thurman, Channell, & Abbeduto, Citation2017).
Craniofacial
Craniofacial differences have been reported in individuals with DS, many of which may influence speech production. Kent and Vorperian (Citation2013) concluded that, compared to control participants, participants with DS had ‘reduced volumes of the airway, mandible, adenoid and tonsil and a smaller mid-lower-face skeleton and hard palate’ (p.10) associated with mid-lower face hypoplasia. Reports of macroglossia are also common, but recent studies suggest the presence of relative macroglossia (i.e., typical tongue size) secondary to undersized oral cavities (Guimaraes, Donnelly, Shott, Amin, & Kalra, Citation2008; Kent & Vorperian, Citation2013; Uong et al., Citation2001). These differences result in variations in laryngeal and resonatory properties of speech and voice production that can lower intelligibility.
Sensorimotor
Diminished peripheral somatosensory performance has been reported in persons with DS (Brandt & Rosén, Citation1995), resulting in decreased accuracy in stimuli detection and slower response times (Valkenburg, Tibboel, & van Dijk, Citation2015). Anecdotal clinical reports suggest diminished sensory ability of the oral mechanism during mastication and swallowing, including decreased awareness of bolus size, delayed initiation of the swallow, and laryngeal penetration due to undetected residual residue. Although sensory input plays a primary role in how infants learn the motor skills for speech (Guenther, Citation1995; Guenther, Hampson, & Johnson, Citation1998), the role of sensory processing in speech development and performance is not well understood.
Hearing
The DIVA model (Directions into Velocities of Articulators) posits that hearing plays a primary role in accurate speech production (e.g., Coppens-Hofman et al., Citation2012; Lane et al., Citation2005; Perkell et al., Citation2000, Citation2004). A retrospective investigation of 382 children with DS indicated that nearly half of the infants tested (46.1%) did not pass a newborn hearing screening and of those identified, 88.2% had a conductive hearing loss (Park, Wilson, Stevens, Harward, & Hohler, Citation2012). Medical management of middle ear disease can reduce the frequency and severity of chronic conductive loss; however, the audiologic profiles of adults with DS suggest that hearing acuity can be an ongoing concern (Evenhuis, Theunissen, Denkers, Verschuure, & Kemme, Citation2001). Chapman, Seung, Schwartz, and Bird (Citation2000) report significant associations between hearing status and intelligibility.
Motor speech disorders as an explanatory construct for reduced intelligibility in persons with Down syndrome
The research cited above is a sample of the database of studies of intelligibility in DS. At present, there is no consensus on an explanatory construct to guide treatment of reduced intelligibility in DS. One potential explanatory construct is a speaker’s motor speech diagnostic classification status. Although some type of motor component has been specified or implied as a primary source of reduced intelligibility in the DS literature, there appears to be no research documenting associations between specific motor speech classifications and the intelligibility status of persons with DS. For example, in a study of adult men with DS using a single-word intelligibility task, simplification of clusters in both the word initial and word final position, and contrasts involving tongue-posture, control, and timing were the variables most negatively affecting intelligibility (Bunton, Leddy, & Miller, Citation2007). The authors concluded that the observed errors provide support for ‘motor speech disorder’ as a primary cause of lowered intelligibility in DS.
The present question is whether a speaker’s diagnostic motor speech classification status may provide the most informative basis to explicate speech processing sources of reduced intelligibility in persons with DS, and accordingly, the most effective construct on which to base treatment. The motor speech classification framework for the present research (Shriberg, Kwiatkowski, & Mabie, Citation2019, ) posits five motor speech classifications: a representational delay or deficit that may account for reduced intelligibility in speakers with No Motor Speech Disorder (No MSD), a developmental delay in the execution of precise and stable speech, prosody, and voice (Speech Motor Delay [SMD]), a more pervasive and persistent disorder in speech execution (Childhood Dysarthria [CD]), a disorder in speech planning/programming (Childhood Apraxia of Speech [CAS]), and concurrent Childhood Dysarthria and Childhood Apraxia of Speech (CD & CAS). The term explanatory construct refers to the neuromotor correlates of delays or deficits in the two motor speech processes – planning/programming (transcoding) or execution – for understanding and treating reduced intelligibility. Comparative discussion of alternative classification systems for childhood speech sound disorders is beyond the scope of the present focus on intelligibility in adolescents with DS.
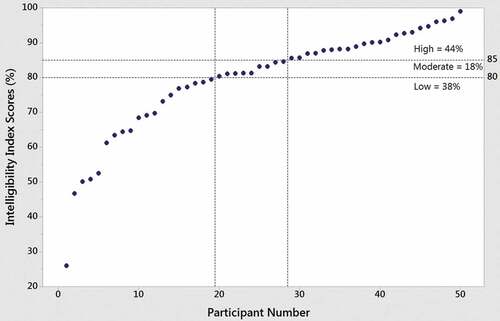
Figure 1. Intelligibility Index (II) scores and ordinal intelligibility index (OII) classification findings for 50 adolescents with Down syndrome.
An ordinal measure of intelligibility
Comparative discussion of alternative measurement approaches to intelligibility in research on persons with DS is also beyond the scope of the present focus. Two considerations motivated the development of an intelligibility measure termed the Ordinal Intelligibility Index (OII) for use in the present study. First, findings from prior research suggested that in contrast to single-word or sentence repetition tasks, conversational speech samples provide the only context that includes the contributions of propositional language, speech, fluency, prosody, and voice to generalizations about intelligibility (Morrison & Shriberg, Citation1992). Consequently, an interval-level, conversational speech measure termed the Intelligibility Index (II) was developed for research and clinical use in speech sound disorders (Shriberg, Citation1993). II percentage scores are calculated by dividing the number of intelligible words in a conversational speech sample by the total number of words produced, multiplied by 100.
The second consideration was that an analysis of II scores from a database of 346 speakers with one of eight types of complex neurodevelopmental disorders (Shriberg, Strand, Jakielski, & Mabie, Citation2019) indicated that their II scores were not normally distributed. Rather than using statistical transformations to normalize II scores for the present study, a three-classification ordinal scale of intelligibility (OII) was determined to be the optimum fit to the II data from participants in each of the eight groups: Low intelligibility OII = 0% – 79.9% II scores, Moderate intelligibility OII = 80% – 84.9% II scores, and High intelligibility OII = 85% – 100% II scores. These intelligibility cut-off percentages for the OII are generally comparable to those described in Hustad (Citation2016) for ordinal scaling of the intelligibility of children with cerebral palsy. For comparison, in a technical report providing reference data for speech in conversational samples, all 40 typically-developing 3- to 6-year-old boys and girls in the report had II scores above 95.5% (Potter et al., Citation2012). In addition to the three levels of intelligibility in the OII, the cover term reduced intelligibility is used hereafter to refer to speakers with either Moderate or Low intelligibility on the OII.
