
Abstract
Objective
To assess patient- and physician-reported reasons for discontinuing biologic therapy among patients with severe asthma from a real-world US cohort.
Methods
This retrospective analysis surveyed US physicians and their patients with severe asthma who were receiving/had previously received biologic therapy between August and December 2019. Physicians managing ≥3 patients with asthma per month completed surveys on disease management, demographics, exacerbation history, and biologic adherence for eligible patients. Patients could voluntarily complete a questionnaire, providing perceptions of their disease and treatment.
Results
117 physicians completed case reports for 285 patients; 85 patients had discontinued biologic therapy. Physicians (n = 85) and patients (n = 64) reported patient request (28.2% and 46.9%), shortness of breath (45.9% and 23.4%), other chronic respiratory symptoms (29.4% and 10.9%), cost/reimbursement (17.7%/9.4% and 20.3%/7.8%), and exacerbations (25.9% and 10.9%) among the main reasons for biologic discontinuation. Patients who continued biologic therapy were older (mean age 47.6 years) than those who discontinued (43.8 years), and were more likely to have ≥2 exacerbations in the previous year (52.5% vs 35.3%), allergic rhinitis (70.0% vs 62.4%), or chronic rhinosinusitis (30.0% vs 12.9%). Side effects were cited as reasons by only 15.3% and 7.8% of physicians and patients, respectively.
Conclusions
The most common reasons given for discontinuation of biologic therapy were lack of symptom control, exacerbations, cost, and patient request. These data highlight the complexity of care for this patient group and the need for ongoing, regular assessment of common challenges to biologic continuation and reasons for discontinuation, including both clinical and non-clinical factors.
Introduction
The prevalence of asthma in the US in 2018 was 19.2 million (Citation1), with an estimated 5–10% of people with asthma experiencing severe disease (Citation2). Severe asthma is defined as that requiring treatment with high-dose inhaled corticosteroids (ICS) and additional controllers and/or systemic corticosteroids to prevent it from becoming uncontrolled, or remaining uncontrolled despite this therapy (Citation2). As such, patients with severe asthma often experience persistent respiratory symptoms and exacerbations, accounting for a disproportionate use of healthcare resources, including hospitalizations, and reporting the greatest impairment in quality of life (Citation3).
Given the growing call for less reliance on long-term use of oral corticosteroids (OCS) to prevent asthma exacerbations (Citation3), patients with severe asthma often require the use of additional add-on therapies including phenotype-targeted biologics (Citation4). Available biologic treatment options for patients in the US include monoclonal antibodies targeting immunoglobulin-E (omalizumab), interleukin (IL)-5 (mepolizumab and reslizumab), the IL-5 receptor (benralizumab), and the IL-4/IL-13 receptor (dupilumab) (Citation4–9). Selecting the most appropriate biologic for a particular patient, based on specific criteria, is a key step in providing optimal disease management (Citation3).
Patients with severe asthma who are eligible to initiate specific biologic therapies are now well characterized, as are the individual factors associated with patient response to treatment (Citation10–16). Several factors influencing preference for and adherence to biologic therapies have been identified and include dosing frequency, administration route, time to onset of efficacy, and cost/insurance coverage (Citation17,Citation18). However, reasons why patients discontinue biologic therapy remain unclear (Citation19). The main objectives of this study were to describe and compare patient-reported reasons with physician-reported reasons for discontinuation of biologic therapy among patients who are prescribed biologics to treat severe asthma (primary objective) and to compare patient characteristics between those who discontinue biologic therapy and those who do not (secondary objective), to help identify barriers to treatment success in a US patient cohort with severe asthma treated with biologic therapy.
