Abstract
A non-blinded three armed study of the effect of Aloe vera, Essex and no lotion on erythema was performed. The erythema is an effect of radiotherapy treatment in breast cancer patients. The study required testing of objective methods for measuring the erythema. The chosen experimental methods were Near Infrared Spectroscopy, Laser Doppler Imaging and Digital Colour Photography. The experimental setup was made in such a way that in parallel with testing the effect of the lotions there was also a test of the sensitivity of the instruments. Fifty women were selected consecutively to participate in the study. They were all subjected to treatment with high-energy electrons (9-20 MeV) after mastectomy, 2Gy/day to a total dose of 50 Gy. Measurements were performed before the start of radiotherapy and thereafter once a week during the course of treatment. Aloe vera and Essex lotion were applied twice every radiation day in selected sites. The increase in skin redness could be monitored with all techniques with a detection limit of 8 Gy for Digital Colour Photography and Near Infrared Spectroscopy and 18 Gy for Laser Doppler Imaging. In clinical practice our recommendation is to use Digital Colour Photography. No significant median differences were observed between the pairs no lotion-Essex, no lotion-Aloe vera and Essex-Aloe vera for any of the techniques tested.
Breast cancer is the most common cancer form among women in Sweden with more than 6 800 new cases discovered in 2003 (www.cancerfonden.se). In the developed countries more than 50% of all cancer patients will be treated with radiotherapy Citation[1]. The wanted effects of the treatment are failure of mitosis, cell death, apoptosis and damage to the target cells although normal tissue is affected as well Citation[1], Citation[2] There are, however, some negative consequences that are divided into acute and late effects Citation[1]. Thus, up to 95% of the patients treated with external radiotherapy will experience some form of skin reaction due to the radiosensitivity of the skin Citation[3], Citation[4]. The exact mechanism for erythema induced by ionizing radiation is not known, but an intrinsic cellular radiosensitivity is suggested Citation[4].
The extent of erythema is often assessed with visual inspection, which implies that there is a risk that subjective factors interfere with the evaluation. Furthermore, the absence of a universal skin reaction rating scale makes it difficult to compare results from different studies Citation[5]. Thus, two different grading systems were used in a trial investigation on the toxicity of Aloe vera gel in the management of radiotherapy induced skin reactions. The methods were ARSI scale (Acute Skin Reaction Index) and RTOG (Radiation Therapy Oncology Group) and the comparison gave different results Citation[6].
Some general recommendations for skin care are prevalent i.e. it is advised not the rub the skin and to keep it clean and dry. These have some value but there is no established consensus on how to treat skin reactions and therefore treatment policies vary between centres Citation[7].
The high incidence of skin reactions among patients undergoing radiotherapy has led to an interest in investigating methods to minimise and treat side effects. In some earlier randomised trials concerning non-steroid creams Citation[8–12] only sucralfate and hyaluronic acid have shown statistically positive effects Citation[10], Citation[13]. Boström et al. recommend the use of a potent topical steroid together with an emollient cream Citation[14], which showed a significantly more effective result than just the emollient cream.
Essex lotion is a commonly recommended and used product at radiotherapy departments in Sweden. However, to our knowledge there are no investigations on its capability to reduce radiotherapy induced erythema. The effect of using Aloe vera based products in the treatment of erythema has been investigated with somewhat contradicting results Citation[15]. A randomized, controlled and double blind trial involving 194 women undergoing radiotherapy for breast cancer was performed by Williams et al., no significant reduction in erythema was observed with Aloe vera gel as compared to a placebo Citation[16]. Similar results were obtained when Aloe vera was compared with Aqueous cream in a phase III study involving 225 breast cancer patients who were treated with tangential fields after partial resection Citation[17].
In another randomized, controlled study involving 70 patients, Olsen et al. Citation[18] compared Aloe vera gel and mild soap versus using mild soap alone in preventing radiotherapy induced erythema. It was concluded that the application of Aloe vera gel on the irradiated skin provides a protective effect at cumulative dose larger than 27 Gy. Another study concludes that hydrophilic substances such as Aloe vera gel or vegetable oils that are high in essential fatty acids are as effective as mild steroid creams such as 1% hydrocortisone in reducing severe reactions Citation[15].