Statement of purpose
The well-documented intelligibility deficits in persons with DS and the substantial prevalence of motor speech disorders in adolescents with DS recently reported in Wilson, Abbeduto, Camarata, and Shriberg (Citation2019) motivated the questions posed in the present report. Findings in Wilson et al. (Citation2019) indicated that nearly all (97.8%) of the 45 classifiable adolescents with DS in the sample met diagnostic classification criteria for one of the four types of motor speech disorders described previously. In order of prevalence within the sample, 37.8% of the participants met criteria for CD, 26.7% met criteria for SMD, 22.2% met criteria for CD & CAS, and 11.1% met criteria for CAS. The one remaining participant (2.2%) was classified as having No MSD. Among participants with CD, with or without concurrent CAS, the most prevalent subtype was Ataxia. Using data from this sample, data from the OII, and comparison data from two other groups of speakers, the following two questions were posed:
In a sample of adolescents with Down syndrome, are there statistically significant associations between any one or more risk factors and reduced intelligibility, or between types of motor speech disorder and reduced intelligibility?
Method
Participants and procedures
A previous report by Wilson et al. (Citation2019) describes the procedures used to recruit and assess an original sample of 50 American-English speaking adolescents with DS, the perceptual and acoustic procedures used by four transcribers and acoustic analysts to reduce the speech, prosody, and voice data, and reliability estimates within and among the transcribers and acoustic analysts. The Supplement for each of the six papers in the present issue of Clinical Linguistics & Phonetics [Supplementary Data] includes information on the methods and measures used to classify participants’ speech and motor speech status. Readers may wish to consult the prior article, the Appendix for the prior article, and the Supplement. The original sample was reduced to 45 participants for the primary analyses. Five of the original participants, each of whom did not have the required number of pause opportunities to classify their status on the CAS marker described in the Supplement, were excluded from the primary analyses. Comparison intelligibility data from studies of motor speech disorders in 415 participants with idiopathic Speech Delay (SD: Shriberg, Kwiatkowski, & Mabie, Citation2019) and 301 participants with complex neurodevelopmental disorders (Shriberg, Strand, et al., Citation2019) are used for one intelligibility analysis.
Statistical analyses
Due to the low power to detect true significant differences associated with the small cell sizes in the present dataset, the inferential statistical analyses to follow were treated family-wise (i.e., without adjustments for multiple tests; see Feise, Citation2002; Nakagawa, Citation2004; Perneger, Citation1998). Interpretation of findings is based on the pattern of significant Hedges-corrected effect sizes for continuous variables (Hedges & Olkin, Citation1985), and Cohen’s (Citation1988) procedure to calculate effect sizes from tests of proportions. Effect sizes with confidence intervals that do not cross 0.00 were classified as statistically significant.
Results and discussion
Intelligibility findings
is a display of the II scores and OII classifications for the original sample of all 50 children with DS, including the 5 participants whose motor speech status could not be classified due to insufficient data to complete the measure used to classify a speaker as having CAS (Wilson et al., Citation2019). Two of the five participants excluded from further analyses in the present paper met OII criteria for High intelligibility and the other three met criteria for Low intelligibility. As shown in , 44% of the original 50 participants met the criterion for High intelligibility, 18% met the criterion for Moderate intelligibility, and 38% met the OII criterion for Low intelligibility. Thus, consistent with other studies of intelligibility in adolescents with DS, over half (56%) of the speakers in the present original sample of 50 participants had reduced intelligibility as defined using the OII. Specifically, over half had fewer than 85% intelligible words in a sample of their conversational speech.
Demographic, intelligence, and language variables and intelligibility
is a summary of findings assessing associations between demographic, intelligence, and language variables and participants’ intelligibility status on the OII. Statistical tests on all variables were completed for two comparisons. First, for each variable, tests compared the percentages of participants (for categorical variables) or scores of participants (for continuous variables) with Low compared to High intelligibility. Second, for each variable in , tests compared the percentages or scores of participants with reduced (Low + Moderate) intelligibility to the percentages or scores of participants with High intelligibility. The larger number of participants in the second set of dichotomized comparisons had less sensitivity to participants with more severe intelligibility deficits (i.e., < 80% OII scores), but greater statistical power. Statistically significant confidence intervals in (i.e., intervals not crossing zero) and their effect sizes are bolded, with effect sizes classified by Cohen’s (Citation1988) conventional criteria: Small (0.20–0.49), Medium (0.50–0.79), and Large (≥0.80).
Table 1. Risk factors and intelligibility findings for 45 participants with Down syndrome.
Sex
Some studies have reported more prevalent or severe intelligibility deficits in males than females with DS (e.g., Kumin, Citation2006; Martin, Klusek, Estigarribia, & Roberts, Citation2009; Roberts et al., Citation2005; Wild et al., Citation2018). Trends in the descriptive statistics in the first six rows of are consistent with these findings, but none of the inferential statistical findings for the six ways to test for sex differences in intelligibility were significant.
Age
Associations between intelligibility and age, which have been well studied in the DS literature, suggest that reduced intelligibility may persist throughout the life span (Coppens-Hofman et al., Citation2012; Kent & Vorperian, Citation2013; Kumin, Citation1994, Citation2006; Wild et al., Citation2018). Wild et al. (Citation2018) reported persistent challenges with intelligibility in individuals with DS, although the authors described an improvement in speech intelligibility with age, particularly between 4 and 16 years of age. Findings from the current research () indicate no significant age difference in the mean ages of participants with Low or reduced compared to High intelligibility in tests using both chronological and non-verbal age. Unlike other studies, the chronological age range of the present participants is limited to 10–20 years.
Intelligence
Few studies of persons with DS have addressed associations between specific cognitive impairments and intelligibility using contemporary measures of each variable. The present non-significant difference in the mean intelligence findings for participants with High compared to Low intelligibility is consistent with findings reported by Dodd and Thompson (Citation2001) and Cleland, Wood, Hardcastle, Wishart, and Timmins (Citation2010), with both of the latter studies reporting non-significant associations between specific cognitive impairments and intelligibility.
Language
Potential associations between language variables and intelligibility in individuals with DS have been reported (see Martin et al., Citation2009 for review), but few associations have been confirmed. Findings in the current study, which included four global measures of language, did not yield significant associations between language scores and intelligibility status.
Speech disorder classifications and intelligibility
is a descriptive summary of intelligibility findings for participants with DS whose speech and motor speech classifications at assessment were cross-classified using the Speech Disorders Classification System (SDCS).