Methods
Study design
This was a retrospective analysis (GSK ID: 209643; HO-19–19596) of US data from the 2019 Adelphi Respiratory DSP, an independent, point-in-time physician and patient survey conducted between August and December 2019. The conduct of DSPs has been described previously (Citation20). In brief, physicians were identified from publicly available lists and contacted to complete a telephone screening to determine eligibility for the study. Eligible physicians then completed a survey, a 5-day workload form documenting the total number of patients seen in that time period, as well as the number of patients with specific diagnoses, and a patient record form for the next 10 consecutive eligible patients. The same patients were invited to complete a voluntary self-completion questionnaire. Patient-provided data included adherence to treatment, reasons for discontinuation, and reasons for switching. Physician-provided data included demographics, comorbidities, exacerbations, asthma medications and dosing, and adherence to asthma treatment. The DSP did not include laboratory values for phenotype, endotype, type 2 status, or lung function. All information was recorded during the survey period, from available medical history, or a specified recall period for patients. No follow-up information was collected.
The DSP survey from which this study was performed was submitted to the Western Institutional Review Board, a central international review board, where ethical exemption determination was provided. The survey was conducted with full participant consent and in accordance with the principles of the Declaration of Helsinki.
Population
This study included patients ≥18 years of age with a physician-confirmed diagnosis of severe asthma who were currently receiving or had previously received biologic therapy. Patients currently involved in a clinical trial were not eligible for inclusion. Eligible physicians had been board certified primary care or respiratory (pulmonologist/allergist) physicians for ≥5 to ≤35 years and were managing ≥3 patients with asthma per month.
Variables and outcomes
Outcome variables of interest for the primary objective were reasons for discontinuation and switching, which were provided by selecting from up to 14 available multi-choice responses (Supplementary Table 1).
Outcome variables of interest for the secondary objective were demographic and clinical characteristics, provided by the physician on the survey date or based on available medical records; exacerbation history, provided by the physician based on medical records for the 12 months prior to the survey date (0, 1, 2, or ≥3 exacerbations in the previous 12 months); perception on adherence to asthma treatment, provided on the survey date by the physician (based on the following multi-choice responses: not at all, slightly, moderately, very, and completely adherent) (Supplementary Table 1); number of biologic appointments missed in the previous 12 months, provided by the physician based on available medical records; reasons for missing biologic administration appointments in the previous 12 months, provided by the patient based on selection from 10 multi-choice responses (Supplementary Table 1).
Examination of comorbidities that increase or decrease the likelihood of prescribing biologic therapy, as reported by physicians, was an exploratory objective.
Analysis
Descriptive statistics were used for all outcomes. In addition, for discontinuation of a biologic, comparisons made were based on a matched base of patients for whom both physician- and patient-reported reasons for discontinuation were available. Mean and standard deviations (SDs) were presented for continuous variables, and frequencies and percentages were presented for categorical variables. For all outcomes, variables were described using the maximum sample available for that variable. Missing data were not imputed. Analyses were performed using IBM SPSS Data Collection Survey Reporter.
Results
Population
In total, 117 physicians completed surveys, including 79 (67.5%) pulmonologists and 38 (32.5%) allergists. More than 80% of allergists prescribed benralizumab, dupilumab, mepolizumab and omalizumab, while the proportion of pulmonologists prescribing these agents ranged from 32.9–68.4%. Of all biologics, omalizumab was prescribed by the greatest proportion of physicians overall (77.8%) and was the preferred first-line biologic of the greatest proportion of physicians (52.4%), while mepolizumab was the preferred second-line biologic of the greatest proportion of physicians (35.7%). These physicians completed patient report forms for 285 patients. Of these patients, 200 (70.2%) continued their biologic therapy of whom 79 (39.5%) had switched to another biologic therapy, and 85 (29.8%) had discontinued biologic therapy.
Of the 200 patients who continued biologic therapy, 44.5% were receiving omalizumab, 23.0% received mepolizumab, 1.0% received reslizumab, 20.5% received benralizumab, and 11.5% were on dupilumab. Of the 85 patients who have discontinued biologic therapy, none were on any biologic for their current regimen. For these discontinuers, the percentage on each biologic for their previous regimen was 63.5% for omalizumab, 23.5% for mepolizumab, 0% for reslizumab, 5.9% for benralizumab, and 7.1% for dupilumab.
