Spontaneous regression of metastatic renal cell carcinoma (MRCC) is a rare event. Since it was first described in 1928 about 95 cases have been reported Citation[1], including post-nephrectomy regression. Histological documentation of metastatic lesions has been present in only 20–25% of these cases Citation[1–3], and the duration of the regression is often short or not reported. A number of possible mechanisms for the spontaneous regression of cancer have been proposed. In 1966 Everson and Cole postulated that immune mechanisms were the most important factors Citation[4]. This is also the general view today. A correlation between immunosuppression and the incidence of cancer is generally accepted Citation[5]. During the last three decades stimulation of the immune system with Interferon-α and/or Interleukin-2 has thus been a principle in the therapy of MRCC, avoiding glucocorticoids during such treatment Citation[6], Citation[7], as these drugs often lead to suppression of the immune system.
We have observed a long lasting and ongoing complete remission of histologically verified MRCC in a patient who received Prednisone monotherapy.
In April 1995 a 61-year old woman underwent right-sided nephrectomy, due to a non-metastatic renal cell carcinoma of the clear cell type, Fuhrman grade 3 with penetration of the renal capsule into the perirenal fat tissue.
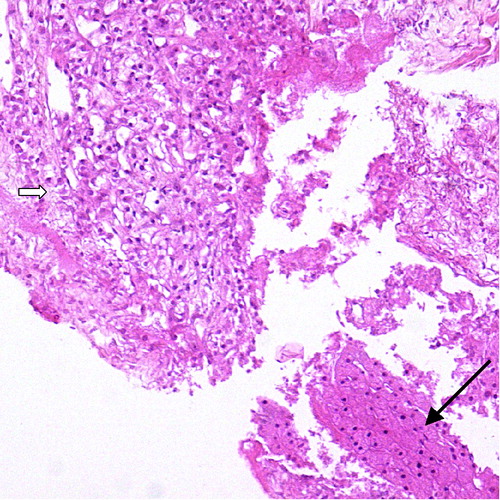
In November 1995 a computerized tomography (CT) revealed right-sided paravertebral lymphatic metastases and a 5 cm large lesion in lobus caudatus hepatis. CT-guided fine needle biopsy of the hepatic lesion showed the metastasis from renal clear cell carcinoma ().
Figure 1. Fine needle biopsy from the liver with clear cell carcinoma (Hematoxilin and eosin×20). Liver parenchyma is marked with long arrow, tumour tissue with short, broad arrow.
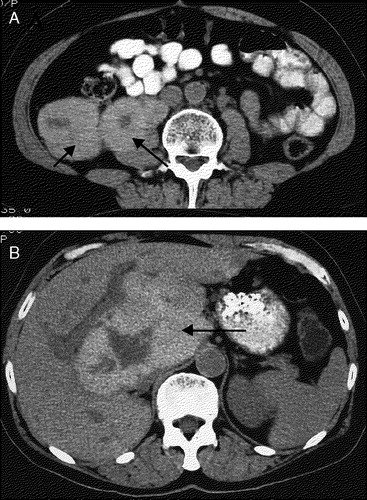
Surgery was deemed impossible, and the patient was in March 1996 referred for systemic treatment. At this time her erythrocyte sedimentation rate (ESR) was 87 mm. A CT showed three retroperitoneal partly necrotic tumour masses with infiltration in M. psoas major, reaching from the liver to the right iliac crest. The hepatic lesion had progressed to a size of 13×8 cm (A, B). Due to her poor general condition (performance status 3), immunotherapy was not initiated. She received prednisone 10 mg twice daily as her only palliative treatment. During the subsequent months the ESR fell to 30 mm. The patient reported a significant clinical improvement. A CT in November revealed reduction of the hepatic lesion to 5 cm in diameter, and almost complete regression of the paravertebral masses.
Figure 2. Metastatic sites (March 1996). a: Retroperitoneal tumour masses (arrows), b: Metastasis to lobus caudatus hepatis (13×8 cm).