Table 2. Intelligibility findings for 45 participants with Down syndrome classified by their speech and motor speech status.
Normal(ized) speech acquisition and intelligibility
The one participant with DS whose phonemic competence met criteria for Normal(ized) Speech Acquisition was a 16-year-old female who also met motor speech criteria for CD and OII criteria for High intelligibility. These cross-classification findings illustrate the independence of speech classifications and motor speech classifications at assessment. For the present focus, they underscore the complex of risk factors, speech characteristics, and motor speech characteristics that may contribute to an individual speaker’s reduced intelligibility.
Persistent speech errors and intelligibility
As shown in , two participants – one female, 17 years of age and the other a male, 18 years of age – met criteria for Persistent Speech Errors. The first participant met criteria for SMD and Moderate intelligibility; the second met criteria for CAS and High intelligibility. Again, findings illustrate the possible direct, moderating, or mediating effects of correlates of types of speech, prosody, and voice behaviours that may impact intelligibility in persons with DS.
Persistent speech delay and intelligibility
All of the 42 participants in with Speech Delay/Persistent Speech Delay (PSD) were over 9 years of age (i.e., had PSD). The intelligibility findings in the right-most two columns suggest that they had approximately similar percentages of Low or reduced intelligibility compared to the percentage with High intelligibility. Statistical tests of these percentages were not completed because the cell sizes were too small to covary the intelligibility findings by participants’ motor speech classifications. That is, as reviewed next, the type and number of participants with each of the five motor speech classifications likely moderated the intelligibility findings for the participants in with PSD.
Motor speech disorder classifications and intelligibility
The motor speech findings in the Totals for each of the five columns in were used to address the second part of the question posed in the Statement of Purpose: Are there statistically significant associations between any one or more types of motor speech disorder and reduced intelligibility in a sample of adolescents with Down syndrome?
includes descriptive statistics for participants meeting criteria for each of the four types of motor speech disorders, with the appropriate denominators used to calculate the percentages of participants with Low and Low + Moderate (reduced) intelligibility. The two right-most columns in include the confidence intervals and conservative two-tailed effect sizes testing the hypothesis that the proportion of participants with Low or Low + Moderate intelligibility compared to the proportion with High intelligibility in each motor speech disorder group is 0.50. The bolded values indicate two-tailed statistically significant comparisons (Cohen, Citation1988) and the magnitude of significant effect sizes using Cohen’s conventional adjectives.
Table 3. Intelligibility findings for 45 participants with Down syndrome classified by their motor speech status.
No motor speech disorder
The one participant meeting classification criteria for No MSD in was a 20-year-old male with PSD and High intelligibility. Due to the lack of group data for analyses, it is not known what percentage of speakers with DS and No MSD would have lowered intelligibility compared to the present intelligibility data for speakers with the four types of motor speech disorders.
Speech motor delay
includes the descriptive and inferential statistical findings for the intelligibility status of the 12 participants meeting the SDCS criterion for SMD. A total of 2 of the participants had Low intelligibility, 2 had Moderate intelligibility, and 8 had High intelligibility. When percentaged as shown in , the percentage with High intelligibility (80%) was significantly higher than the percentage with Low intelligibility (20%), but not significantly higher than the percentage with Low + Moderate intelligibility (33.3%).
Notice that the two descriptive findings, one of which was significant, are counterintuitive, with significantly more speakers with SMD having High rather than Low intelligibility. The imprecise and unstable speech, prosody, and voice errors that characterize SMD evidently did not have the same consequences for intelligibility as the phonemic errors (i.e., deletions, substitutions) and the types of inappropriate prosody and voice signs that characterize the three types of motor speech disorders discussed next. Alternatively, as is a caution for all statistical analyses with small cell sizes in the present report, the intelligibility finding for SMD may be a chance finding that does not replicate in additional data sets.
Childhood dysarthria
For the 17 participants in meeting SDCS criteria for CD, 7 had Low intelligibility, 3 had Moderate intelligibility and 7 had High intelligibility. Thus, 58% of the participants with DS and CD had reduced intelligibility, compared to 41.2% with High intelligibility; the difference was not statistically significant. Later analysis reports findings for subtypes of dysarthria in relation to intelligibility.
Childhood apraxia of speech
For the 5 participants in with CAS, 3 had Low intelligibility, none had Moderate intelligibility and 2 had High intelligibility. These findings – that 60% of the participants with DS and CAS had lowered intelligibility compared to 40% with DS and CAS with High intelligibility – were non-significant.
Childhood dysarthria & childhood apraxia of speech
For the 10 participants in with CD & CAS, 4 had Low intelligibility, 4 had Moderate intelligibility and 2 had High intelligibility. Thus 80% of the participants with DS and persistent CD & CAS had reduced intelligibility, compared to 20% with High intelligibility. As shown in , the difference was statistically significant (effect size: 0.644). This finding is interpreted to support the hypothesis that it is the speech, prosody, and voice signs of concurrent CD and CAS that may provide the strongest explanatory construct for the frequent intelligibility impairments in persons with DS. The interpretation is that these speech, prosody, and voice errors associated with CD & CAS are additive, relative to their contribution to reduced intelligibility. As noted in Shriberg, Kwiatkowski, and Mabie (Citation2019), the increasing reports of concurrent dysarthria in the genetic CAS literature, notably the FOXP2 literature, may suggest directions for including intelligibility variables in speech-genetics research.
Childhood dysarthria, childhood apraxia of speech, and childhood dysarthria & childhood apraxia of speech
The final two rows in provide descriptive and inferential intelligibility findings for all participants in the present sample who met criteria for either one or for both of the two conventional motor speech disorders, CD and CAS. For the 32 participants in who met this criteria, 14 had Low intelligibility, 7 had Moderate intelligibility and 11 had High intelligibility. As shown in , the difference between the percentages of the participants with Low (56%) and High (44%) intelligibility was not significant. However, the difference between the percentages of all 32 participants with reduced (65.6%) compared to High (34.4%) intelligibility was significant (effect size: 0.318). Notice that the previous analyses assessed the additive effects of CD and CAS in the same 10 speakers, whereas in the present analyses 22 of the 32 speakers had only CD or only CAS.
Subtypes of dysarthria
is a graphic summary of findings addressing the possible association of intelligibility status and subtypes of dysarthria. includes the averaged subtype index scores of the 20 participants with DS who met criteria for CD or CD & CAS. A total of 9 of the 20 participants had High intelligibility and 11 had Low intelligibility. includes the averaged percentile scores for the subtype indices, using the methods described in Wilson et al. (Citation2019) and in the Supplement. Scores are arranged from lowest to highest values in each panel, with lower scores/percentiles indicating greater support for the dysarthria subtype.