Reasons for patients discontinuing or switching biologic therapy
Of the 64/85 (75%) patients who provided a reason for discontinuation of biologic therapy, the most common reasons cited were related to patient request (46.9%), no improvement in symptoms (shortness of breath [23.4%], other chronic symptoms [10.9%], and exacerbations [10.9%]), and cost/reimbursement (20.3%/7.8%) (). Among the 85 matched physicians who provided a reason for discontinuation of biologic therapy, the most common reasons cited were lack of symptom control (shortness of breath [45.9%], other chronic respiratory symptoms [29.4%], and exacerbations [25.9%]), patient request (28.2%), and costs/reimbursement (17.7%/9.4%) (). Side effects were cited as a reason for therapy discontinuation by 15.3% of physicians and 7.8% of patients ().
Figure 1. Reasons for discontinuation of biologic therapy. *Data for patients who provided a reason for discontinuation of therapy and physicians who reported a reason for their patient discontinuing therapy; †lack of control of shortness of breath/exacerbations; ‡includes all other respiratory symptoms not classifiable. OCS, oral corticosteroid.
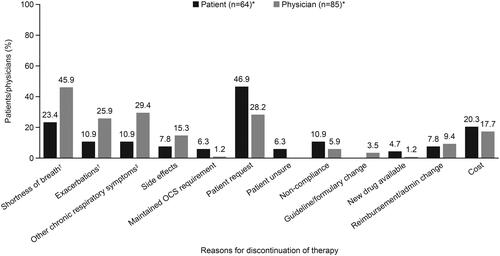
Among the 85 physicians who provided a reason for discontinuation of biologic therapy, 38 (44.7%) of these provided only one reason for discontinuation: the top three reasons provided on their own were patient request (12 patients, 14.1%), prevalence of side effects (9 patients, 10.6%), and lack of control of shortness of breath (6 patients, 7.1%).
Of the 79 patients who switched, but did not discontinue, therapy, the most common reasons cited by patients (n = 70) and physicians (n = 79) were shortness of breath, exacerbations, and other chronic respiratory symptoms. Other reasons cited for switching were side effects, maintained OCS requirement, patient request, patient unsure, noncompliance, guideline/formulary change, new drug available, reimbursement/administrative change, cost, and dosing schedule (Supplementary Figure 1).
Patient demographics and baseline characteristics
Patients who discontinued biologic therapy were younger than those who continued therapy (mean age 43.8 vs 47.6 years) and more likely to be male (52.9% vs 46.5%) (). Patients who discontinued were less likely to have allergic rhinitis (62.4% vs 70.0%) or chronic rhinosinusitis (12.9% vs 30.0%) than those who continued (). At the time of the survey, patients who had discontinued biologic therapy were being prescribed fewer concomitant asthma medications than those who continued therapy (mean [SD] 1.9 [0.90] vs 2.6 [0.92]). While OCS and ICS/LABA were prescribed in similar proportions of discontinuing and continuing patients, short-acting β2-agonists (SABAs; 81.2% vs 61.5%) and long-acting muscarinic antagonists (LAMAs; 27.1% vs 16.5%) were more often prescribed in those who discontinued than in those who continued biologic therapy ().
Figure 2. Asthma medication use at the time of the survey. ICS inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LRA, leukotriene receptor antagonist; OCS, oral corticosteroid; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist.
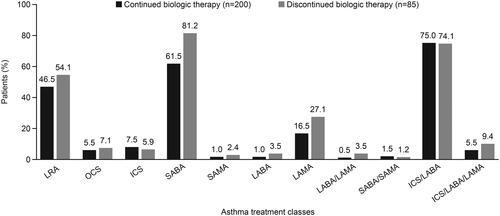
Table 1. Patient demographics and baseline characteristics.
Table 2. Patient comorbidities.
Number of exacerbations in the 12 months prior to the survey
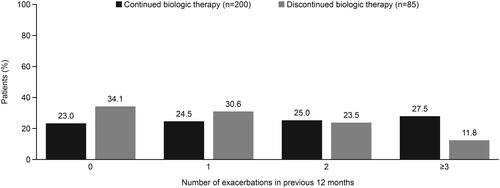
Mean (SD) exacerbation rates for the 12 months prior to the survey were 1.2 (1.2) events in patients who discontinued and 2.0 (1.9) in those who continued biologic therapy. During this period, patients who discontinued biologic therapy generally had fewer exacerbations than those who continued, with 34.1% and 23.0% experiencing no exacerbations, and 11.8% and 27.5% ≥3 exacerbations, respectively ().
