To the Editor,
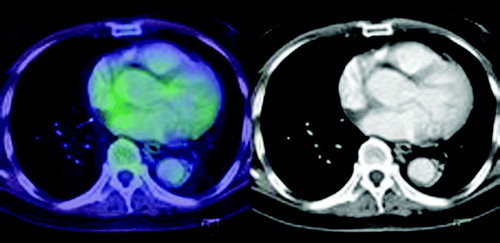
We present a case of a 65-year-old Asian male who presented with difficulty in swallowing and sore throat for one-month duration. A PET/ CT (contrast enhanced) scan showed a locally invasive soft tissue mass in the left tonsillar region as well as extensive Fluorodeoxyglucose(FDG)-avid disease above and below the diaphragm. An intense FDG-avid (SUV max 25) filling defect was noted in the right atrium (). Biopsies taken from the right nasal cavity and tonsil revealed the presence of an extranodal nasal-type NK/T cell lymphoma. The tumour expressed pan-T markers CD2 and CD3e. In situ hybridization for EBV encoded RNA (EBER) and granzyme B were positive. Bone marrow biopsy demonstrated involvement by nasal-type NK/T-cell lymphoma. Thus, the patient had stage IV extranodal nasal-type NK/T cell lymphoma with an international prognostic index (IPI) score of 4. As the patient's left ventricular ejection fraction was depressed at 25–30%, he was commenced on a non-anthracycline-based combination chemotherapy comprising of ifosfamide, carboplatin and etoposide (ICE). Four days after initiation of chemotherapy, the patient developed supraventricular tachycardia, which was refractory to adenosine. Intravenous amiodarone was subsequently started but he continued to experience episodes of atrial fibrillation. The second cycle of ICE chemotherapy was administered on day 14, which was uneventful. The patient's cardiac rhythm subsequently reverted to sinus rhythm. A PET/CT (contrast enhanced) scan performed after the second cycle, showed near complete metabolic resolution of the lymphoma (). Of note, the FDG avid lesion in the right atrium had completely resolved. The patient has completed 4 cycles of ICE chemotherapy and remained in remission.
Figure 1. FDG avid filling defect in the right atrium (arrow) pre-chemotherapy.
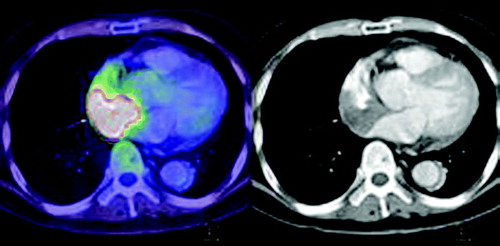
Figure 2. Disappearance of the filling defect in the right atrium post cycle 2 of chemotherapy.
Nasal NK cell lymphomas are classified by the World Health Organization into NK/T cell lymphoma (nasal type) Citation[1] and aggressive NK-cell leukaemia Citation[2]. NK-cell lymphomas are predominantly extranodal and are more commonly seen in Asian and South American populations compared to people in Europe and the United States Citation[3], Citation[8]. The histopathology and immunophenotypic features of extranodal NK/T cell lymphoma have been well described Citation[4]. In this patient, immunostaining for the natural killer cell marker CD56 was negative. Notably, a subset of nasal-type NK/T cell lymphoma lacked expression of the natural killer cell marker CD56/NCAM as reported by Ng et al. in a study of patients in Singapore Citation[5]. However, the biological behaviour is similar to classic CD56+ cases provided there is expression of cytotoxic granules and evidence of EBV infection, both of which were present in this biopsy.
Compared to peripheral T cell lymphoma, the survival of patients with extra-nodal NK/T cell lymphoma is significantly worse Citation[6], Citation[8]. Based on the presence of disseminated nodal disease, stage IV presentation and elevated LDH, our patient has an extremely poor prognosis, with a less than 10% chance of long term survival Citation[7]. In general, NK/T cell lymphomas display an aggressive clinical course and response to conventional, anthracycline-based (mostly CHOP, namely cyclophosphamide, doxorubicin, vincristine and prednisone) regimens is poor. Outcomes are particularly dismal in advanced stages of disease, with complete remission rates of less than 15% Citation[9].
There is currently no established first line treatment in the management of advanced extranodal NK/T cell lymphoma. However, non-anthracycline regimens with ifosfamide or L-asparaginase have shown promising results when used as salvage therapy Citation[10]. Based on these considerations and the fact that our patient had impaired cardiac function, the ICE regimen was selected.
Our patient developed cardiac arrhythmia (supraventricular tachycardia) during the first cycle of ICE chemotherapy. This could be attributed to tumour infiltration of the right atrium, possibly affecting the sino-atrial node or as a direct consequence to chemotherapy (ifosfamide, etoposide) induced cardiac toxicities. The incidence of supra ventricular tachycardia with ifosfamide is about 15% Citation[11]. Considering that fact that our patient's arrhythmias resolved following tumour resolution with the continuation of ICE chemotherapy, lymphomatous cardiac involvement is the most likely cause of his cardiac arryhthmia.