Figure 2. Subtypes of dysarthria as explanatory constructs for low intelligibility in adolescents with Down syndrome. Panel A includes the mean percentage scores on each of the dysarthria subtype indices for participants with high and low intelligibility, and panel B includes the mean percentile scores on each index for participants with high and low intelligibility.
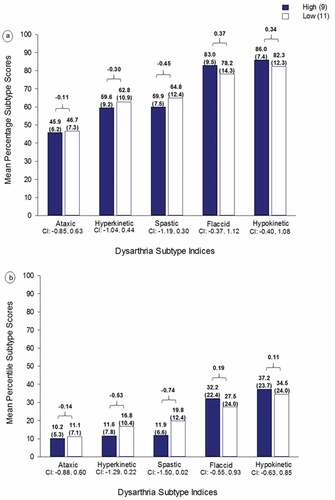
As shown in the confidence intervals overlapping 0.00 under each subtype in both , none of the effect sizes for the pair-wise comparisons were significant. Thus, in the present sample of 20 participants with DS with CD or CD & CAS, their averaged scores on the dysarthria subtype indices were not associated with their intelligibility classification on the OII.
There are several constraints in these preliminary data. First, due to limited cell sizes, the data for participants meeting criteria for CD and CD & CAS are combined, with the attendant effects of both disorders on their intelligibility classification. Second, most of the 20 participants would be classified as having mixed dysarthria, with a participant’s dysarthria subscale index scores meeting criteria for more than one of the five subtypes of dysarthria. Thus, the intelligibility status of such participants may reflect the contributions of the specific mix of subtypes. Additional research with sufficient sample sizes is needed to test the intelligibility classifications of participants meeting criteria only for CD, and meeting dysarthria subtype criteria for only one of the five subtypes. The most frequent subtype of dysarthria in the present sample of adolescents with DS, ataxic dysarthria (see Wilson et al., Citation2019), is of foremost interest. As noted in the prior paper, Kent and Vorperian (Citation2013) review reports features of ataxic or flaccid dysarthria secondary to the hypotonia reported in individuals with DS.
Motor speech disorders and intelligibility in two comparison datasets
provides comparative information on motor speech disorders as a potential explanatory construct for reduced intelligibility in three study groups. is a display of the present intelligibility findings for participants with DS meeting criteria for each of the five motor speech classifications. includes intelligibility findings by motor speech status of 301 speakers with seven types of complex neurodevelopmental disorders (Shriberg, Strand, et al., Citation2019 [i.e., excluding the present findings for DS]). includes intelligibility findings by motor speech status of 415 speakers with idiopathic SD (Shriberg, Kwiatkowski, & Mabie, Citation2019). The primary observation about the comparative findings in is support for the high prevalence of reduced intelligibility in adolescents with DS, compared to the percentage of participants with reduced intelligibility in each of the other study samples. The adolescents with DS in the present sample more frequently had Moderate and especially Low intelligibility.
Figure 3. Comparative information on diagnostic classifications of motor speech status as an explanatory construct for reduced intelligibility in adolescents with Down syndrome. Figure 3a includes intelligibility findings for 45 speakers with DS in the original sample. Figure 3b includes intelligibility findings for 301 speakers with seven types of complex neurodevelopmental disorders (Shriberg, Strand, et al., Citation2019). Figure 3c includes intelligibility findings for 415 speakers with idiopathic Speech delay (Shriberg, Campbell, et al., Citation2019). No MSD: No Motor Speech disorder; SMD: Speech Motor delay; CD: Childhood Dysarthria; CAS: Childhood Apraxia of Speech: CD & CAS: Concurrent CD & CAS.
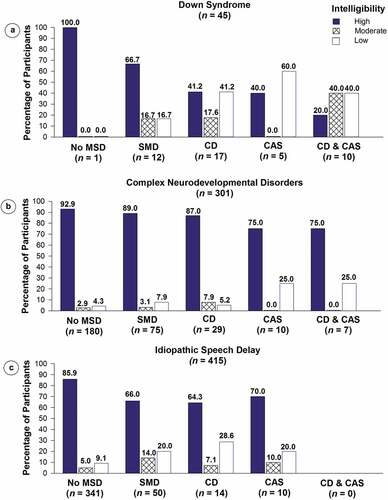
A second observation is on the intelligibility findings in for participants with No MSD in each of the two comparison study samples. Recall that the intelligibility status of adolescents with DS with this classification could not be assessed in the present study because there was only one participant with No MSD. As shown in , most of the participants with No MSD in the two comparison groups had High intelligibility, including 92.9% of the participants with complex neurodevelopmental disorders and 85.9% of the participants with idiopathic SD. These findings are interpreted as support for motor speech disorder as an explanatory construct for reduced intelligibility in adolescents with DS, as well as for reduced intelligibility in other clinical populations.
Speech, prosody, and voice signs and intelligibility
– provide a representative sample of findings selected to highlight significant speech, voice, and prosody differences between participants with DS with High compared to those with Low intelligibility in conversational speech. Some of the findings discussed in the following sections replicate findings reported in the literature on intelligibility in persons with DS; other findings appear to be unique to the present methods and measures. Data from participants with Moderate intelligibility were not included in these analyses to be maximally sensitive to speakers at the low end of the distribution of intelligibility in (i.e., below 80% intelligible words in conversational speech).
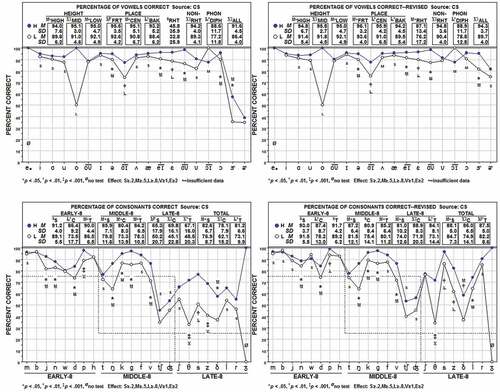
Figure 4. Four measures of consonant and vowel production in Conversational Speech (CS) in adolescents with Down syndrome. In each of the four panels, filled circles indicate participants with High (H) intelligibility; open circles indicate participants with Low (L) intelligibility. Statistically significant comparisons in the upper numeric section of each panel are indicated both by boxes around them and by effect size information.