Figure 3. Exacerbations in the previous 12 months.
Adherence to therapy
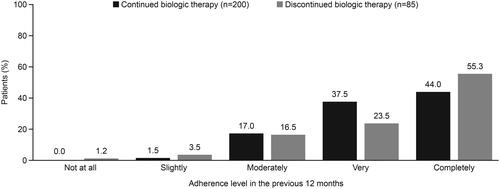
Physicians reported that 55.3% (47/85) of patients who discontinued biologic therapy were completely adherent to asthma therapy in the prior 12 months and 23.5% (20/85) were very adherent (). Of the 200 patients who continued biologic therapy, complete adherence for all asthma treatments was reported in 44.0% (88/200) and 37.5% (75/200) were reported to be very adherent ().
Figure 4. Patient adherence to therapy.
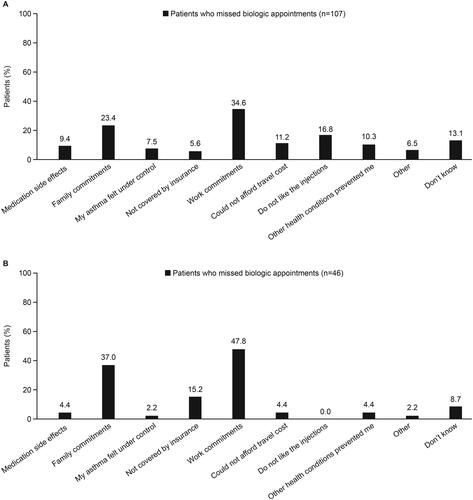
In total, 164 patients provided information on missed biologic administration appointments in the 12 months prior to the survey, 120 who had continued biologic therapy and 44 who had discontinued therapy. Among these patients, the mean (SD) number of biologic administration appointments missed, as reported by the patients themselves, was 0.6 (0.98) in those who continued biologic therapy and 0.7 (1.5) in those who discontinued. Among the 107 patients who provided reasons for missing their biologic administration appointments, patients most commonly reported absence due to work commitments (n = 37/107 [34.6%]) or family commitments (n = 25/107 [23.4%]) (). In the 46 physician reports of reasons for missing a biological appointment, work commitments (n = 22/46 [47.8%]) and family commitments (n = 17/46 [37%]) were also the most common reasons for missing a biological appointment ().
Figure 5. Patient (A) and physician (B)-reported reasons for missing a biologic administration appointment.
Most common comorbidities associated with a physician prescription for biologic
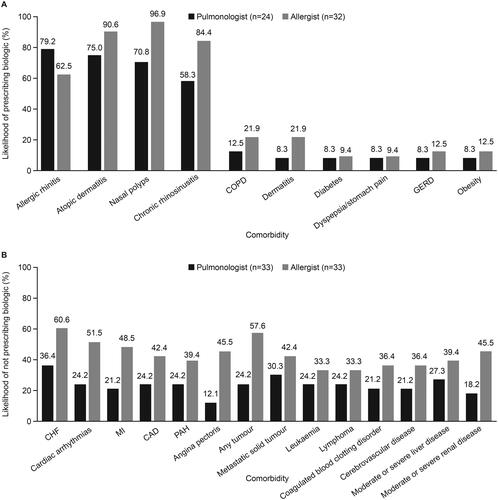
Based on the physician surveys, allergic rhinitis, atopic dermatitis, nasal polyps, and chronic rhinosinusitis were the most common comorbidities that increased the likelihood of a physician prescribing a biologic (). The most common comorbidities decreasing the likelihood of a physician prescribing a biologic were cardiac disorders and neoplasms (). The presence of certain comorbidities, namely cardiovascular disorders, malignancy, coagulopathy, and liver or kidney disease, decreased the likelihood of allergists versus pulmonologists in prescribing biologics for asthma ().
