
Abstract
Objective: The aim of the study was to achieve consensus among a group of ultrasound proficient general practitioners (GPs) from Denmark, Norway, Sweden and Finland on which ultrasound scanning modalities and ultrasound-guided procedures are essential to GPs in their daily work for the purpose of including them in a basic ultrasound curriculum.
Design: The Delphi methodology was used to obtain consensus.
Subjects: Sixty Scandinavian GPs with more than two years of point-of-care ultrasound (POCUS) experience were invited to join the Delphi expert panel.
Main outcome measures: In the first Delphi round each member of the panel was asked to produce a list of scanning modalities and procedures which they found relevant to include in a basic ultrasound curriculum. In Delphi round two, these suggestions were presented to the entire panel who assessed whether they found them essential in their daily work. Items not reaching consensus in round two, were presented to the panel in a third and final round. Items reaching more than 67% agreement were included.
Results: Forty-five GPs were included in the study and 41 GPs completed all rounds. Agreement was obtained on 30 scanning modalities and procedures primarily within the musculoskeletal (8), abdominal (5), obstetric (5) and soft tissue (3) diagnostic areas. Four ultrasound-guided procedures were also agreed upon.
Conclusion: A prioritized list of 30 scanning modalities and procedures was agreed upon by a group of ultrasound proficient GPs. This list could serve as a guideline when planning future POCUS educational activities for GPs.
Point-of-care ultrasound (POCUS) is increasingly being used by general practitioners (GPs), but little is known about which ultrasound applications are most used.
We performed a systematic needs assessment among a group of ultrasound proficient GPs using the Delphi methodology for the purpose of establishing a basic POCUS curriculum.
The process resulted in a prioritized list of 30 scanning modalities and ultrasound guided procedures.
Our study provides the basis for an evidence-based basic POCUS curriculum for GPs.
Key points
Introduction
In recent years the use of point-of-care ultrasound (POCUS) has gained ground in general practice in part facilitated by the development of compact, low-cost, high-quality ultrasound scanners [Citation1]. In addition to this, a new generation of general practitioners (GPs) are expected to incorporate POCUS in patient care after having acquired ultrasound competencies during their pre- and postgraduate training [Citation2,Citation3]. Hence, the use of POCUS in general practice is assumed to increase significantly in the coming years.
POCUS examinations are different from traditional comprehensive ultrasound examinations which cover an anatomical region, assess more than one organ and result in a full report of the examination. Instead, POCUS examinations are performed to achieve specific procedural aims (e.g. direct the needle to the correct location) or answer focused clinical questions (e.g. ‘does my patient have ascites?’) [Citation4,Citation5].
Ultrasonography is a user dependent image modality and competence is needed to ensure diagnostic accuracy [Citation6]. POCUS requires a combination of anatomical and clinical knowledge, technical skills and the ability to interpret ultrasound images [Citation7]. Failure to provide GPs with the necessary skills could lead to false positive findings, eliciting unnecessary patient anxiety and further redundant testing. Similarly, false negative findings could lead to potentially dangerous diagnoses being overlooked. Acquiring and sustaining competencies of various scanning modalities and procedures require training and continual exposure to relevant clinical conditions.
Many scanning modalities could be included in a basic POCUS curriculum for general practitioners [Citation8], and several ultrasound curricula have been suggested and incorporated into general practice residency training programs [Citation9–Citation13]. While many studies have demonstrated that GPs are able to perform various ultrasound scanning protocols [Citation14–Citation17], few studies have addressed which competencies are relevant in general practice. Further, none of the curricula published have been evidence-based or prioritized. Therefore, a systematic needs assessment to guide a POCUS curriculum specific to general practice is called for.
The aim of the study was to achieve consensus among a group of ultrasound proficient GPs from Denmark, Norway, Sweden, and Finland on which ultrasound scanning modalities and procedures are essential to GPs in their daily work for the purpose of including them in a basic ultrasound curriculum.
