Case Report
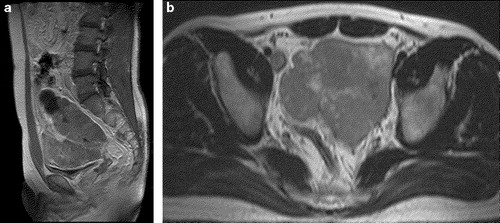
A 32-year-old man was admitted to our department due to dysuria that was associated with an intra-adominal mass. Ultrasonography revealed a normal bladder, a lobulated mixed echoic mass in the retroperitoneum and small quantity of pelvic ascites. Preoperative magnetic resonance imaging (MRI) revealed that the largest tumor was slightly hypointense relative to the muscle on the T1-weighted image, hyperintense relative to the muscle on the T2-weighted image, and heterogeneously enhanced with some cystic components ().
Figure 1. A. Sagittal scan of the contrast enhanced T1WI shows a large lobulated and moderately enhancing mass in the pelvic cavity. A cystic portion can be seen in the upper part of the mass. Note the compressed urinary bladder inferior to the mass. B. Axial scan of T2WI shows a large lobulated hyperintense mass in the pelvic cavity. The portions with bright signal intensity are seen inside of the mass, representing cystic components. Note the sigmoid colon posterior to the mass.
The patient underwent a complete gross excision of the mass combined with a low anterior resection. At surgery, the tumor was found adhered to the wall of the rectum and could not be dissected without causing injury. There were several retroperitoneal nodules that proved to be a metastasis, which was confirmed by a frozen histological evaluation.
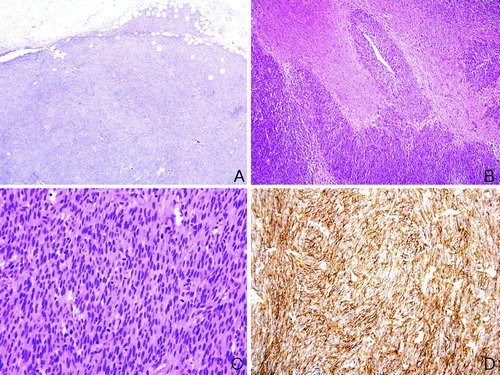
Grossly, the tumor measured 13.3 (CC)×10.2 (AP)×9.4 (W) cm. It was encapsulated, and cut sections showed fleshy, reddish and some myxoid tissue. Histologically, the tumor cells consisted of spindle cells and relatively uniform medium size round epitheloid cells. There was marked nuclear pleomorphism and high mitotic activity (60/10 High power field). The tumor cells tested strongly immunohistochemically positive for c-kit (CD 117), CD34, and vimentin, but negative for desmin, α-smooth muscle actin, and the S-100 protein ().
Figure 2. Histology of EGIST. A. Low power view shows that the tumor cells are composed of spindle cells and invade the surrounding tissue (hematoxylin and eosin×40). B. Extensive tumoral necrosis is noted (hematoxylin and eosin×100). C. High power view demonstrates frequent mitoses (60/10 High power field, hematoxylin and eosin×200). D. Immunohistochemically, the tumor cells test strongly positive for c-kit (×200).
After an uneventful postoperative course, the patient was discharged 14 days after surgery and has since been treated with imatinib mesylate (Gleevec®, Novartis Pharma, Basel, Switzerland). There was no recurrence of the tumor at the 6-months follow-up examination.
Discussion
Gastrointestinal stromal tumors (GISTs) are nonepithelial neoplasms that usually arise in the muscular layer of the digestive tract, particularly in the stomach and small intestine. These lesions exhibit the typical histopathological and immunophenotypic features, including prominent tumor cell spindling and c-kit (CD117) expression Citation[1]. GISTs rarely develop outside of the digestive tract especially in the soft tissues of the abdomen and retroperitoneum. Such tumors are designated extra-GISTs (EGISTs). EGISTs are histologically and immunohistochemically similar to their gastrointestinal counterpart but they have an aggressive course resembling small intestinal stromal tumors and they have no or little connection to the abdominal wall or serosal surface of the gastrointestinal tract Citation[2]. As a result of their rarity, the clinicopathological features of the EGISTs, particularly those of the retroperitoneum, have not been fully elucidated.
Although the histogenesis of EGISTs has not been determined, the expression of the c-kit receptor in EGISTs suggests either the presence of pacemaker cells outside the gastrointestinal tract or the ability of the mesenchymal elements to recapitulate this phenotype aberrantly.
Regarding the significance of the prognostic factors, although the tumor size and mitotic index have been well established for GISTs, Emory et al. Citation[3] reported that the behavior of stromal tumors differs according to the location, and there appears to be a general trend for an increasingly aggressive behavior as one proceeds distally along the gastrointestinal tract. EGISTs have more in common with the GISTs located in the distal gastrointestinal tract, which means that they are considered to be an aggressive group of stromal tumors.
In contrast to studies of GISTs, those of EGISTs did not report any association between the tumor size and outcome. It is believed that this can be best explained by the fact that the majority of EGISTs are large when first detected. This is because small EGISTs are rarely encountered as they hardly ever produce symptoms that lead to detection. Therefore, as Ortiz-Rey at al. reported Citation[4], when first detected, many cases of EGISTs can be accessible by a fine needle aspiration biopsy (FNAB).
Until the recent introduction of imatinib mesylate, which is the inhibitor of the tyrosine kinase activity of c-kit, a complete surgical resection is the best treatment for GISTs. The drug has been reported to be an effective and safe for controlling metastatic GIST disease. However, the role of imatinib in the treatment of EGISTs is unclear.
In summary, CD117-positive stromal tumors, although rare and found mainly in the gastrointestinal tract, can involve the retroperitoneum. This should be considered when imaging studies reveal a huge abdominal tumor involving the retroperitoneum without a connection to the gastrointestinal tract. The management of these tumors demands the surgical removal because these tumors are resistant to chemotherapy. Further studies will be needed to more clearly define the phenotypic and genetic characteristics as well as the biological behavior of these rare tumors.
References
- Fletcher CD, Berman JJ, Corless C, Gorstein F. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol 2002; 33: 459–65
- Reith JD, Goldblum JR, Lyles RH, Weiss SW. Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol 2000; 13: 577–85
- Emory TS, Sobin LH, Lukes L, Lee DH, O'Leary TJ. Prognosis of gastrointestinal smooth-muscle (stromal) tumors: dependence on anatomic site. Am J Surg Pathol 1999; 23: 82–7
- Ortiz-Rey JA, Fernandez GC, Magdalena CJ, Alvarez C, Anton I, Miguel PS, et al. Fine needle aspiration appearance of extragastrointestinal stromal tumor. Acta Cytologica 2003; 47: 490–4