Speech findings
Research on the contributions of individual and classes of speech sounds to intelligibility suggest that some vowel and consonant feature classes and individual vowels and consonants may have more significant impact on intelligibility than other feature classes or phonemes, with implications for the selection of treatment targets. For example, Bunton and Leddy (Citation2011), and Wild et al. (Citation2018) provide informative discussions of anatomic, physiologic, and tactile correlates of reduced vowel space associated with persistent intelligibility deficits in some adolescents with DS, including rationale for the contribution of spatiotemporal errors on specific vowel feature classes to intelligibility deficits. The four panels in include vowel and consonant data obtained from four measures of speech in conversation that bear on these issues. The panels include summary findings for the Percentage of Vowels Correct, the Percentage of Vowels Correct-Revised, the Percentage of Consonants Correct, and the Percentage of Consonants Correct-Revised. The first and third measures score speech sound deletions, substitutions, and distortions as incorrect, whereas the second and fourth score only deletions and substitutions as incorrect.
As shown for the Percentage of Vowels Correct (), the averaged vowel (including diphthongs) accuracy of the 19 participants with DS in the Low intelligibility subgroup was significantly lower (86.4% [4.0]) than the averaged vowel accuracy of the 22 participants in the High intelligibility group (91.6% [4.5]); effect size: >1.0). Note that as shown in the graphic section below these findings, vowel errors in the participants with Low intelligibility can be characterized as an ‘across-the-board’ deficit. Specifically, in comparison to participants with High intelligibility, participants with Low intelligibility had significantly lower vowel accuracy on each of the three Height features, each of the three Place features, and nearly all vowels and diphthongs. A significant, across-the-board difference between participants in the two intelligibility groups also occurred on Percentage of Vowels Correct-Revised scores, also with an approximately five percentage point difference in the total scores. The significant difference between Low and High intelligibility groups on the Percentage of Vowels Correct-Revised indicates that in comparison to participants in the High intelligibility group, participants with DS in the Low intelligibility group more frequently deleted vowels (i.e., syllables) and substituted vowels (i.e., in addition to the average of five percentage points in the Percentage of Vowels Correct that reflect vowel distortions). Possible explanations for the difference in the present across-the-board vowel findings compared to the feature-class findings reported in studies that assess intelligibility in single-word tasks include language and prosodic variables that mediate speech intelligibility and comprehensibility when sampled in propositional speech. Some examples of the latter are the stress assignments that affect articulation of vowels in propositional speech (e.g., unstressed vowels in function words and syllables with secondary and tertiary stress in multisyllabic words).
Consonant accuracy findings for the participants in the Low intelligibility group in can also be summarized as a significant, across-the-board deficit. As shown in , the average Percentage of Consonants Correct score for participants in the Low intelligibility group (73.1% [9.9]) was significantly lower on this measure than the score for participants in the High intelligibility group (81.2% [6.6]; effect size: >0.80). Notably, with the exception of Early-8 singletons, participants with Low intelligibility had significantly lower Percentage of Consonants Correct scores than participants with High intelligibility on singletons and clusters in the Early-8, Middle-8, and Late-8 developmental sound classes. The absolute differences in accuracy between Low and High intelligibility groups were greatest for Late-8 consonant singletons and clusters.
As shown for vowels in , findings in provide information on the consequences for intelligibility of phonemic changes. As previously indicated, the Percentage of Consonants Correct-Revised scores only deletions and substitutions as incorrect. The average Percentage of Consonants Correct-Revised score for participants in the Low intelligibility group (82.2% [8.6]) was significantly lower than the score on this measure for participants in the High intelligibility group (85.5% [5.0]; effect size: >0.50). These findings indicate that in addition to their phonetic distortions, the latter group are making significantly more phonemic deletions and substitution errors in singletons and clusters across all developmental sound classes, again with implications for target selection in treatment planning.
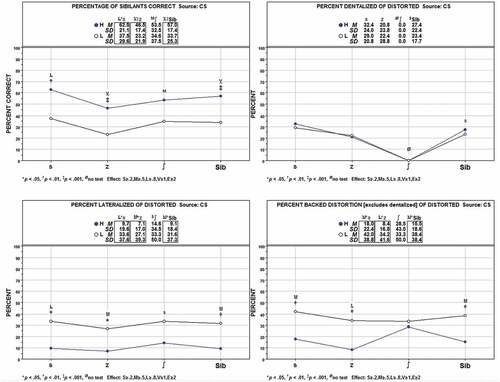
illustrates a significant feature of the speech of adolescents with DS with Low intelligibility – a high percentage of speech sound distortions on sibilants other than the dentalized sibilants that are common in children with idiopathic SD. Sibilants occur frequently in English and are important for comprehensibility, with /s/ and /z/ marking many grammatical forms (e.g., plurals, possessives, third person simple present tense). The trends in for speakers in the Low intelligibility group indicate significantly lower percentages of correct sibilant sounds (/s/, /z/, and /ʃ/) than produced by speakers in the High intelligibility group (effect size: >1.0). Notably, as shown in , the two groups did not differ in their percentage of dentalized distortions of sibilants. As shown in , however, speakers with Low intelligibility had a significantly higher percentage of lateralized sibilant distortions compared to the speakers with High intelligibility (effect size: >0.5). As shown in , speakers with low intelligibility also had significantly higher percentages of backed distortions than speakers with High intelligibility (effect size: >0.5). These findings implicate the likely negative contributions of these and other less common speech sound distortions to a speaker’s intelligibility and comprehensibility.
Figure 5. Sibilant distortions and intelligibility in Conversational Speech (CS) in adolescents with Down syndrome. Filled circles indicate participants with High (H) intelligibility; open circles indicate participants with Low (L) intelligibility.
Prosody and voice findings
In addition to the lowered accuracy of speech production, including vowel/diphthong errors in all feature classes, consonant errors of all types on all three developmental classes, and common and less common distortion errors, prosodic and voice deficits have been associated with low intelligibility in adolescents with DS (Kent & Vorperian, Citation2013). provides a summary of prosody and voice findings for the present participants with High and Low intelligibility. Data were obtained from prosody and voice coding of the conversational speech samples using a measure termed the Prosody-Voice Screening Profile that provides perceptually-based scores on seven dimensions of prosody and voice (Shriberg et al., Citation2010; Shriberg, Kwiatkowski, & Rasmussen, Citation1990). The three panels in are summaries of Prosody-Voice Screening Profile findings for Prosody (Phrasing, Rate, Stress) and Voice (Loudness, Pitch, Laryngeal Quality, Resonance).
Figure 6. Inappropriate prosody and voice and intelligibility in Conversational Speech (CS) in adolescents with Down syndrome. Filled circles indicate participants with High (H) intelligibility; open circles indicate participants with Low (L) intelligibility. See text for description of the data in each panel.