Methods
Study design
A Delphi methodology was used to conduct a systematic general needs assessment to explore which ultrasound scanning modalities and procedures are essential to GPs in their daily work in order to establish a basic ultrasound curriculum [Citation18,Citation19]. The Delphi technique entails setting up a panel of experts in an area of interest. Panelists are anonymous to each other thereby avoiding dominant individuals to interfere with and unduly influence the process. The process consists of multiple rounds. In the first round, a brainstorm is performed by each participant in order to establish a comprehensive pool of suggestions for the panel to evaluate. In consecutive rounds, participants rate the items in order to come to an agreement on which items should be included in the end result. Rounds are iterated until consensus has been reached on some or all of the items. Usually, three rounds suffice, but more rounds can be added if agreement has not been reached. We set the level of agreement to two-thirds majority (67%) which is widely accepted in the literature [Citation20].
Selection of Delphi panel members
The following inclusion criteria were used: participants had to be GPs, work in a permanent position in a general practice in Denmark, Sweden, Norway or Finland, have completed a basic ultrasonography course which included basic physics, ‘knobology’ and an introduction to more than two scanning modalities and have used POCUS on a daily basis for more than two years. Potential participants were excluded if they had conflicts of interest (e.g. financial) or had a colleague in the same clinic who was already participating in the study. Key members of national ultrasound societies (Danish Society for Ultrasound in General Practice (DAUS) and Association for Ultrasound in General Practice (FUA Norway) were identified and asked to provide names of potential participants. Since no formal ultrasound societies for general practitioners exist in Sweden and Finland, participants were recruited through informal interest groups and course providers. Back-ground information about the study was provided to the participants by means of a homepage where the complete protocol was published (www.gp-ultrasound.com). Invitations were sent by e-mail. If potential participants met the inclusion criteria, they were asked to provide informed consent. The participants were anonymous to each other.
The Delphi process
The data collection was conducted from September 2018 to January 2019.
Delphi round 1: brainstorm
After inclusion each panel member received an e-mail including instructions on how to complete the questionnaire. The participants were asked to provide information about themselves, practice characteristics, POCUS use and equipment availability.
The panel members were asked the following question: ‘which scanning modalities and/or procedures should be included in a basic ultrasound curriculum for general practitioners? i.e. which modalities/procedures should every GP with ultrasound equipment be able to perform?’. A list of all the replies were produced and content analysis was applied by the project group (TL, CAA and MBJ) in order to allow for identification of items that were either too non-specific, similar or could be grouped in the same category. First, replies were categorized according to overall scanning area, e.g. musculoskeletal, abdominal and gynecological. Secondly, according to organ, e.g. kidney, bladder and uterus, and lastly according to condition, e.g. gall stone, living intrauterine pregnancy or abdominal aortic aneurism. If scanning protocols were suggested, they were subdivided into their individual constituent parts in order to avoid misunderstandings due to participants having different perceptions of the content of the protocol, e.g. FATE: pericardial effusion, chamber dimensions, wall thickness or estimation of ejection fraction. In case of difficulties categorizing an item, the project group resolved the problem by group discussion until consensus was reached. Items suggested by only one participant were excluded.
Delphi round 2: rating of scanning modalities
Panelists received an e-mail with instructions on how to fill out the questionnaire and a link to the second round of the survey. For each item, they were presented with the following question: ‘this scanning modality/procedure is essential for my work as a general practitioner’ and had to rate the statement on a five-point Likert scale where five was ‘strongly agree’ and one was ‘strongly disagree’.
An item was included in the final list of scanning modalities and procedures if it reached agreement (Likert score ≥ 4) by more than two-thirds (≥67%) of the participants. If the item reached agreement by less than one-third (≤33%) of the participants, it was excluded. Remaining items would go on to a third round for re-evaluation.
