
Abstract
Background
Although ERAS Program had some advantages in laparoscopic distal gastrectomy (LDG), its efficacy and safety remained unclear. We conducted a systematic review and meta-analysis to assess the efficacy and safety of the ERAS group and the traditional care (TC) group in LDG.
Methods
Multiple databases were retrieved from 1 January 2000 to 30 April 2023. The risk ratio (RR), standardized mean difference (SMD) and their 95% confidence interval (CI) were used to estimate the results.
Results
Our meta-analysis contained 17 randomized controlled trials (RCTs) studies, which comprised 1468 patients. Regarding efficacy, the ERAS group had significantly shorter postoperative time to first flatus (SMD = −1.29 [95% CI: −1.68, −0.90]), shorter time to first defecation (SMD = −1.26 [95% CI: −1.90, −0.61]), shorter hospital stays (SMD = −0.99 [95% CI: −1.34, −0.63]), and lower hospitalization costs (SMD = −1.17 [95% CI: −1.86, −0.48]) compared to the TC group. Furthermore, in the ERAS group, C-reactive protein levels were lower on postoperative days 1, 3 or 4, and 7; albumin levels were higher on postoperative days 3 or 4 and 7; and interleukin-6 levels were lower on postoperative days 1 and 3. Regarding safety, the overall postoperative complication rate was lower in the ERAS group (RR: 0.76 [95% CI: 0.60, 0.97]), but there was no significant difference in the individual postoperative complication rate. Other indicators were also not statistically significant.
Conclusion
The combination of ERAS Program with laparoscopy surgery was safe and effective for the perioperative management of patients with distal gastric cancer.
Key Messages
There was no systematic review and meta-analysis on the efficacy and safety of ERAS Program in LDG, so we included 17 studies comprising 1468 patients.
The results indicated that the application of ERAS Program in LDG can significantly improve treatment effect, accelerate patient recovery, shorten hospital stays, and reduce medical costs. It was worth noting that ERAS was effective in reducing the risk of complications, such as postoperative lung infections.
These findings bring new ideas and enlightenment to clinicians under the traditional nursing mode, and provide evidence-based medicine evidence for clinical practice.
Introduction
Gastric cancer (GC) was a prevalent malignant tumour of the gastrointestinal tract with high incidence rates among individuals over 45 years old [Citation1]. According to the Global Cancer Statistics 2020, GC ranked fifth in incidence and fourth in mortality in the world [Citation2]. Currently, surgery remained the primary treatment for GC [Citation3], which included total and subtotal gastrectomy. The location of the tumour and its surrounding lymph nodes determined the extent of surgical resection, with a higher rate of resection in the distal stomach [Citation4]. However, open surgery had higher complication rates, slower recovery, and worse prognosis compared with minimally invasive surgery [Citation5, Citation6]. In 1994, Kitano et al. first reported laparoscopic distal gastrectomy (LDG) for GC, and this surgical method was widely used due to its benefits (such as less bleeding, faster recovery, and good cosmetic results) [Citation7–11]. Despite the many benefits of LDG, there was still a risk of postoperative complications. Therefore, effective perioperative management was crucial for improving clinical outcomes.
The ERAS Program was a concept that promoted patients to achieve rapid recovery after surgery by using a series of perioperative management to block or reduce the stress response of the body. The ERAS Program, proposed by Professor Kehlet in the 1990s [Citation12], was a perioperative management concept that challenged traditional management methods and could be applied to various surgical procedures. Initially developed for colorectal surgery [Citation13], the ERAS Program had been successfully extended to other gynaecology, bladder, liver and spine surgeries [Citation14–17]. The gastrectomy guidelines released by the International ERAS Society in 2014 was a comprehensive application of perioperative management, including 8 procedure-specific items and 17 not procedure-specific items [Citation18].