Three different objective measurements Near Infrared spectroscopy, Laser Doppler Imaging and Digital Colour Photography are suggested in this paper for objective classification of erythema. The technical details of these methods including statistical analysis of the data are described elsewhere Citation[19]. In the present paper the potential of the objective methods to measure increase in erythema compared to non-irradiated skin is investigated. Once the first goal is reached, the methods can also be used to try to differentiate between the lotion treatments. In clinical practise patients are often recommended to use Essex lotion to reduce skin reactions during radiotherapy. This treatment can be expensive for the patients and therefore more knowledge is needed for a well-founded recommendation.
Thus the main goal of the present paper is to use the objective methods in determining whether Essex lotion or Aloe vera could reduce the intensity of the erythema in acute radiation dermatitis and to find a scientific recommendation for the patient.
Material and methods
Clinical background
Fifty female patients with breast cancer who had undergone total mastectomy were included in the study by consecutive selection. A previous pilot study on 25 patients showed promising results, but also a large variation in the data. Therefore it was decided to double the number of patients. This was also reasonable considering time and expenses involved.
The average age was 60 years. The patients were subjected to treatment involving 2Gy/day to a total dose of 50Gy, with high energy electrons 9-20 MeV, [20 MeV (n = 1), 15 MeV (n = 4), 12 MeV (n = 21), 10 MeV (n = 21), 9 MeV (n = 3)]. To make sure that the exact dose was delivered to the patients the equipment was controlled by a radiophysicist every day. No investigation was made on whether the different energies applied had any effect on the development of erythema. Bolus was used for all patients to reach maximum dose in the skin and this should minimize any influence the effect different energy would have on the development of erythema. Forty of the women in the study had received chemotherapy before starting their radiotherapy treatment. To obtain a uniform dose distribution a radiophysicist selected, three sites (2×4 cm2) in the treated area. Site two was not treated with skin lotion while the other two sites were treated twice every radiation day with Aloe vera gel and Essex lotion (0.2 ml) respectively (). The patients included in the study were informed not to use any topical treatment themselves in the treated area. The lotions were applied directly after the radiotherapy treatment and once again 4 hours later by a nurse. Previous studies (23) have shown a large individual variation between patients and therefore this study uses each patient as their own reference. In order to apply the lotions in a reproducible manner. After 25 patients the lotion-treated sites were inter-changed. All four sites, see , were measured with Near Infrared Spectroscopy, Digital Camera and Laser Doppler Imaging before radiation treatment started and thereafter once a week during the course of treatment. This study was performed to objectively study the extent of erythema developed and to see if the lotions would effect the development of erythema. Subjective classification is a rough estimation and the small treatment areas used in this study (2×4 cm) would make it problematic to give an accurate subjective estimation.
Figure 1. Illustration of measurement sites. 1 and 3 = Essex or Aloe vera, 2 = no lotion, 4 = healthy breast. Regions 1, 2, 3 can be placed vertical or horizontal.
All women participating in the study signed a written consent and the study was approved by the Ethical Committee (archive number 02-168) and the “Medical Products Agency” (archive number 2002/23568) and was monitored by Northern Sweden Clinical Research Institute NS-CRI
Skin lotions
The lotions in the present study were Aloe barbadensis 97% Gel (Neli AB, Halmstad, Sweden) and Essex lotion (Schering – Plough, Germany), see Appendix 1. A volume of 0.2 ml was applied twice every treatment day. Essex lotion was chosen as this is the most frequently recommended lotion at the local university hospital as in many other treatment centres in Sweden. Aloe vera on the other hand is a lotion often chosen by the patients themselves as it is believed to have positive healing effect on skin burns.