Delphi round 3: re-prioritization and elimination
In round three panelists were asked to re-rate the remaining items in accordance with the question in round two. To facilitate the responses, panelists were provided with a list of their previous replies and the overall results of the replies from the panel. Items reaching more than two-thirds agreement (≥67%) were included in the final list. The rest were excluded.
Statistics
Participant characteristics were recorded as categorical and continuous variables and characterized by descriptive statistics accordingly. Medians, ranges, frequencies, percentages and cumulative percentages were calculated for each item in round two and three. Consensus level was set to 67%. Mean Likert score for each item was calculated together with the standard deviation in order to rank each item in order of importance. Pearson´s correlation coefficient was calculated in order to explore correlation between agreement levels in round two and three.
The questionnaires were sent out using SurveyMonkey® and statistical analysis of data was performed with the IBM® SPSS® software package, version 25.0 (SPSS, Chicago, IL).
Ethics
Ethical approval was granted in the form of an exemption letter from the Regional Ethical Committee of the Capital Region, Denmark (file-number: H-18017138). Participants granted informed consent by replying to the invitation.
Results
Forty-five (75%) of the 60 general practitioners invited were included in the survey (). Nine did not meet the inclusion criteria and six did not reply to the invitation. Of the 45 panelists who replied in round one, 41 participated in round two (91%) and all 41 participated in round three (100%). Characteristics of the panelists completing round three are summarized in .
Figure 1. Study flow. Items: scanning modalities and procedures. N:number of panelists in the study.
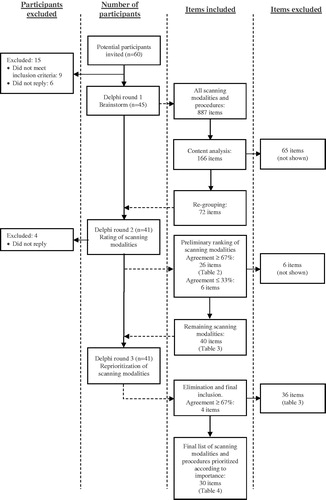
Table 1. Delphi panelist characteristics (n = 41).
The brainstorm process in round one resulted in 887 suggestions of scanning modalities and ultrasound-guided procedures in all. Content analysis including removal of duplicates reduced the number of items to 166. After elimination of items suggested by only one panelist and further re-grouping, the total number of items which were carried through to round two was 72 ().
In round two, 26 items were agreed upon by more than 67% of the panelist qualifying these items to be included in the final list without further re-evaluation (). Six items were excluded since less than 33% agreed to these. Forty items went on to round three (). In round three, four items: rotator cuff tendinitis and/or ruptures (partial/full), injection/aspiration knee joint, elbow joint effusion and trochanter bursitis, increased their level of agreement, and were added to the final list of items. A Pearson´s correlation coefficient of 0.78 between agreements in rounds two and three was obtained. shows all the items included in the final list prioritized according to their mean Likert score. The most common scanning modalities were within the musculoskeletal (8), abdominal (5), obstetric (5) and soft-tissue (3) diagnostic areas. Additionally, four ultrasound-guided procedures were included: shoulder and knee injection, Bakers cyst injection/aspiration and ultrasound guided abscess drainage.
Table 2. List of scanning modalities and procedures which reached agreement in round 2 (≥67%).
Table 3. List of scanning modalities and procedures in round 2, which were carried through to round 3 by level of agreement (percent).
Table 4. Final prioritized list of scanning modalities and procedures which have gained consensus by level of and importance (mean).
Discussion
Principal findings
We conducted a systematic needs assessment using the Delphi method among a group of 41 Scandinavian GPs who have used POCUS daily for more than two years. This process resulted in a list of 30 scanning modalities and procedures which a majority of panelists found essential to their work as GPs and could be considered for inclusion in a basic ultrasound curriculum. Simple scanning modalities and procedures within the musculoskeletal, obstetric, abdominal and soft tissue diagnostic areas were most prevalent.