Beginning with the Prosody findings in , there was no significant difference between participants in the High and Low intelligibility groups in the percentage of utterances in conversation with appropriate Phrasing (i.e., repetitions and/or revisions of sounds, syllables, and words). Participants in both the High and Low intelligibility groups had Phrasing scores in the marginal (80%-89.9%) range on this prosodic variable. As shown in the numeric and graphic sections of , there were significant between-group intelligibility group findings for Rate and Stress. Participants in the Low intelligibility group averaged significantly fewer utterances with appropriate Rate (73.3%) and Stress (62.3%) compared to the average percentages for participants in the High intelligibility group (85.6% and 76.3%, respectively); respective effect sizes: >0.5 and >0.8.
provides additional information on the significant Rate and Stress findings. As shown, the Rate difference was due to speakers in the Low intelligibility group having a significantly higher percentage of utterances coded ‘9’ (see horizontal axis in ), which is the code for ‘Slow Articulation/Pause Time.’ Thus, speakers in the Low OII group had slower averaged syllables per second rates than the 2–4 syllables per second rates typical for their chronological age and sex (Potter et al., Citation2012; Scheer-Cohen et al., Citation2013). The Slow Articulation component of the code is generally viewed as associated with motor speech constraints and the increased Pause Time as associated with cognitive-linguistic constraints (Shriberg et al., Citation1990). As also shown in , the inappropriate Stress finding in is associated with significantly higher percentages of utterances coded as ‘15’ (‘Excessive/Equal/Misplaced’ Stress). Excessive/Equal Stress is posited to indicate deficits in both neurocognitive (linguistic stress assignment) and neuromotor (force regulation) speech processing. These two deficits in Rate and Stress are central to definitions of dysarthria and apraxia of speech.
Last, as shown in , both the High and Low intelligibility groups of adolescents with DS had a high percentage of utterances (approximately 25%) coded as ‘Rough’ (Code '24' in ), a widely studied feature of DS (Kent & Vorperian, Citation2013). Both High and Low intelligibility groups also had significantly low percentages of utterances with appropriate Resonance (: 33.6% and 29.7%, respectively). As reviewed previously, craniofacial aspects of DS affect resonance, including both nasality (for participants with Low intelligibility; Code '30' in ), and for both groups, a type of resonance termed 'Nasopharyngeal' (Code '32' in ; Shriberg et al., Citation1990).
Summary and conclusions
Summary
A total of 38% or over one-third of the 45 participants in the present sample of adolescents with DS met criteria for Low intelligibility. Together with the 18% of participants with Moderate OII scores, 56% or over half of the participants in the present study experience the intelligibility challenges that have been documented in the Down syndrome literature. Reduced intelligibility was not significantly associated with the demographic, intelligence, or language variables assessed in this study or with the motor speech execution disorder termed Speech Motor Delay. Significantly more participants with dysarthria or apraxia of speech had lowered intelligibility than High intelligibility, as did a combined group of participants with either dysarthria, apraxia, or both dysarthria and apraxia. Reduced intelligibility was not significantly associated with dysarthria subtype. Consistent with the literature in DS, lowered intelligibility was significantly associated with across-the-board phonemic and phonetic errors and inappropriate prosody and voice.
Methodological considerations
Cross-validation studies to support and extend generalizations from the present findings are needed to address two methodological considerations. First, the small sample sizes for some of the present analyses constrained representativeness issues (e.g., age range, treatment histories), increased the risk for Type II errors due to power limitations, and prohibited use of multiple regression and other techniques that may have cross-validated prior or identified new direct, moderated, or mediated significant associations between variables and reduced intelligibility. A second methodological consideration is the lack of information in the present data from other assessment modalities in the speech sciences and disorders literature (e.g., kinematics, neuroimaging) that may have cross-validated prior findings or provided new insights on neuromotor processes underlying reduced intelligibility.
Research and clinical implications
The research implications of the initial support for substantial prevalence of motor speech disorders in Down syndrome (Wilson et al., Citation2019), and the present initial support for Childhood Dysarthria and Childhood Apraxia of Speech as explanatory constructs for the reduced intelligibility in persons with DS would appear to be straightforward. Specifically, as indicated in Results and Discussion and in the methodological considerations above, additional studies are needed to cross-validate the present initial findings and to extend findings in studies using instrumental measurement modalities.
Speculations about the clinical implications of the present findings would be premature, pending replication and extension of the current initial findings. Continuing studies to improve intelligibility in adolescents with DS have reported promising findings using instrumental treatment approaches developed for motor speech disorders (e.g., Cleland, Timmins, Wood, Hardcastle, & Wishart, Citation2009; Gibbon, McNeill, Wood, & Watson, Citation2003; Horvat, Croce, & Fallaize, Citation2016; Matthews-Brzozowska, Cudziło, Walasz, & Kawala, Citation2014; Wood, Wishart, Hardcastle, Cleland, & Timmins, Citation2009). Optimally, intelligibility and comprehensibility (e.g., Yoder, Camarata, & Woynaroski, Citation2016) programmes for persons with DS will address motor speech challenges within the larger context of successful communication (Rvachew & Folden, Citation2018).
Acknowledgments
The authors would like to thank the participants and their families for their participation in this project. Our thanks also to Loredana Bruno, Mary Camarata, Terrie Gibson, Nancy Giles, Sheryl Hall, Selma Karadottir, Heather Karlsson, Heather Mabie, Jane McSweeny, Melissa Murphy, Alison Scheer-Cohen, Susen Schroeder, Christie Tilkens, and David Wilson.
Supplemental Material
Download PDF (801 KB)Disclosure Statement
The authors report no declarations of interest.
Supplemental data
Supplemental data for this article can be accessed on the publisher’s website.
Additional information
Funding
References
- Barnes, E., Roberts, J., Long, S. H., Martin, G. E., Berni, M. C., Mandulak, K. C., & Sideris, J. (2009). Phonological accuracy and intelligibility in connected speech of boys with fragile X syndrome or Down syndrome. Journal of Speech, Language, and Hearing Research, 52, 1048–1061. doi:10.1044/1092-4388(2009/08-0001)
- Brandt, B. R., & Rosén, I. (1995). Impaired peripheral somatosensory function in children with Down syndrome. Neuropediatrics, 26, 310–312. doi:10.1055/s-2007-979780
- Bunton, K., & Leddy, M. (2011). An evaluation of articulatory working space area in vowel production of adults with Down syndrome. Clinical Linguistics & Phonetics, 25, 321–334. doi:10.3109/02699206.2010.535647
- Bunton, K., Leddy, M., & Miller, J. (2007). Phonetic intelligibility testing in adults with Down syndrome. Down’s Syndrome, Research and Practice: the Journal of the Sarah Duffen Centre/University of Portsmouth, 12, 1–20.