Figure 6. Comorbidities (A) increasing and (B) decreasing the likelihood of physician prescribing of biologics. CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease; MI, myocardial infarction; PAH, pulmonary arterial hypertension.
Discussion
Clinical management of patients with severe asthma is challenging given the heterogeneity and severity of this disease state. Randomized controlled trials and real-world data support the clinical benefits of biologic therapy in this patient group (Citation4); however, an understanding of the reasons for discontinuing treatment in real-world settings may help to predict triggers for this decision and allow a tailored approach to care. This is the first study with the primary aim of assessing patient- and physician-reported reasons for discontinuing biologic therapy in a real-world severe asthma population.
Some care pathways suggest assessment of biologic continuation after a short course of treatment (e.g. less than 4 months) and assessment of the appropriateness of discontinuation after a longer course of treatment (e.g. 3 years) (Citation21). However, there are no data supporting a validated stopping rule for biologics in severe asthma (Citation21). Nearly one-third of patients surveyed in the current study had discontinued biologic therapy at some point in their treatment history. The proportion of patients who had discontinued biologic therapy was similar to the 36.9% of patients with severe asthma who discontinued therapy with the biologic omalizumab over a 12-month period in a recent retrospective claims database analysis conducted in the US (Citation22). In this study, most of those discontinuing had been in receipt of omalizumab versus other biologics, however this is likely reflective of the relative level of use of each biologic in real-world practice at the time of analysis.
From the perspectives of the physicians included in the current study, a lack of symptom control, particularly shortness of breath, exacerbations and other chronic symptoms, were key reasons for discontinuing biologic therapy in patients with severe asthma. Symptom control was also a key reason for patients, and the three symptom categories described by physicians were among their top six reasons for biologic discontinuation. The cost of biologic treatment was also an important factor, cited as the 5th most common reason for discontinuation among physicians and the 3rd most common reason among patients. It is also possible that the proportion reporting costs as a reason for discontinuation may be an underestimation, as some patients may not wish to divulge this as a reason. Although discontinuation of biologics for safety reasons has been reported (Citation23), side effects were cited as a reason for discontinuation by only 15.3% of physicians and 7.8% of patients. The most common reasons for switching biologic broadly mirrored the reasons for discontinuation; however, there were notable exceptions in how often these reasons were cited by patients switching biologic including cost (2–3-fold lower with switch), patient request (4–5-fold lower), and the availability of a new drug. In summary, it appears that while discontinuation and switching share common reasons for either decision, owing to symptoms and exacerbations, they differ in that patient request and cost are more likely to be drivers of discontinuation compared with switching therapy.
There were several characteristics that occurred more commonly in patients who discontinued biologic therapy than in those who continued treatment. Firstly, there was a trend toward an increased discontinuation rate in males and younger patients versus females and older patients. There were fewer asthma-related comorbidities, higher use of SABA and LAMA controller monotherapies, and lower exacerbation rates in those who discontinued. These observations could result from various scenarios such as patients who discontinued had less severe disease, or if they were younger and male with fewer comorbidities, lower exacerbation rates on the biologic would indicate less severe disease, but higher rescue inhaler use would indicate active symptoms and disease instability. It could also represent a patient group with control of “severe” disease on the biologic, who discontinue their biologic at that point in the hope of sustaining disease control with agents such as SABA and LAMA. As described, biologic discontinuation tended to correlate with increased SABA, LAMA, and LTRA usage. If these patients were switching from one biologic to another, this increased use of controller therapy may serve as a therapeutic bridge until the new biologic becomes active. Taken together, these results indicate a need for a tailored approach to care in certain patients, such as more frequent visits, digital communications, and/or assistance with care from close family members if permitted.
Although adherence has been linked with treatment discontinuation in some patient populations (Citation24), this did not appear to be the case in the current study as almost 80% of patients who discontinued biologic therapy were reported to be very or completely adherent to their treatment. Patient request was also a frequent reason for discontinuing biologic therapy and may represent a favored choice that was convenient and nonspecific.