Strengths and weaknesses of the study
The strength of our study is that we succeeded in establishing a homogenous panel of experienced GPs in enough numbers to obtain a valid result [Citation21]. A low drop-out rate between rounds was achieved indicating a dedicated and motivated panel. Panelists characteristics were representative of a diverse population of GPs and they provided many scanning modalities and procedures in round one, which secured a robust and representative selection of scanning modalities to be assessed in rounds two and three.
Our study has some limitations. GPs from each country were not represented in equal numbers. Panelists were mainly male and primarily worked in urban practices relatively close to radiological services (<50 km) thereby limiting the generalizability of our results. GPs in rural settings and in remote areas might find more advanced scanning modalities like lung and cardiac POCUS applications more useful than GPs working in an urban setting where easy access to emergency services and radiological departments is possible. Furthermore, primary care in the Scandinavian countries share many similarities regarding funding, access, visitation and referral to other specialties and the secondary sector [Citation22]. This may limit the relevance of our findings to countries where primary care does not play the same central role.
Even though consensus was reached on some items, there were also significant disagreements which is reflected in the wide intervals in range and standard deviation for many of the items. This divergence of opinions among panelists could be due to differences in gender, national guidelines, ultrasound experience, special interests, work requirements and geography. Our study was not designed to explore if significant differences between subgroups were present, however post-hoc statistical analysis indicated that Danish GPs were more restrictive regarding which scanning modalities and procedures to include in a basic curriculum (data not shown).
We acknowledge some methodological limitations regarding the way we designed the Delphi process which may have affected the validity of our findings. The condensation procedure excluded many items, which consequently did not have a chance to be rated and included in the final list. We eliminated items from round three which had gained consensus or were only agreed upon by less than a third in round two to secure a manageable number of items for the panelists to rate in round three. This contributed to a high response rate but did not allow for the panelists to rate the items in round three again.
Findings in relation to other studies
To our knowledge this is the first time an evidence-based systematic needs assessment of ultrasound scanning modalities for the purpose of establishing a basic POCUS curriculum for office-based GPs has been published. The American Academy of Family Practitioners (AAFP) has published a curriculum guideline for family medicine residents which proposes a wide range of POCUS applications, many of which are also included in our study [Citation9]. Applications are divided into basic and advanced according to consensus opinion. However, the guideline does not state how consensus has been reached and among whom. The authors suggest that successful implementation requires that course providers decide which modalities they find most useful in their setting. Our study is an attempt to provide an evidence-based basic POCUS curriculum for GPs in accordance with the AAFP guideline recommendation.
Most POCUS curricula for GPs published are based on assumptions about which modalities are useful for GPs, developed to be used in other settings than general practice, e.g. emergency departments or designed by general practitioners affiliated with academic centers [Citation10–13]. In addition to this, these ultrasound curricula bear considerable resemblance to curricula published for emergency physicians, which limit their relevance to the average GP [Citation23,Citation24].
The most common scanning modalities in our study were within the musculoskeletal, abdominal, obstetric and soft-tissue diagnostic areas. To some extent this is consistent with previously published studies about the use of POCUS in general practice. Thus, Andersen et al. [Citation8] found that abdominal and obstetric scanning modalities were most reported in the literature.
However, there are also substantial differences. Panelists in our study prioritized musculoskeletal scanning modalities which made out most of the scanning modalities. Given that musculoskeletal symptoms are among the most common presentations in general practice this is not surprising [Citation25]. However, only few studies have been conducted of both training in and use of musculoskeletal ultrasound in general practice [Citation8].
