To the Editor
Sarcomas are amongst the least common tumors clinical oncologists encounter; however even amongst soft tissue sarcomas, subsets requiring distinct treatment plans exist. Gastrointestinal stromal sarcomas (GIST) have undergone a revolutionary paradigm shift in treatment with the discovery of targeted kinase inhibitors; other less treatable soft tissue sarcomas also require distinct treatments, even as regimens continue to evolve Citation[1]. Although clear cell sarcoma, being an uncommon entity, is not in the differential of common paraspinous tumors this rare presentation illustrates several important aspects of truncal sarcoma management for the practicing oncologist.
We report a rare paraspinous clear cell sarcoma. A 38-year-old African-American fireman was admitted to the hospital for severe pain beginning in the left subcostal region and radiating to the left upper quadrant. A magnetic resonance imaging (MRI) scan showed a paraspinous mass 2.0×5.0 cm in size ( and )
Figure 1. Sagital T1-weighted MRI of the thoracic spine showing marrow infiltration, endplate destruction, and paravertebral mass at T5 and T6 level. Note involvement of anterior longitudinal ligament.

Figure 2. Axial view.

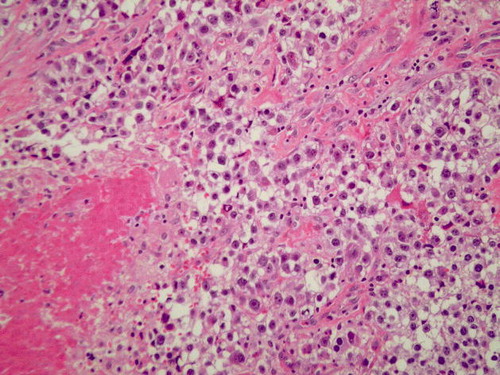
The patient underwent a thoracotomy from a left-sided approach for diagnosis and resection because of the tumor's predominantly left-sided location. Non-necrotic margins displayed a clear cell pattern, initially felt to be consistent with a renal primary. Follow-up immunocytochemical panel included strongly positive results for S100, HMB45, and periodic acid-Schiff (PAS) reaction (). No melanin pigment was seen; a clear cell sarcoma was suspected. Subsequently, the EWS-ATF-1 fusion gene was detected.
Figure 3. Paraspinal tumor. The clear cell sarcoma is comprised of polygonal cells with abundant clear to pale cytoplasm bordered by thin fibrous septae. A small amount of associated necrosis is seen in the lower left hand corner. (H & E section, 200X)
Subsequently, the patient underwent a course of Cisplatin, Dacarbazine, interleukin-2, and interferon. Briefly, the patient received Dacarbazine 250 mg/m2 intravenously on days 1, 2 and 3; Cisplatin 25 mg/m2 on days 1, 2 and 3; interleukin-2 18 million units/m2 days 6–10 and13–15 and interferon 5 million units/m2 on days 6, 8, 10, 13 and 15. After two full cycles of chemotherapy, the patient was noted to have completely responded. No new lymphadenopathy was seen. The tumor subsequently recurred.
Clear cell sarcoma is an uncommon neoplasm first described by Enzinger in 1965 as a distinct type of soft tissue sarcoma Citation[2]. The tumors are primarily diagnosed in the tendons or aponeuroses of the extremities. Because of its histological and immunochemical similarity to melanoma, it has also been called melanoma of the soft parts; like melanoma, the clear cell sarcoma is believed to originate from migrated neural crest cells, and hence, it has been thought that these tumors might respond better to biochemotherapy regimens used typically for malignant melanoma, rather than adriamycin and ifosfamide based regimens used more commonly in the treatment of soft tissue sarcomas Citation[2–6]. Since 1965, less than five hundred cases have been reported, most of which have demonstrated an aggressive malignant behavior with rapidly disseminating disease.
The diagnosis of clear cell sarcoma can be challenging. Histologically, the clear cell sarcoma is characterized by fibrous septa and uniform cells which appear to have a clear eosinophilic cytoplasm, vesicular nuclei, and large basophilic nucleoli Citation[7]. This has led to great difficulty in diagnosis due to a large differential that may include fibrosarcoma, malignant melanoma, synovial sarcoma, and, as with our case's initial diagnosis, renal cell carcinoma. Like lymphomas, however, many soft tissue sarcomas are characterized by translocations. Cytogenetic analysis has revealed a unique genetic marker in these tumors, a translocation from chromosome 12 to chromosome 22 Citation[8–14].