As expected, the most common patient- and physician-reported reasons for missing a biologic administration were family and work commitments. The introduction and approval of self-administered biologics could allow patients to continue therapy at home, possibly mitigating the risk for missing appointments, reduced adherence, and discontinuation. The dislike of injections cited as a reason by 16.8% of patients can be discussed with a view to alleviating the concern around this procedure. Finally, the finding that 7.5% of patients missed an appointment because their asthma control felt better, indicates the need for healthcare providers to emphasize to their patients in advance the expectation that if/when they feel better, they will need to continue their medicine to continue to maintain that control.
The data on the influence of comorbidities on the likelihood of biologic prescription, from the perspective of physicians, provide further insight into real-world prescribing patterns in the severe asthma population. The likelihood of prescribing a biologic is driven primarily by the presence of four major comorbidities; allergic rhinitis, atopic dermatitis, nasal polyps and chronic rhinosinusitis (nasal polyps are only rarely observed without chronic rhinosinusitis, so these populations overlap). Our results indicate that physicians may be more likely to prescribe for select comorbidities that are thought to be directly related to the condition that they are primarily responsible for treating. For example, allergists were found to be less likely than pulmonologists to prescribe biologics for asthma in the presence of comorbid cardiovascular disorders, malignancy, coagulopathy, and liver or kidney disease. This prescribing pattern may reflect the typical role of pulmonologists as critical care doctors, where they may be more likely to initiate biologics in select comorbidities such as cardiovascular disease. Alternatively, it may be due to the relatively limited numbers of this patient group with whom allergists have contact, or hesitancy on the part of allergists because of clinical experience or safety concerns with potential drug/biologic interactions (Citation25,Citation26). Allergists also manage injectable immunotherapy in a patient population in whom relative, or absolute, contraindications stem from select comorbidities such as cardiovascular disease (Citation27).
Overall, the findings of this study reinforce the need for a better understanding and definition of expectations of outcomes between patients with severe asthma treated with biologic therapy and their physicians. Clinicians need to regularly assess symptom control, particularly shortness of breath and exacerbations, persistence with background therapy, as well as patients’ insurance/coverage status, as outlined in the Global Initiative for Asthma guidelines (Citation4). Exacerbation control requires regular clinical assessment. The burden and risk associated with exacerbations can vary markedly; however, patients often have symptoms that may only require a small adjustment in therapy. Finally, demographic and clinical measures such as sex, age, comorbidities, and asthma medication use are also important considerations when predicting which patients may be most likely to discontinue biologic treatment for severe asthma, to allow a targeted approach to care.
There are some important study limitations to consider. Firstly, the patient population was made up of those who were willing to participate during their physician visit, therefore findings may not be generalizable to the wider severe asthma population, including patients who visit their physician less frequently. Moreover, identification of relevant patients was determined by physician judgment and formal patient selection verification procedures were not used, although physicians were asked to provide data for consecutive patients to avoid bias. Furthermore, physician diagnosis of asthma may not have been confirmed by spirometry. It is also unknown if any differences in characteristics existed between those who did and did not complete the patient self-completed form, and whether this may have influenced the patient-reported findings. Additionally, some of the survey questions, including those on adherence, were subjective in nature and responses may have been biased due to differing patient/physician perceptions. Finally, this was a cross-sectional survey with no specified baseline period that was not designed for testing hypotheses. While this is not necessarily a limitation, because the data provided satisfied the study objectives, an extended period of evaluation may be worthy of future study to determine, for example, the duration of discontinuation, the likelihood, causes, or characteristics of secondary discontinuation upon switch, or if the drivers for discontinuation of the initial biologic are mitigated or resolved upon switch to the next biologic. Nonetheless, the data provide helpful insights into the reasons for biologic discontinuation in patients with severe asthma in the US.
Conclusions
In this analysis of a US population with severe asthma, nearly one-third of patients had ever discontinued biologic therapy, most commonly due to patient request, lack of symptom control, cost, or exacerbations. These data highlight the complexity of care for this patient group and the need for ongoing, regular assessment of common challenges to biologic continuation and reasons for discontinuation, including both clinical and non-clinical factors. Such assessments may aid holistic and personalized management of the most challenging and refractory asthma patients.