Cardiac and pulmonary scanning modalities, excluding pericardial and pleural effusion, did not gain consensus. These findings were surprising given that several studies suggest that limited cardiac examinations can be mastered by GPs and implemented in clinical practice [Citation16,Citation26,Citation27]. Nearly half of the panelists (49%) did not have phased array transducers and only 46% performed cardiac examinations which may explain their low priority in our study. The limited use of cardiac scanning modalities could be due to the fact that phased array (cardiac) transducers are more costly than curved array (abdominal) transducers. Furthermore, cardiac examinations are time consuming and require considerable training and routine to perform [Citation28,Citation29]. GPs might also omit cardiac examinations in clinical decision making due to the more severe consequences of making an erroneous diagnosis or overlooking significant pathology. A concern that seems well founded in the literature where cardiac examinations have lower diagnostic accuracies than other scanning modalities [Citation8].
Pulmonary scanning modalities did not reach agreement. This might reflect the fact that lung ultrasound is a new scanning modality and not widely utilized yet, even though it has been shown to be useful in general practice [Citation30].
The majority of panelists in our study performed 1–4 ultrasound scans a day which is in accordance with other studies [Citation8]. Legitimate concern could be raised about how to maintain adequate training if POCUS is applied to a wide range of indications. General practice is characterized by low disease prevalence rates and accordingly low predictive values of tests. Thus, scanning patients with high pre-test probabilities of having specific conditions is important to be aware of in order to obtain a correct result. In our study panelists agreed on simple scanning modalities of common clinical conditions, e.g. knee joint effusion and gall stones, which indicate that they recognize this concern.
One might argue that 30 items are a lot to cover in a basic curriculum. However, if a more limited curriculum is wanted the final prioritized list can still aid the course provider in deciding which items are most relevant to include.
Meaning of the study
Our study offers a proposal for the content of a basic ultrasound curriculum for GPs. The Delphi panel primarily agreed upon simple scanning modalities and procedures mainly within the musculoskeletal, abdominal, obstetric and soft tissue diagnostic areas. Cardiac, pulmonary and more advanced gynecological scanning modalities did not gain consensus and should probably not be included in a basic POCUS curriculum but reserved for more experienced GPs. Our data also shows a considerable range of opinions which need to be considered when establishing a curriculum. Future studies should focus on development of evidence-based educational activities for GPs and residents in primary care medicine.
Acknowledgements
The authors thank Doctor Canh le Nygaard for his help in recruiting GPs, the Danish Society of Ultrasound in General Practice (DAUS) and the Association for Ultrasound in General Practice (FUA Norway).
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Mengel-Jorgensen T, Jensen MB. Variation in the use of point-of-care ultrasound in general practice in various European countries. Results of a survey among experts. Eur J Gen Pract. 2016;22:274–277.
- Hall JW, Holman H, Bornemann P, et al. Point of care ultrasound in family medicine residency programs: a CERA study. Fam Med. 2015;47:706–711.
- Galusko V, Khanji MY, Bodger O, et al. Hand-held ultrasound scanners in medical education: a systematic review. J Cardiovasc Ultrasound. 2017;25:75–83.
- Dietrich CF, Goudie A, Chiorean L, et al. Point of care ultrasound: a WFUMB position paper. Ultrasound Med Biol. 2017;43:49–58.
- Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med. 2011;364:749–757.
- Todsen T, Melchiors J, Charabi B, et al. Competency-based assessment in surgeon-performed head and neck ultrasonography: a validity study. Laryngoscope. 2018;128:1346–1352.
- Tolsgaard MG, Todsen T, Sorensen JL, et al. International multispecialty consensus on how to evaluate ultrasound competence: a Delphi consensus survey. PLoS One. 2013;8:e57687.
- Andersen CA, Holden S, Vela J, et al. Point-of-care ultrasound in general practice: a systematic review. Ann Fam Med. 2019;17:61–69.
- American Academy of Family Physicians. Recommended curriculum guidelines for family medicine residents: point of care ultrasound. AAFP Reprint No 290D. 2016 Dec [cited 2018 Mar 1]. Available from: https://www.aafp.org/dam/AAFP/documents/medical_education_residency/program_directors/Reprint290D_POCUS.pdf
- Bornemann P. Assessment of a novel point-of-care ultrasound curriculum's effect on competency measures in family medicine graduate medical education. J Ultrasound Med. 2017;36:1205–1211.