Currently, several meta-analysis on ERAS Program for GC patients undergoing laparoscopic surgery had been published [Citation19–23], but we found that these studies did not provide a detailed analysis on the laparoscopic surgical approaches and the surgical resection site of the stomach. For example, Yao et al. [Citation19] and Li et al. [Citation21] only analysed the application of ERAS Program in laparoscopic-assisted gastrectomy, Cao et al. [Citation20] only analysed the application of ERAS Program in laparoscopic total gastrectomy, and Li et al. [Citation22] and Zhang et al. [Citation23] only analysed laparoscopic radical gastrectomy. Meanwhile, all these studies included some non-randomized controlled trials (RCTs), which might lead to unreliable evidence-based evidence. The most common invasive site of GC was the gastric antrum [Citation24, Citation25], which was usually used by distal gastrectomy. The common laparoscopic surgical approaches were total laparoscopic distal gastrectomy (TLDG) and laparoscopic-assisted distal gastrectomy (LADG), but we found the clinical application of ERAS Program in LDG had not been effectively evaluated. Therefore, we conducted a systematic review and meta-analysis of the efficacy and safety of ERAS Program in LDG to provide evidence for clinical practice.
Methods
Protocol and registration
We conducted a systematic review and meta-analysis based on the guidelines outlined in PRISMA [Citation26]. Our research was registered on the Open Science Framework. Check it out at https://osf.io/38ydw.
Search strategy
An extensive search of PubMed, CNKI, and WanFang databases was performed from 1 January 2000 to 30 April 2023. To ensure the accuracy of the retrieval results, the following search terms were used: ‘Distal gastric cancer’ and ‘Enhanced recovery after surgery’. Additionally, we searched the list of references for all retrieved articles. Table S1 listed the detailed retrieval pathways.
Inclusion and exclusion criteria
Inclusion criteria contained: (1) Participant: patients who could receive LDG surgery without preoperative chemotherapy or radiotherapy; (2) Intervention: LDG patients receiving ERAS Program in the ERAS group; (3) Comparison: LDG patients receiving traditional nursing care in the TC group; (4) Outcomes: operative time, intraoperative blood loss, number of lymph node dissection, overall postoperative complication rate, readmission rates, time to first flatus, time to first defecation, length of postoperative hospital stay, hospital costs, C-reactive protein (CRP), albumin (ALB), and interleukin-6 (IL-6); (5) Study design: RCTs.
The following exclusion criteria were contained: (1) Case-control, cohort, and retrospective studies; (2) Duplicate publications, data, or full text were unavailable; (3) Studies did not report in detail on the ERAS Program.
Study selection and data extraction
After using search terms and removing duplicate articles through Endnote 20, all remaining titles and abstracts were carefully screened by two authors (HW and BY). Then, eligible studies needed to be further assessed. If there was any ambiguity, it was necessary to consult the third author (BZ) and resolve it through discussion or negotiation. The two authors (QT and TG) collected basic information from the included studies, including the first author’s name, age, sample size, year of publication, body mass index (BMI), type of study design, study results, and assessment of bias. When multiple reports from the same study were available, we collected the most current and complete studies.
Quality assessment
The quality of the included studies was assessed by two authors (BY and YL) using the Cochrane Collaboration risk of bias tool [Citation26]. The assessment covered several domains, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Each domain was categorized as ‘low risk’, ‘high risk’, or ‘uncertain risk’.