Aloe barbadensis is a member of the liliaceae family Citation[20]. The chemical composition of the Aloe plant depends on climate, species and growing conditions. The gel of the leaf is the most frequent Aloe product used by the cosmetic industry and is added to many sun and skin care products. The variety of organic materials in the gel is thought to have emollient, moisturising and healing effects Citation[21]. The use of Aloe vera in the treatment of skin reactions caused by radiotherapy dates back to 1935 Citation[22]. Aloe vera has an ability to penetrate deeply into the skin, to block UVB sunrays from affecting the skin, to rebalance the skin pH, and is thought to have antibiotic, anti-coagulant and anti-viral properties Citation[15].
Essex lotion is a commonly used lotion that is not registered as a medical product and therefore there are no specific recommendations for its use. The manufacturer claims that it keeps the skin moist and that it has a protective effect (http//:aponet.apoteket.se).
Near Infrared Spectroscopy
Near Infrared Spectroscopy has previously been used for skin studies Citation[23]. The instrument used in this study was a Bruker FT-NIR (Matrix F) with a fibre-optic probe (833–2 500 nm). Three consecutive spectra were collected in a scar-free area in the centre of each of the four measurement sites. The fibre-optic probe illuminates the skin with near infrared radiation in a spot of approx. 3 mm diameter. The reflected radiation that is not absorbed by the skin is used to construct a spectrum. The method is fast and easy to use. Wavelengths above 1 200 nm are not affected by pigmentation.
Digital Colour Photography
As an alternative to visual subjective inspection, it was decided to use Digital Colour Photography which is quick, cheap and easy to use. The results are files with measurable grey levels over the photographed skin part. The use of an electronic flash made it possible to have reproducible illumination. For an objective examination, the data from the digital camera can easily be extracted and thereafter subjected to image and/or data analysis. A Fuji FinePix S2, equipped with a Micro-Nikon f 1:2, 8 60 mm objective and a Nikon macro speedlight SB-29 (ring flash) were used to photograph the skin. A white plastic ruler was included in the 3040×2016 pixel images and used as a white balance and geometry reference standard. A skin area, free from scars, and a part of the ruler were selected from each image to produce average Red Green Blue (RGB) values. Pigmentation will affect the colour of the skin and could therefore be confused with classification of erythema.
Laser Doppler
Laser Doppler Imaging uses laser beam scanning to illuminate a chosen area of skin with monochromatic laser radiation. The measurement head uses the wavelength shifts in the radiation to calculate movement of blood cells by the Doppler effect. Thus it can be used to measure perfusion, i.e. the amount and velocity of the red blood cells in the skin. The perfusion is assumed to increase as the erythema develops. Three measurements were made in all sites, see , with a Laser Doppler Imaging (PIM II, Perimed, Sweden), and the signal is processed to a scale linearly related to tissue perfusion. The Laser Doppler images were not reproducible and therefore an average perfusion was calculated. It is not expected that pigmentation will affect the Laser Doppler results in the same way as perfusion.
Results
The extent of erythema developed differed between patients. Some patients developed more severe erythema however no one had to stop their radiation treatment because of severe skin reactions.
Near Infrared Spectroscopy
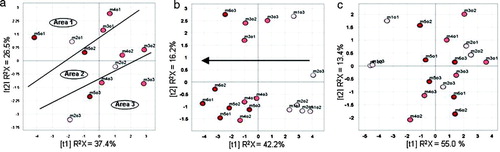
The NIR spectra have many correlated wavelengths and are too large for visual inspection or inclusion as appendices. Therefore a meaningful data reduction was needed. Principal component analysis (PCA) reduces the 5 704 measured wavelengths to a few components that explain most of the interesting variation in the data and makes studying the spectral information much easier. The spectra from site 1–3, i.e. all patients and all radiation doses were averaged over replicates, mean-centred and the data matrix was analysed with Principal Component Analysis, PCA Citation[24]. The resulting score plot showed clustering tendencies for the reference measurements and the measurements made at the end of the radiation treatment Citation[19] but the large individual differences call for local, patient-based models. In , score plots of local PCA models for three patients are shown. For the patient shown in a the three measurement sites separate very well with no strong tendencies for radiation dose. In b the radiation dose shows a clear trend (arrow) but the role of measurement sites is rather blurred. For the patient shown in c no trends could be seen. It is impossible to show all individual patient models, but generally all patients adhered to one of the three scenarios portrayed in . A PCA on all the measurements was used to extract first and second score vectors. These were used for the calculation of the Wilcoxon Signed Rank Sum Test Citation[25] (www.fon.hum.uva.nl/Service/Statistics/Signed_Rank_Test.html), which showed that even measurements made after a small radiation dose differed significantly from those at zero dose value. This makes the median detection limit for Near Infrared Spectroscopy 8 Gy. No significant differences for the lotions and using no lotion were found by Near Infrared Spectroscopy.