- Lee JB, Tse C, Keown T, et al. Evaluation of a point of care ultrasound curriculum for Indonesian physicians taught by first-year medical students. World J Emerg Med. 2017;8:281–286.
- Wong F, Franco Z, Phelan MB, et al. Development of a pilot family medicine hand-carried ultrasound course. WMJ. 2013;112:257–261.
- Flick D. Bedside ultrasound education in primary care. J Ultrasound Med. 2016;35:1369–1371.
- Todsen T, Tolsgaard MG, Olsen BH, et al. Reliable and valid assessment of point-of-care ultrasonography. Ann Surg. 2015;261:309–315.
- Lindgaard K, Riisgaard L. Validation of ultrasound examinations performed by general practitioners. Scand J Prim Health Care. 2017;35:256–261.
- Mjolstad OC, Snare SR, Folkvord L, et al. Assessment of left ventricular function by GPs using pocket-sized ultrasound. Fam Pract. 2012;29:534–540.
- Mumoli N, Vitale J, Giorgi-Pierfranceschi M, et al. General practitioner-performed compression ultrasonography for diagnosis of deep vein thrombosis of the leg: a multicenter, prospective cohort study. Ann Fam Med. 2017;15:535–539.
- Keeney S, Hasson F, McKenna H. The Delphi technique in nursing and health research. 1st ed. Oxford: Wiley-Blackwell; 2011.
- Nayahangan LJ, Stefanidis D, Kern DE, et al. How to identify and prioritize procedures suitable for simulation-based training: experiences from general needs assessments using a modified Delphi method and a needs assessment formula. Med Teach. 2018;40:676–683.
- de Villiers MR, de Villiers PJ, Kent AP. The Delphi technique in health sciences education research. Med Teach. 2005;27:639–643.
- Skulmoski GJ, Hartmann FT, Krahn J. The Delphi method in graduate research. Int J Inf Educ Technol. 2007;6:1–21.
- Lyttkens CH, Christiansen T, Häkkinen U, et al. The core of the Nordic health care system is not empty. Nordic J Health Eco. 2016;4:7.
- Ultrasound guidelines: emergency, point-of-care and clinical ultrasound guidelines in medicine. Ann Emerg Med. 2017;69:e27–e54.
- European Core Curriculum for Emergency Medicine. 2017 [cited 2019 Mar 1]. Available from: https://eusem.org/images/ebeem/European-Core-Curriculum-for-EM-Version-1.2-April-2017-final-version-1.pdf
- Moth G, Olesen F, Vedsted P. Reasons for encounter and disease patterns in Danish primary care: changes over 16 years. Scand J Prim Health Care. 2012;30:70–75.
- Zamorano JL, Moreno R, Alburquerque C. Echocardiography performed by physicians outside of echo-labs – is it possible? Eur Heart J. 2002;23:908–909.
- Evangelista A, Galuppo V, Mendez J, et al. Hand-held cardiac ultrasound screening performed by family doctors with remote expert support interpretation. Heart. 2016;102:376–382.
- Chamsi-Pasha MA, Sengupta PP, Zoghbi WA. Handheld echocardiography: current state and future perspectives. Circulation. 2017;136:2178–2188.
- Bornemann P, Johnson J, Tiglao S, et al. Assessment of primary care physicians' use of a pocket ultrasound device to measure left ventricular mass in patients with hypertension. J Am Board Fam Med. 2015;28:706–712.
- Chavez MA, Naithani N, Gilman RH, et al. Agreement between the World Health Organization algorithm and lung consolidation identified using point-of-care ultrasound for the diagnosis of childhood pneumonia by general practitioners. Lung. 2015;193:531–538.