Statistical analysis
We used Review Manager (version 5.4.1; The Cochrane Collaboration) for statistical analysis. MetaXL (Version 5.3) was used to generate the Doi plots. For continuous variables, we used the standardized mean difference (SMD) and its 95% confidence intervals (CIs). For dichotomous variables, we calculated risk ratio (RR) and its 95%CIs. If the article did not directly report mean and standard deviation, but the median and range could be obtained, we should convert them to mean and standard deviation using the technique proposed by McGrath et al. [Citation27]. For studies with zero events, the Review Manager had done this by automatically adding a fixed value (usually 0.5) to all cells [Citation28]. In order to evaluate heterogeneity, we used the I2 and χ2 tests. When the I2 ≥ 50%, we used the random-effects model. If not, a fixed-effects model was applied. Furthermore, substantial heterogeneity was indicated by either the Cochrane test p < 0.10 or I2 > 50%. We performed several subgroup analysis on the following criteria, to explore potential sources of greater heterogeneity: year of study publication (Early ≤ 2015 or Recent > 2015) according to the guidelines for GC released by the International ERAS Society in 2014 [Citation18]; appropriate age (Younger ≤ 60 or Older > 60) was obtained by calculating the median age of each included study; BMI (Normal ≤ 23 or Overweight > 23) as defined by the World Health Organization Classification of BMI for Asia; gender ratio (gender ≤ 2.20 or gender > 2.20) sourced from Global Cancer Statistics 2020[2]. The level of statistical significance was set at p < 0.05.
Sensitivity analysis was performed by removing one study at a time in the Review Manager. The Doi plot was used to assess whether there was publication bias in studies with a sample size of more than 10 studies. We used the Luis Furuya-Kanamori (LFK) index to show asymmetry to detect and quantify publication bias [Citation29]. The LFK index within ± 1 showed that there was symmetry in the Doi plots; an LFK index exceeding ± 1 but within ± 2 showed slight asymmetry; and an LFK index exceeding ± 2 showed significant asymmetry.
Results
Study selection and characteristics
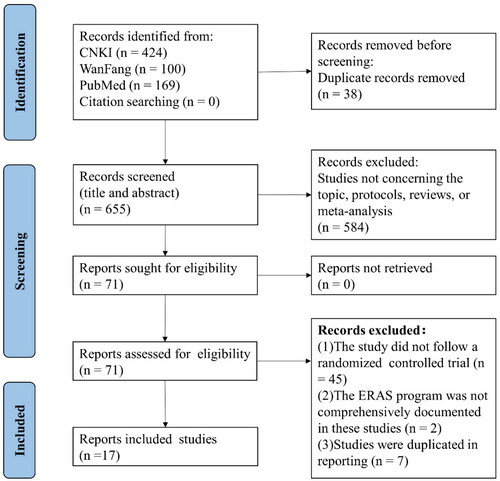
We collected 693 studies, and 38 duplicate studies were removed by using Endnote 20. According to the inclusion and exclusion criteria, we carefully screened the titles and abstracts of 655 studies, and the remaining 71 studies. Ultimately, only 17 studies were eligible for our inclusion criteria. A PRISMA flowchart illustrating the literature screening process was shown in .
Figure 1. PRISMA flowchart of literature selection.
outlined the main characteristics and outcomes of the included studies. All seventeen studies (four studies reported TLDG and thirteen studies reported LADG) were published between 2010 and 2022. In all included studies, there were 738 patients in the ERAS group and 730 patients in the TC group. The ERAS Program must be clearly defined in all studies and each study contained at least seven ERAS items. showed the number of ERAS items used in the ERAS group and TC group. According to the gastrectomy guidelines released by the International ERAS Society in 2014, we could intuitively present the ERAS items included in each study by the radar charts, as shown in . showed all ERAS items included in the ERAS and TC groups, showed before 2015, and showed after 2015.
Figure 2. The reporting results of ERAS items in the included RCTs.
(The ERAS items: 1, Preoperative nutrition; 2, Wound catheters and transversus abdominis plane block; 3, Avoid nasogastric/nasojejunal decompression; 4, Avoiding the use of abdominal drains; 5, Early postoperative diet and artificial nutrition; 6, Preoperative counselling; 7, Preoperative smoking and alcohol consumption; 8, Avoid preoperative bowel preparation; 9, Preoperative fasting and preoperative treatment with carbohydrates; 10, No Preanesthetic Medication; 11, Antithrombotic prophylaxis; 12, Antimicrobial prophylaxis and skin preparation; 13, Epidural analgesia; 14, Intravenous analgesia; 15, Anaesthetic management; 16, Prevention of nausea and vomiting; 17, Avoiding hypothermia; 18, Postoperative glycaemic control; 19, Fluid balance; 20, Early urinary drainage tube removal; 21, Stimulation of bowel movement; 22, Early and scheduled mobilization)
Figure 2 showed the ERAS items reported in both the ERAS and TC groups during different time periods: (A) all, (B) before 2015, (C) after 2015.