Figure 2. Principal Component Analysis (PCA on NIR data) score plots for three patients (a-c). The plots illustrate how individuals respond differently to the radiotherapy treatment and how the sites that are supposed to be similar might still be different.
Digital Colour Photography
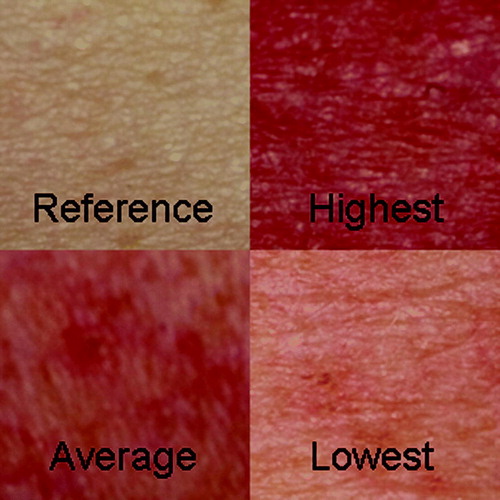
There are large individual differences in the sensitivity of the skin to radiotherapy. The photographs in clearly show that the irradiated skin is redder than the reference. The images taken at maximum dose irradiated for the lowest, highest, and average individual are shown. The irradiated skin changes in intensity, but also in colour and therefore an objective observation of change is called for.
Figure 3. The developed erythema in dose interval 46–50 Gy for the lowest, highest and median individual compared to a reference photograph
The corrected RGB mean values were organised in a data matrix (652×3). The matrix was mean-centred and PCA was calculated. In the scoreplot, , results for 0 Gy and results for 36–50 Gy for the three treatment sites were used (294 points). The skew distribution of the values and the risk for outliers necessitated the use of a nonparametric test of significance. A univariate index was constructed by combining the first score with the sign-inverted second score. Wilcoxon Signed Rank Sum Test Citation[25] was chosen. This test showed significant (p = 0.05) differences even for the comparison of 0 and 8 Gy. The median differences of the lotions or between lotion and no lotion were never significant at p = 0.05.
Figure 4. PCA score plot of Digital photography data. ![]()
Laser Doppler
Three Laser Doppler measurements were made in each of the four sites (). Since the Laser Doppler measurement is affected by body temperature and blood pressure, site four was used as a reference. A scar-free area was chosen for calculation of average perfusion in each measured image. The perfusion mean values over the replicates were divided with the reference mean values. Standard deviation was calculated for the 0 Gy Laser Doppler perfusion values. Large individual differences in perfusion were observed leading to a high detection limit as can be seen in and , and the average person does not show a significant increase in perfusion until the last two measurement occasions. The Wilcoxon Signed Rank Sum Test was employed and the detection limit was determined to be 18 Gy. The median differences between the lotions and between lotion and no lotion were never significant.
Figure 5. Relative perfusion, i.e.: Irradiated/Reference skin, for treatment with two different lotions and no lotion as a function of radiation dose. The detection limit is calculated from the relative perfusion values at 0 Gy and is denoted with three standard deviations, 3σ.
Figure 6. The variation in relative perfusion after a radiation dose ≥36 Gy for the different treatments.