Supplemental Material
Download PDF (809.1 KB)Supplementary_Material_Response_to_reviewers_final.docx
Download MS Word (143.2 KB)Acknowledgment
Editorial support (in the form of writing assistance, including development of the initial draft based on author direction, assembling tables and figures, collating authors’ comments, grammatical editing, and referencing) was provided by Nathan Ley, PhD, at Fishawack Indicia Ltd. part of Fishawack Health, and was funded by GSK.
Declaration of interest
JS, MB, NM, and BH are employees of GlaxoSmithKline and hold stocks/shares; MS, JS, and MH are full-time employees of Adelphi Real World, a research agency that received funding from GSK for this study.
Data availability statement
GSK makes available anonymized individual participant data and associated documents from interventional clinical studies that evaluate medicines, upon approval of proposals submitted to www.clinicalstudydatarequest.com. To access data for other types of GSK sponsored research, for study documents without patient-level data and for clinical studies not listed, please submit an enquiry via the website. The data that support the findings of this study are available from Adelphi Real World, where restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of Adelphi Real World.
Additional information
Funding
References
- Centers for Disease Control and Prevention (CDC). Summary health statistics: National health interview survey, 2018. 2018 [accessed 2020 Aug 4]. https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2018_SHS_Table_A-2.pdf.
- Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, Adcock IM, Bateman ED, Bel EH, Bleecker ER, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:https://doi.org/10.1183/09031936.00202013.
- Scichilone N, Barnes PJ, Battaglia S, Benfante A, Brown R, Canonica GW, Caramori G, Cazzola M, Centanni S, Cianferoni A, et al. The hidden burden of severe asthma: from patient perspective to new opportunities for clinicians. J Clin Med. 2020;9(8):2397. doi:https://doi.org/10.3390/jcm9082397.
- GINA. Global strategy for asthma management and prevention. 2020 [accessed 20 May 2020]. https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report_-final-_wms.pdf.
- FDA. Xolair (omalizumab) highlights of prescribing information. 2003 [accessed 10 June 2020]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/103976s5225lbl.pdf.
- FDA. Nucala (mepolizumab) highlights of prescribing information. 2015 [accessed 10 June 2020]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/125526s004lbl.pdf.
- FDA. Cinqair (reslizumab) highlights of prescribing information. 2016 [accessed 10 June 2020]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/761033lbl.pdf.
- FDA. Fasenra (benalizumab) highlights of prescribing information. 2017 [accessed 10 June 2020]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761070s000lbl.pdf.
- FDA. Dupixent (dupilumab) highlights of prescribing information. 2017 [accessed 10 June 2020]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761055s007lbl.pdf.
- Bleecker ER, Wechsler ME, FitzGerald JM, Menzies-Gow A, Wu Y, Hirsch I, Goldman M, Newbold P, Zangrilli JG. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. Eur Respir J. 2018;52(4):1800936. doi:https://doi.org/10.1183/13993003.00936-2018.
- Corren J, Castro M, Ford LB, Bernstein JA, Jayawardena S, Maroni J, Rowe P, Amin N, Pirozzi G, Graham NMH, et al. Dupilumab improves asthma outcomes irrespective of frequency of previous asthma exacerbation history. Ann Allergy Asthma Immunol. 2019;123(2):222–224.e1. doi:https://doi.org/10.1016/j.anai.2019.04.028.
- Pavord ID, Korn S, Howarth P, Bleecker ER, Buhl R, Keene ON, Ortega H, Chanez P. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet. 2012;380(9842):651–659. doi:https://doi.org/10.1016/S0140-6736(12)60988-X.
- Prazma C, Albers F, Mallett S, Llanos-Ackert J, Yancey S. Mepolizumab improves patient outcomes and reduces exacerbations in severe asthma patients with comorbid upper airways disease. J Allergy Clin Immunol. 2019;143(2):AB94. doi:https://doi.org/10.1016/j.jaci.2018.12.286.