- Camarata, S., Yoder, P., & Camarata, M. (2006). Simultaneous treatment of grammatical and speech comprehensibility deficits in children with Down syndrome. Down Syndrome Research and Practice, 11, 9–17. doi:10.3104/research
- Carr, J. (2012). Six weeks to 45 years: A longitudinal study of a population with Down syndrome. Journal of Applied Research in Intellectual Disabilities, 25, 414–422. doi:10.1111/j.1468-3148.2011.00676.x
- Carrow-Woolfolk, E. (1995). Oral and written language scales (OWLS). Bloomington, MN: Pearson Assessment.
- Chapman, R. S., Seung, H. K., Schwartz, S. E., & Bird, E. K. (2000). Predicting language production in children and adolescents with Down syndrome: The role of comprehension. Journal of Speech, Language, and Hearing Research, 43, 340–350. doi:10.1044/jslhr.4302.340
- Cleland, J., Timmins, C., Wood, S. E., Hardcastle, W. J., & Wishart, J. G. (2009). Electropalatographic therapy for children and young people with Down’s syndrome. Clinical Linguistics & Phonetics, 23, 926–939. doi:10.3109/02699200903061776
- Cleland, J., Wood, S., Hardcastle, W., Wishart, J., & Timmins, C. (2010). Relationship between speech, oromotor, language and cognitive abilities in children with Down syndrome. International Journal of Language and Communicative Disorders, 45, 83–95. doi:10.3109/13682820902745453
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences ((2nd ed.). New Jersey: Lawrence Erlbaum Associates.
- Connolly, J. A. (1978). Intelligence levels of Down‘s syndrome children. American Journal of Mental Deficiency, 83, 193–196.
- Coppens-Hofman, M. C., Maassen, B. A., van Schrojenstein Lantman-de Valk, H., & Snik, A. F. (2012). Speech difficulties and poor speech intelligibility in adults with Down syndrome: A review of the literature. Journal of Hearing Science, 2, 9–16.
- Coppens-Hofman, M. C., Terband, H., Snik, A. F., & Maassen, B. A. (2016). Speech characteristics and intelligibility in adults with mild and moderate intellectual disabilities. Phoniatrica et Logopaedica, 68, 175–182. doi:10.1159/000450548
- Dodd, B., & Thompson, L. (2001). Speech disorder in children with Down’s syndrome. Journal of Intellectual Disability Research, 45, 308–316. doi:10.1046/j.1365-2788.2001.00327.x
- Evenhuis, H. M., Theunissen, M., Denkers, I., Verschuure, H., & Kemme, H. (2001). Prevalence of visual and hearing impairment in a Dutch institutionalized population with intellectual disability. Journal of Intellectual Disability Research, 45, 457–464.
- Feise, R. J. (2002). Do multiple outcome measures require p-value adjustment? BMC Medical Research Methodology, 2, 8. doi:10.1186/1471-2288-2-8
- Gibbon, F. E., McNeill, A. M., Wood, S. E., & Watson, J. M. (2003). Changes in linguapalatal contact patterns during therapy for velar fronting in a 10-year-old with Down‘s syndrome. International Journal of Language & Communication Disorders, 38, 47–64. doi:10.1080/13682820304816
- Guenther, F. H. (1995). Speech sound acquisition, coarticulation, and rate effects in a neural network model of speech production. Psychological Review, 102, 594–621.
- Guenther, F. H., Hampson, M., & Johnson, D. (1998). A theoretical investigation of reference frames for the planning of speech movements. Psychological Review, 105, 611–633.
- Guimaraes, C. V., Donnelly, L. F., Shott, S. R., Amin, R. S., & Kalra, M. (2008). Relative rather than absolute macroglossia in patients with Down syndrome: Implications for treatment of obstructive sleep apnea. Pediatric Radiology, 38, 1062–1067. doi:10.1007/s00247-008-0941-7
- Hedges, L. V., & Olkin, I. (1985). Statistical methods for metaanalysis. Boston, MA: Academic Press.
- Horvat, M., Croce, R., & Fallaize, A. (2016). Information processing and motor control in Down syndrome. Journal of down Syndrome & Chromosome Abnormalities, 2, 1. doi:10.4172/2472-1115.1000107
- Hustad, K. (November, 2016). Measuring children’s intelligibility. Paper presented at the Annual Convention of the American Speech-Language-Hearing Association, Philadelphia, PA.
- Kaufman, A. S., & Kaufman, N. L. (2004). Kaufman Brief Intelligence Test – Second Edition (KBIT-2). San Antonio, TX: Pearson Assessments.
- Kent, R., & Vorperian, H. (2013). Speech impairment in Down syndrome: A review. Journal of Speech, Language, and Hearing Research, 56, 178–210. doi:10.1044/1092-4388(2012/12-0148)
- Kumin, L. (1994). Intelligibility of speech in children with Down syndrome in natural settings: Parents’ perspective. Perceptual and Motor Skills, 78, 307–313. doi:10.2466/pms.1994.78.1.307
- Kumin, L. (2006). Speech intelligibility and childhood verbal apraxia in children with Down syndrome. Down Syndrome Research and Practice, 10, 10–22. doi:10.3104/research
- Lane, H., Denny, M., Guenther, F. H., Matthies, M. L., Menard, L., Perkell, J. S., … Zandipour, M. (2005). Effects of bite blocks and hearing status on vowel production. Journal of the Acoustical Society of America, 118, 1636–1646.
- Martin, G. E., Klusek, J., Estigarribia, B., & Roberts, J. E. (2009). Language characteristics of individuals with Down syndrome. Topics in Language Disorders, 29, 112–132. doi:10.1097/TLD.0b013e3181a71fe1
- Matthews-Brzozowska, T., Cudziło, D., Walasz, J., & Kawala, B. (2014). Rehabilitation of the orofacial complex by means of a stimulating plate in children with Down syndrome. Advances in Clinical and Experimental Medicine, 24, 301–305. doi:10.17219/acem/40451
- McDaniel, J., & Yoder, P. J. (2016). Pursuing precision in speech-language pathology services for children with Down Syndrome. Seminars in Speech and Language, 37, 239–251. doi:10.1055/s-0036-1587708
- McDuffie, A., Thurman, A. J., Channell, M. M., & Abbeduto, L. (2017). Language disorders in children with intellectual disability of genetic origin. In R. Schwartz (Ed.), Handbook of child language disorders (2nd ed., pp. 52–81). New York, NY: Routledge.
- Morrison, J. A., & Shriberg, L. D. (1992). Articulation testing versus conversational speech sampling. Journal of Speech and Hearing Research, 35, 259–273.
