To the Editor
This female patient (65 years of age) was diagnosed in 2002 with infiltrating ductal carcinoma in the right breast, pT1N1M0. Initial therapy included conservative surgery, a breast radiotherapy dose of 50 Gy and a boost dose on the tumour bed with a further 10 Gy, together with adjuvant hormone therapy with tamoxifen.
The patient consulted again in March 2007 due to the appearance of macular lesions over the whole of her right breast. A biopsy showed no neoplastic infiltration. Three months later, the lesions had increased, with the appearance of erythematous nodules (a) spreading to the anterior axillary line. A fresh biopsy revealed an angiosarcoma (AS). As this tumour could not be resected, chemotherapy was started with paclitaxel at 60 mg/m2/weekly for three weeks. A clear response to treatment was seen from the beginning, leading to the disappearance of some lesions and considerable improvements in others.
Figure 1. (a) Angiosarcoma before treatment. (b) Angiosarcoma after 4 months of treatment with Paclitaxel.
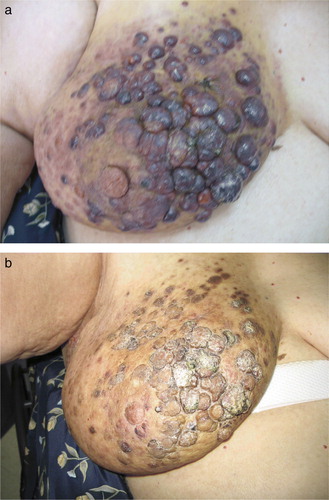
There was a clear clinical response on completion of the first cycle. However, following the second cycle, lesions grew back during the drug-free week. In view of this finding, we resumed uninterrupted paclitaxel therapy at the same dose. Four months later, we saw a continued response to the therapy (b).
Discussion
AS of the breast is very rare (0.04% of all breast tumours) Citation[1]. Over a hundred case reports have been published to date, all in previously irradiated breasts as part of conservative therapy for early-stage breast cancer. These secondary AS appear more frequently in elderly women. They have a latency after breast cancer therapy ranging between 5 and 10 years Citation[2], although short latency times have also been reported Citation[3], Citation[4].
The higher risk of AS in a previously irradiated breast is clearly reflected in the series by Strobbe et al. Citation[5] who estimated an incidence of secondary AS at 0.16%, compared with 0.01% for primary AS.
The relationship between secondary AS of the breast and prior radiotherapy has yet to be thoroughly elucidated. Some authors point to an inversely proportional relationship between radiotherapy dose and latency Citation[6], Citation[7], hereditary factors (certain BRCA1 and BRCA2 mutations) or hormone factors Citation[1].
Pathology diagnosis is achieved through biopsy. As in our case, biopsies do not always yield the expected results. We should not forget that this test may also sometimes give false positive results, especially in low-grade AS that cannot be readily distinguished from radiotherapy-induced changes Citation[3].
Standard therapy entails surgery with complete tumour resection. However, as in our case, chemotherapy becomes the first treatment of choice when surgery is not possible.
Results are far from alone promising for the most widely used drugs. Anthracyclines alone or with iphosphamide have led to disease control after several months (between 7 and 24 months) Citation[8], always in combination with previous surgery. Over the past few years, paclitaxel has been used for used in advanced stage and/or metastatic AS Citation[9], Citation[10].
In our case, the weekly taxane kept the disease under control for five months. Our case reveals the sound profile of paclitaxel as a single agent in the initial treatment of unresectable, radiotherapy-induced AS in an anthracycline-naïve patient.
References
- De Bree E, Van Coevorden F, Peterse J, Russell N, Rutgers E. Bilateral angiosarcoma of the breast after conservative treatment of bilateral invasive carcinoma: Genetic predisposition?. EJSO 2002; 28: 392–5
- Luini A, Gatti G, Galimberti V, Zurrida S, Intra M, Gentilini O, et al. Conservative treatment of breast cancer: Its evolution. Breast Cancer Res Treat 2005; 94: 195–8
- Moe M, Bertelli G. Breast angiosarcoma following lumpectomy and radiotherapy for breast cancer: A case with short latent period and false negative result on biopsies. Ann Oncol 2007; 18: 801–9
- Deutsch M, Sayfan E. Angiosarcoma of the breast occurring soon after lumpectomy and breast irradiation for infiltrating ductal carcinoma: A case report. Am J Clin Oncol 2003; 49: 532–8
- Strobbe LJ, Peterse HL, van Tinteren H, Wijnmaalen A, Rutgers EJ. Angiosarcoma of the breast after conservation therapy for invasive cancer, the incidence and outcome. An unforeseen sequela. Breast Cancer Res Treat 1998; 47: 101–9
- Kirova YM, Vilcoq JR, Asselain B, Sastre-Garau X, Fourquet A. Radiation-induced sarcomas after radiotherapy for breast carcinoma. Cancer 2005; 104: 856–63
- Tomasini C, Grassi M, Pippione M. Cutaneous angiosarcoma arising in an irradiated breast. Dermatology 2004; 209: 208–14
- Sher, T, Hennessy, BT, Valero, V, Trent, J, Broglio, K, Woodward, WA,, et al. Angiosarcoma of the breast. J Clin Oncol 2006;24: 9554 (Abstract).
- Schlemmer, M, Reichardt, P, Verweij, J, Hartmann, JT, Judson, I, Thyss, A, , et al. Paclitaxel in patients with advanced angiosarcomas. J Clin Oncol 2007;25: 10033 (Abstract).
- Penel, N, Bui Nguyen, B, Bay, JO, Cupissol, D, Ray-Coquard, I, Piperno-Neumann, S, , et al. Weekly paclitaxel in metastatic angiosarcoma. A FNCLCC French Sarcoma Group (GSF-GETO) phase II trial. J Clin Oncol 2007;25: 10002 (Abstract).