- Casale TB, Chipps BE, Rosén K, Trzaskoma B, Haselkorn T, Omachi TA, Greenberg S, Hanania NA. Response to omalizumab using patient enrichment criteria from trials of novel biologics in asthma. Allergy. 2018;73(2):490–497. doi:https://doi.org/10.1111/all.13302.
- FitzGerald JM, Bleecker ER, Menzies-Gow A, Zangrilli JG, Hirsch I, Metcalfe P, Newbold P, Goldman M. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir Med. 2018;6(1):51–64. doi:https://doi.org/10.1016/S2213-2600(17)30344-2.
- Ortega HG, Yancey SW, Mayer B, Gunsoy NB, Keene ON, Bleecker ER, Brightling CE, Pavord ID. Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: a secondary analysis of the DREAM and MENSA studies. Lancet Respir Med. 2016;4(7):549–556. doi:https://doi.org/10.1016/S2213-2600(16)30031-5.
- Gelhorn HL, Balantac Z, Ambrose CS, Chung YN, Stone B. Patient and physician preferences for attributes of biologic medications for severe asthma. PPA. 2019;13:1253–1268. doi:https://doi.org/10.2147/PPA.S198953.
- Janson SL, Solari PG, Trzaskoma B, Chen H, Haselkorn T, Zazzali JL. Omalizumab adherence in an observational study of patients with moderate to severe allergic asthma. Ann Allergy Asthma Immunol. 2015;114(6):516–521. doi:https://doi.org/10.1016/j.anai.2015.04.010.
- Ortega H, Lemiere C, Llanos J-P, Forshag M, Price R, Albers F, Yancey S, Castro M. Outcomes following mepolizumab treatment discontinuation: real-world experience from an open-label trial. Allergy Asthma Clin Immunol. 2019;15:37. doi:https://doi.org/10.1186/s13223-019-0348-z.
- Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes - a means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. doi:https://doi.org/10.1185/03007990802457040.
- Bousquet J, Brusselle G, Buhl R, Busse WW, Cruz AA, Djukanovic R, Domingo C, Hanania NA, Humbert M, Menzies Gow A, et al. Care pathways for the selection of a biologic in severe asthma. Eur Respir J. 2017;50(6):1701782. doi:https://doi.org/10.1183/13993003.01782-2017.
- Li P, Kavati A, Puckett JT, Jahnke J, Busse P, Hanania NA, Ortiz B, Doshi JA. Omalizumab treatment patterns among patients with asthma in the US Medicare population. J Allergy Clin Immunol Pract. 2020;8(2):507–515.e10. doi:https://doi.org/10.1016/j.jaip.2019.07.011.
- Doroudchi A, Pathria M, Modena BD. Asthma biologics: comparing trial designs, patient cohorts and study results. Ann Allergy Asthma Immunol. 2020;124(1):44–56. doi:https://doi.org/10.1016/j.anai.2019.10.016.
- Caminati M, Senna G, Stefanizzi G, Bellamoli R, Longhi S, Chieco-Bianchi F, Guarnieri G, Tognella S, Olivieri M, Micheletto C, et al. Drop-out rate among patients treated with omalizumab for severe asthma: literature review and real-life experience. BMC Pulm Med. 2016;16(1):128. doi:https://doi.org/10.1186/s12890-016-0290-5.
- Pepper AN, Hanania NA, Humbert M, Casale TB. How to assess effectiveness of biologics for asthma and what steps to take when there is not benefit. J Allergy Clin Immunol Pract. 2021;9(3):1081–1088. doi:https://doi.org/10.1016/j.jaip.2020.10.048.
- Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010;105(4):259.
- Pitsios C, Tsoumani M, Bilò MB, Sturm GJ, Rodríguez Del Río P, Gawlik R, Ruëff F, Paraskevopoulos G, Valovirta E, Pfaar O, et al. Contraindications to immunotherapy: a global approach. Clin Transl Allergy. 2019;9(1):45–10. doi:https://doi.org/10.1186/s13601-019-0285-4.