During an explorative laparatomy in February 1997 inoperable tumour masses were palpated in lobus caudatus hepatis and multiple enlarged lymph nodes in the coeliac region, omentum minus and the right colon flexure. Biopsies from the tumour nodules in omentum minus and the colon flexure showed no sign of malignancy but inflammatory reaction with histiocytic cells. This was confirmed by immunohistochemistry, which was strongly positive for histiocytic marcers and negative for pancytokeratins.
A new CT in June 1998 demonstrated further decrease of the tumour masses, with complete remission in 2000. Prednisone was discontinued in June 2000. The patient has remained without evidence of MRCC with last control in March 2005.
We regard this case as representing spontaneous regression of MRCC where the role of corticosteroid therapy remains undefined.
An unsolved issue is whether a single or multiple mechanisms are essential for spontaneous regression of MRCC. Immune mechanisms are most often evoked as the mechanism of regression Citation[2]. Interferon-α and Interleukin-2 have been shown to exert antitumour effects in a subset of patients with MRCC Citation[2], Citation[8]. Interleukin-2 is presumed to activate T-lymphocytes, natural killer (NK) cells, lymphocyte-activated killer cells and tumour infiltrating lymphocyte cells as a mechanism of action. Interferons are capable of multiple immunmodulatory effects involving monocytes, macrophages and B-cells, as well as induction of Interleukin-2 receptors Citation[2].
The present observation of complete regression of MRCC in a patient receiving palliative doses of prednisone as monotherapy is intriguing because glucocorticoids are known to suppress a number of key mechanisms in immune reactions. Thus glucocorticoids decrease the generation of Interleukin-2 and other cytokines. After binding to an intracellular corticoid receptor this complex can inhibit the effect of the proinflammatory transcription factor NF-κB that again stimulates the transcription of Interleukin-2, Interleukin-2 receptors and a number of other proinflammatory proteins. Subsequently this leads to a suppression of T-lymphocyte function, NK cells, B-lymphocytes and immunoglobulin formation.
The seemingly contradictory finding of regression of MRCC in a patient receiving prednisone as monotherapy, does not exclude the possibility that the tumour regression was caused by immune mechanisms. Possibly the relatively low prednisone doses in our patient were insufficient to suppress a strong immunological attack against the renal carcinoma cells. The necrotic areas in our patient's metastases before any therapy may indicate some degree of treatment-independent initiation of tumour regression. In this connection it is interesting that patients with MRCC respond to treatment with interferon-α even though the drug is combined with prednisone Citation[8]. The role of glucocorticoids is therefore undefined in MRCC.
Alternatively other types of mechanisms such as angiogenesis inhibition and apoptosis have been discussed in relation to tumour regression of MRCC. These pathways’ contribution has not been investigated in our patient.
Our case confirms the clinical experience of a sometimes unpredictable clinical course in MRCC, with spontaneous and unexplained complete remission.
References
- Thoroddsen A, Gudbjartson T, Geirsson G, Asnarsson BA, Magnusson K, et al. Spontaneous regression of pleural metastases after nephrectomy for renal cell carcinoma. Scand J Urol Nephrol 2002; 36: 396–8
- Papac RJ. Spontaneous regression of cancer. Cancer Treat Rev 1996; 22: 395–423
- Abubakr YA, Chou TH, Redeman RG. Spontaneous remission of renal cell carcinoma: A case report and immunological correlates. J Urol 1994; 152: 156–7
- Everson TC, Cole WH. Spontaneous regression of cancer. W. B. Saunders Co, Philadelphia 1966; 11–87
- Papac RJ. Spontaneous regression of cancer: Possible mechanisms. In Vivo 1998; 12: 571–8
- Glapsy JA. Therapeutic options in the management of renal cell carcinoma. Semin Oncol 2002; 29(Suppl 7)41–6
- Bukowski RM. Immunotherapy in renal cell carcinoma. Oncology 1999; 13: 801–10
- Fosså SD, Lehne G, Gunderson R, Hjelmaas U, Holdener EE, et al. Recombinant interferon alpha-2a combined with prednisone in metastatic renal-cell carcinoma: Treatment results, serum interferon levels and the development of antibodies. Int J Cancer 1992; 50: 868–70