The most effective treatment of a clear cell sarcoma is the complete surgical resection of the tumor. Like epithelioid sarcomas, angiosarcomas, and some liposarcomas, clear cell sarcomas are generally resistant to chemotherapy. The use of standard sarcoma regimens has not been successful. However, the remissions of two metastatic clear cell sarcomas after the use of interferon-alpha 2b (with chemotherapy in one case) have been reported Citation[15], Citation[16]. Hence, interferon was included in the metastatic melanoma regimen we prescribed for our patient who had a transient, albeit complete response Citation[17].
References
- Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in gastrointestinal stromal tumors. N Engl J Med 2002; 347: 472–80
- Enzinger FM. Clear-cell sarcoma of the tendons and aponeuroses: An analysis of 21 cases. Cancer 1965; 18: 1163–74
- Meis-Kindlom JM. Clear cell sarcoma of tendons and aponeuroses: A historical perspective and tribute to the man behind the entity. Adv Anat Pathol 2006; 13: 282–92
- Epstein AL, Martin AO, Kempson R. Use of a newly established human cell line (SU-CCS-1) to demonstrate the relationship of clear cell sarcoma to malignant melanoma. Cancer Res 1984; 44: 1265–74
- Granter S, Weilbaecher K, Quigley C, Fletcher C, Fisher D. Clear cell sarcoma shows immunoreactivity for microphthalmia transcription factor: Further evidence for melanocytic differentiation. Mod Pathol 2001; 14: 6–9
- Kindblom L, Lodding P, Angervall L. Clear-cell sarcoma of tendons and aponeuroses: An immunohistochemical and electron microscopic analysis indicating neural crest origin. Virchows Arch 1983; 401: 109–28
- d'Amore ESG, Ninfo V. Clear cell tumors of the somatic soft tissues: Sem Diagn Pathol 1997; 14: 270–80
- Langezaal SM, Graadt Van Roggen JF, Cleton-Jansen AM, Baeide JJ, Hogendoorn PCW. Malignant melanoma is genetically distinct from clear cell sarcoma of tendons and aponeurosis (malignant melanoma of soft parts). Br J Cancer 2001; 84: 535–8
- Nedoszytko B, Mrózek K, Roszkiewicz A, Kopacz A, Swierblewśki M, Limon J. Clear cell sarcoma of tendons and aponeuroses with t (12;22) (q13;q12) diagnosed initially as malignant melanoma. Cancer Genet Cytogenet 1996; 91: 37–9
- Reeves BR, Fletcher CDM, Gusterson BA. Translocation t(12;22) (q13;q13) is a nonrandom rearrangement in clear cell sarcoma. Cancer Genet Cytogenet 1992; 64: 101–3
- Speleman F, Delattre O, Peter M, Hauben E, Van Roy N, Van Marck E. Malignant melanoma of the soft parts (clear-cell sarcoma): Confirmation of EWS and ATF-1 gene fusion caused by a t(12;22) translocation. Mod Pathol 1997; 10: 496–9
- Stenman G, Kindblom LG, Angervall L. Reciprocal translocation t(12;22) (q13;q13) in clear-cell sarcoma of tendons and aponeuroses. Genes Chromosomes Cancer 1992; 4: 122–7
- Bosilevac JM, Olsen RJ, Bridge JA, Hinrichs S. Tumor cell viability in clear cell sarcoma requires DNA binding activity of the EWS/ATF1 fusion protein. J Biol Chem 1999; 274: 34811–8
- Fujimura Y, Ohno T, Siddique H, Lee L, Rao VN, Reddy EP. The EWS-ATF-1 gene involved in malignant melanoma of soft parts with t(12;22) chromosome translocation, encodes a constitutive transcriptional activator. Oncogene 1996; 12: 159–67
- Lauro S, Bordin F, Trasatti, Lanzetta G, Della Rocca C, Frati L. Concurrent chemoimmunotherapy in metastatic clear cell sarcoma: A case report. Tumori 1999; 85: 512–4
- Steger GG, Wrba F, Mader R, Schlappack O, Dittrich C, Rainer H. Complete remission of metastasised clear cell sarcoma of tendons and aponeuroses. Eur J Cancer 1991; 27: 254–6
- Anderson C, Buzaid A, Legha S. Systemic treatments for advanced cutaneous melanoma. Oncology 1995; 9: 1149–58