Discussion
Analysis of the data from the three non-invasive techniques shows that they all contain information on changes in the skin related to the extent of erythema. Digital Colour Photography and Laser Doppler Imaging gave results that were easy to calculate and interpret and based on these it is certainly possible to evaluate if a specific treatment can prevent radiotherapy-induced erythema. A previous study Citation[26] shows that objective documentation using digital photography is a reliable method. The Laser Doppler technique is also a good candidate for this purpose but it is more time-consuming and less sensitive than the other techniques and therefore might not be the best choice for routine use in the clinic. Digital Colour Photography with its detection limit of 8 Gy, on the other hand is cheap and quick to carry out and is therefore suitable for studying colour changes in the skin. In this case it is of utmost importance to develop reproducible routines and new software to make it useful for clinical practice. Near Infrared Spectroscopy is fast and easy to use but requires expensive instrumentation. The results from the Wilcoxon Signed Rank Sum Test showed a detection limit of 8 Gy.
Therefore, based on the present results Digital Colour Photography is recommended as the cheap and practical method for both objective and subjective evaluation of skin reactions. The other methods could be developed in the future by miniaturisation and software development to complement photography.
No significant effect on the extent of erythema, neither positive nor negative, could be established from using any of the two lotions. These findings support the results from several other studies Citation[6], Citation[16], Citation[17].
The studied lotions may have some beneficial effects, but these are not supported by any of the objective measurements used in the present study. Skin reactions are an accepted side effect of radiotherapy but patients request correct information on what to do in order to decrease the extent of erythema. There is probably no harm in using Aloe vera or Essex lotion during the course of radiotherapy treatment. It is, however, of greatest importance that recommendations of certain skin care products are based on real knowledge and not only vague ideas. Caregivers have a responsibility when recommending topical treatments to patients.
Clinically these different objective methods could be used to clarify inter-patient variation in the degree of erythema developed during radiation treatment. In the future these objective methods might also be an instrument for developing prediction tests to adjust the radiation dose based on the radiosensitivity of the individual patient.
Acknowledgements
The European Union Structure Foundation Objective 1 is recognised for their financial support. PG wishes to thank the Unizon project NIRCE sponsored by Interreg.
References
- Naylor W, Mallett J. Management of acute radiotherapy induced skin reactions: A literature review. Eur J Oncol Nurs 2001; 5: 221–33
- Whiters H. Biological basis of radiation therapy. C. Perez and L. Brady. Philadelphia: Lippincost; 1991.
- Turesson I, Nyman J, Holmberg E, Oden A. Prognostic factors for acute and late skin reactions in radiotherapy patients. Int J Radiat Oncol Biol Phys 1996; 36: 1065–75
- Burnet N, Nyman J, Turesson I, Wurm R, Yarnold J, Peacock J. Prediction of normal-tissue tolerance to radiotherapy from in-vitro cellular radiation sensitivity. Lancet 1992; 339: 1570–1
- Russell NS, Knaken H, Bruinvis IA, Hart AA, Begg AC, Lebesque JV. Quantification of patient to patient variation of skin erythema developing as a response to radiotherapy. Radiother Oncol 1994; 30: 213–21
- Dana J, Thompson J, Meegan M, Haycocks T, Barbieri C, Manchul L. Pilot study to investigate the toxicity of Aloe vera gel in the management of radiation induced skin reactions for post-operative primary breast cancer. J Radiother Pract 2000; 1: 197–204