- Nakagawa, S. (2004). A farewell to Bonferroni: The problems of low statistical power and publication bias. Behavioral Ecology, 15, 1044–1045. doi:10.1093/beheco/arh107
- Park, A. H., Wilson, M. A., Stevens, P. T., Harward, R., & Hohler, N. (2012). Identification of hearing loss in pediatric patients with Down syndrome. Otolaryngology-Head & Neck Surgery, 146, 135–140. doi:10.1177/0194599811425156
- Pennington, B. F., Moon, J., Edgin, J., Stedron, J., & Nadel, L. (2003). The neuropsychology of Down syndrome: Evidence for hippocampal dysfunction. Child Development, 74, 75–93.
- Perkell, J. S., Guenther, F. H., Lane, H., Matthies, M. L., Perrier, P., Vick, J., & Zandipour, M. (2000). A theory of speech motor control and supporting data from speakers with normal hearing and with profound hearing loss. Journal of Phonetics, 28, 233–272. doi:10.1006/jpho.2000.0116
- Perkell, J. S., Guenther, F. H., Lane, H., Matthies, M. L., Stockmann, E., Tiede, M., & Zandipour, M. (2004). The distinctness of speakers’ productions of vowel contrasts is related to their discrimination of the contrasts. Journal of the Acoustical Society of America, 116, 2338–2344.
- Perneger, T. V. (1998). What’s wrong with Bonferroni adjustments? British Medical Journal, 316, 1236.
- Potter, N. L., Hall, S., Karlsson, H. B., Fourakis, M., Lohmeier, H. L., McSweeny, J. L., … Shriberg, L. D. (2012). Reference data for the Madison speech assessment protocol (MSAP): A database of 150 participants 3-to-18 years of age with typical speech. (Tech. Rep. No. 18). Retrieved from Phonology Project website: http://www.waisman.wisc.edu/phonology/
- Roberts, J., Long, S. H., Malkin, C., Barnes, E., Skinner, M., Hennon, E. A., & Anderson, K. (2005). A comparison of phonological skills of boys with fragile X syndrome and Down syndrome. Journal of Speech, Language, and Hearing Research, 48, 980–995. doi:10.1044/1092-4388(2005/067)
- Roberts, J. E., Price, J., & Malkin, C. (2007). Language and communication development in Down syndrome. Mental Retardation and Developmental Disabilities Research Reviews, 13, 26–35. doi:10.1002/mrdd.20136
- Rvachew, S., & Folden, M. (2018). Speech therapy in adolescents with Down syndrome: In pursuit of communication as a fundamental human right. International Journal of Speech-Language Pathology, 20, 75–83. doi:10.1080/17549507.2018.1392605
- Scheer-Cohen, A. R., Holt, A. S., Karlsson, H. B., Mabie, H. L., McSweeny, J. L., Tilkens, C. M., & Shriberg, L. D. (2013). Reference data for the Madison Speech Assessment Protocol (MSAP): A database of fifty 20-to-80 year old participants with typical speech. (Tech. Rep. No. 20). Retrieved from Phonology Project website: http://www.waisman.wisc.edu/phonology/
- Shriberg, L. D. (1993). Four new speech and prosody-voice measures for genetics research and other studies in developmental phonological disorders. Journal of Speech and Hearing Research, 36, 105–140. doi:10.1044/jshr.3601.105
- Shriberg, L. D., Campbell, T. F., Mabie, H. L., & McGlothlin, J. H. (2019). Initial studies of the phenotype and persistence of Speech Motor Delay (SMD). Clinical Linguistics & Phonetics. doi:10.1080/02699206.2019.1595733
- Shriberg, L. D., Fourakis, M., Hall, S., Karlsson, H. B., Lohmeier, H. L., McSweeny, J., … Wilson, D. L. (2010). Perceptual and acoustic reliability estimates for the speech disorders classification system (SDCS). Clinical Linguistics & Phonetics, 24, 825–846. doi:10.3109/02699206.2010.503007
- Shriberg, L. D., Kwiatkowski, J., & Mabie, H. L. (2019). Estimates of the prevalence of motor speech disorders in children with idiopathic speech delay. Clinical Linguistics & Phonetics. doi:10.1080/02699206.2019.1595731
- Shriberg, L. D., Kwiatkowski, J., & Rasmussen, C. (1990). The prosody-voice screening profile. Tucson, AZ: Communication Skill Builders.
- Shriberg, L. D., Strand, E. A., Jakielski, K. J., & Mabie, H. L. (2019). Estimates of the prevalence of speech and motor speech disorders in persons with complex neurodevelopmental disorders. Clinical Linguistics & Phonetics. doi:10.1080/02699206.2019.1595732
- Thorndike, R. L., Hagen, E. P., & Sattler, J. M. (1986). Stanford-Binet intelligence scale (4th ed.). Chicago, IL: Riverside.
- Uong, E. C., McDonough, M., Tayag-Kier, C. E., Zhao, H., Mahboubi, S., Schwab, R. J., & Arens, R. (2001). Magnetic resonance imaging of the upper airway in children with Down syndrome. American Journal of Respiratory & Critical Care Medicine, 163, 731–736. doi:10.1164/ajrccm.163.3.2004231
- Valkenburg, A. J., Tibboel, D., & van Dijk, M. (2015). Pain sensitivity of children with Down syndrome and their siblings: Quantitative sensory testing versus parental reports. Developmental Medicine and Child Neurology, 57, 1049–1055. doi:10.1111/dmcn.12823
- Wild, A., Vorperian, H. K., Kent, R. D., Bolt, D. M., & Austin, D. (2018). Single-word speech intelligibility in children and adults with Down syndrome. American Journal of Speech-Language Pathology, 27, 222–236. doi:10.1044/2017_AJSLP-17-0002
- Wilson, E. M., Abbeduto, L., Camarata, S. M., & Shriberg, L. D. (2019). Estimates of the prevalence of speech and motor speech disorders in adolescents with Down syndrome. Clinical Linguistics & Phonetics.
- Wood, S., Wishart, J., Hardcastle, W., Cleland, J., & Timmins, C. (2009). The use of electropalatography (EPG) in the assessment and treatment of motor speech disorders in children with Down’s syndrome: Evidence from two case studies. Developmental Neurorehabilitation, 12, 66–75. doi:10.1080/17518420902738193
- Yoder, P. J., Camarata, S., & Woynaroski, T. (2016). Treating speech comprehensibility in students with Down syndrome. Journal of Speech, Language, and Hearing Research, 59, 446–459. doi:10.1044/2015_JSLHR-S-15-0148
- Yoder, P. J., Woynaroski, T., & Camarata, S. (2016). Measuring speech comprehensibility in students with Down syndrome. Journal of Speech, Language, and Hearing Research, 59, 460–467. doi:10.1044/2015_JSLHR-S-15-0149