Lymphomatous involvement of the heart has been detected in 14 to 24% of lymphoma patients in systemic autopsy studies Citation[12], Citation[13]. One of the manifestations of cardiac lymphoma includes arrhythmias. Medications such as amiodarone have been successfully used for the control of ventricular tachycardia secondary to cardiac metastasis. Interestingly, this patient's supraventricular tachycardia did not respond to amiodarone or adenosine but resolved only after treatment with chemotherapy and tumour response to it.
The current diagnostic modalities such as echocardiography and computed tomography scans are less useful in the early diagnosis of cardiac lesions Citation[14]. Positron emission tomography (PET) has gained favor as an imaging modality to assess tumour extent and response to chemotherapy and to predict the risk of disease relapse in patients with Hodgkin disease and non-Hodgkin lymphoma Citation[15]. In our case the use of a PET scan has proven clinically useful in diagnosis and the review of treatment response. Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Chan JK, Jaffe ES, Ralfkiaer E. Extranodal NK/T-cell lymphoma, nasal type. Tumours of haematopoietic and lymphoid tissues. World Health Organization Classification of Tumours, ES Jaffe, NL Harris, H Stein, JW Vardiman. IARC Press, Lyon 2001; 204–207
- Chan JK, Wong KF, Jaffe ES, Ralfkiaer E. Aggressive NK-cell leukaemia. Tumours of haematopoietic and lymphoid tissues. World Health Organization Classification of Tumours, ES Jaffe, NL Harris, H Stein, JW Vardiman. IARC Press, Lyon 2001; 198–200
- Au W, Ma SY, Chim CS, Choy C, Loong F, Lie AKW, et al. Clinicopathologic features and treatment outcome of mature T cell and natural killer-cell lymphomas diagnosed according to World Health Organization classification scheme: A single centre experience of 10 years. Ann Oncol 2005; 16: 206–14
- Nava VE, Jaffe ES. The pathology of NK-cell lymphomas and leukemias. Adv Anat Pathol 2005; 12: 27–34
- Ng SB, Lai KW, Murugaya S, Lee KM, Loong SL, Fook-Chong S, et al. Nasal-type extranodal natural killer/T cell lymphomas: A clinicopathologic and genotypic study of 42 cases in Singapore. Mod Pathol 2004; 17: 1097–107
- Vose, JM. The International PTCL Project International Peripheral T-cell Lymphoma (PTCL) Clinical and Pathologic Review Project: Poor outcome by prognostic indices and lack of efficacy with anthracyclines. Blood (ASH Annual Meeting Abstracts). 2005;106:811.
- Lee J, Suh C, Park YH, Ko YH, Bong SM, Lee JH, et al. Extranodal natural killer T-cell lymphoma, nasal type: A prospective model from retrospective multicentre study. JCO 2006; 24: 612–8
- Lim ST, Hee SW, Quek R, Lim LC, Yap SP, Loong EL, et al. Comparative analysis of extra-nodal NK/T-cell lymphoma and peripheral T-cell lymphoma: Significant differences in clinical characteristics and prognosis. Eur J Haematol 2008; 80: 55–60
- Kwong YL. Natural killer-cell malignancies: Diagnosis and treatment. Leukemia 2005; 19: 2186–94
- Lee KW, Yun T, Kim DW, Im SA, Kim TY, Yoon SS, et al. First line ifosfamide, methotrexate, etoposide and prednisolone chemotherapy±radiotherapy is active in stage I/II extranodal NK/T-cell lymphoma. Leuk Lymphoma 2006; 47: 1274–82
- Kandylis K, Vassilomanolakis M, Tsoussis S, Efremidis AP. Ifosfamide cardiotoxicity in humans. Cancer Chemother Pharmacol 1989; 24: 395–6
- Roberts WC, Glancy DL, DeVita VT. Heart in malignant lymphoma (Hodgkin's disease, lymphosarcoma, reticulum cell sarcoma and mycosis fungoides): A study of 196 autopsy cases. Am J Cardiol 1968; 22: 85–107
- Lam KY, Dickens P, Chan ACL. Tumors of the heart: A 20-year experience with a review of 12 485 consecutive autopsies. Arch Pathol Lab Med 1993; 117: 1027–31
- Dorsay TA, Ho VB, Rovira MJ, Armstrong MA, Brisette MD. Primary cardiac lymphoma: CT and MR findings. J Comput Assist Tomogr 1993; 17: 978–81
- Burton C, Ell P, Linch D. The role of PET imaging in lymphoma. Br J Haematol 2004; 126: 772–84