- De Conno F, Ventafridda V, Saita L. Skin problems in advanced and terminal cancer patients. J Pain Symptom Manage 1991; 6: 247–56
- Halperin E, Gaspar L, George S, Darr D, Pinnell S. A double-blind, randomized, prospective trial to evaluate topical vitamin C solution for the prevention of radiation dermatitis. CNS Cancer Consortium. Int J Radiat Oncol Biol Phys. 1993; 26: 416–6
- Liguori V, Guillemin C, Pesce G, Mirimanoff R. J. B. Double-blind, randomized clinical study comparing hyaluronic acid cream to placebo in patients treated with radiotherapy. Radiother Oncol. 1997; 42: 155–61
- Lokkevik E, Skovlund E, Reitan JB, Hannisdal E, Tanum G. Skin treatment with Bepanthen cream versus no cream during radiotherapy – A randomized controlled trial. Acta Oncol 1996; 35: 1021–6
- Maiche A, Grohn P, Maki-Hokkonen H. Effect of chamomile cream and almond ointment on acute radiation skin reaction. Acta Oncol 1991; 30: 395–6
- Tepmongkol P, Chuthasri S, Rodprasert T, Rattanapol P, Maneenil W. The use of ambiphilic dermatological cream and radiation dermatitis in radiation therapy: A clinical study at Siriraj hospital, Bangkok. J Med Assoc Thai 1981; 64: 328–32
- Maiche A, Isokangas OP, Grohn P. Skin protection by sucralfate cream during electron-beam therapy. Acta Oncol 1994; 33: 201–3
- Bostrom A, Lindman H, Swartling C, Berne B, Bergh J. Potent corticosteroid cream (mometasone furoate) significantly reduces acute radiation dermatitis: Results from a double-blind, randomized study. Radiother Oncol 2001; 59: 257–65
- Maddocks-Jennings W, Wilkinson J, Shillington D. Novel approaches to radiotherapy-induced skin reactions: A literature review. Complement Ther Clin Pract 2005; 11: 224–31
- Williams MS, Burk M, Loprinzi CL, Hill M, Schomberg PJ, Nearhood K, et al. Phase III double-blind evaluation of an aloe vera gel as a prophylactic agent for radiation-induced skin toxicity. Int J Radiat Oncol Biol Phys 1996; 36: 345–9
- Heggie S, Bryant GP, Tripcony L, Keller J, Rose P, Glendenning M, et al. A phase III study on the efficacy of topical aloe vera gel on irradiated breast tissue. Cancer Nursing 2002; 25: 442–51
- Olsen D, Raub W, Bradley C, Jr, Johnson M, Macias J, Love V, et al. The effect of aloe vera gel/mild soap versus mild soap alone in preventing skin reactions in patients undergoing radiation therapy. Oncol Nurs Forum 2001; 28: 543–7
- Nyström J. Multivariate non-invasive measurements of skin disorders. VMC-KBC, Umeå University, Umeå 2006
- Vazques B, Avila G, Segura D, Escalante B. Anti- inflammatory activity of extracts from Aloe vera gel. J Ethnopharmacol 1996; 55: 69–75
- Alan D, Klein M-D, Neal S. Aloe vera. J Am Acad Dermatol 1988; 18: 714–20
- Collins C, Collins C. Roentgen dermatitis treated with fresh whole leaf of Aloe vera. Am J Roentgenol Radium Ther 1935; 33: 396–7
- Nystrom J, Geladi P, Lindholm-Sethson B, Rattfelt J, Svensk A-C, Franzen L. Objective measurements of radiotherapy-induced erythema. Skin Res Technol 2004; 10: 242–50
- Jackson JE. A user's guide to principal components. Wiley, New York 1991
- Wilcoxon F. Individual comparisons by ranking methods. Biometrics 1945; 1: 80–3
- Wengstrom Y, Forsberg C, Naslund I, Bergh J. Quantitative assessment of skin erythema due to radiotherapy – evaluation of different measurements. Radiother Oncol 2004; 72: 191–7
Appendix 1
Aloe vera gel consists of: Aloe barbadensis 97%, aqua, carbomer, sodium hydroxide, phenoxyethanol, methylparben, butylparben, ethylparben, propylparben. Essex lotion consists of: Aqua, petrolatum, glycerin, methyl glucose sesquistearate, dimethicone, PEG-20 methyl glucose sesquistearate, palmitic acid, steric acid, cetyl alcohol, xanchan gum, magnesium aluminum silicate, carbomer, sodium hydroxide.