Table 1. Basic characteristics of the included RCTs.
Table 2. Number of ERAS items adopted in the included RCTs.
Quality assessment of studies
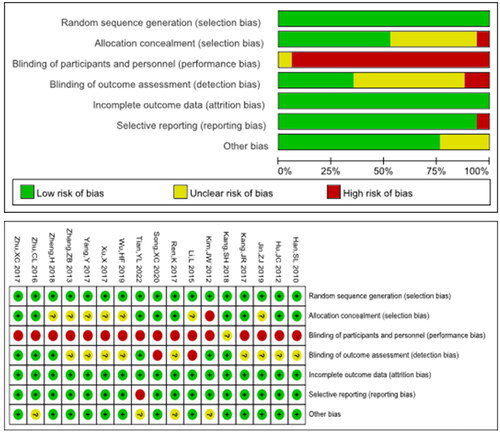
Our study assessed risk of bias using Review Manage 5.4.1. The implementation of the double-blinding method in this type of research had been a challenge. In our study, blindness was considered the main risk of bias. The quality assessment of all the included studies was shown in . Performance bias showed that most of all the included studies had high risk of bias and only one study was uncertain. Blinding of outcome assessment showed that two studies had a high risk of bias. Overall, the risk of bias was defined as moderate to low.
Figure 3. The risk of bias graph and risk of bias summary.
Efficacy of the ERAS Program
Time to first postoperative flatus and defecation
Fifteen studies reported time to first postoperative flatus [Citation30–44]. The results indicated that the ERAS group had shorter time to first postoperative flatus compared to the TC group (SMD = −1.29 [95% CI: −1.68, −0.90]).
Two studies reported time to the first postoperative defecation [Citation33, Citation39]. The results indicated that the ERAS group had shorter time to the first postoperative defecation compared with the TC group (SMD = −1.26 [95% CI: −1.90, −0.61]).
Postoperative hospital stay
Fourteen studies reported postoperative hospital stays [Citation30–41, Citation43, Citation44]. The results indicated that the ERAS group had shorter postoperative hospital stays compared to the TC group (SMD = −0.99 [95% CI: −1.34, −0.63]).
Hospitalization costs
Ten studies reported hospitalization costs [Citation30–37, Citation41, Citation44]. The results indicated that the ERAS group had lower hospitalization costs compared with the TC group (SMD = −1.17 [95% CI: −1.86, −0.48]).
C-reactive protein
Seven studies reported preoperative CRP levels [Citation30, Citation36, Citation38, Citation39, Citation42, Citation45, Citation46]. The difference between ERAS and TC groups did not reach statistically significant (SMD = −0.22 [95% CI: −0.60, 0.17; p = 0.27]). CRP levels on postoperative day POD 1 and 3 or 4 were reported in eight studies [Citation30, Citation31, Citation36, Citation38, Citation39, Citation42, Citation45, Citation46]. The ERAS group had lower CRP levels compared with the TC group in both POD 1 (SMD = −0.58 [95% CI: −1.02, −0.14]) and POD 3 or 4 (SMD = −1.34 [95% CI: −2.04, −0.63]). Three studies reported CRP levels on POD 7 [Citation30, Citation36, Citation38,]. The results indicated that the ERAS group had lower CRP levels compared with the TC group (SMD = −0.82 [95% CI: −1.40, −0.24]).
Albumin
Eight studies reported preoperative ALB levels [Citation30, Citation32, Citation33, Citation35–38, Citation41]. The results indicated that the ERAS group showed a possible trend towards significance compared with the TC group (SMD = 0.17 [95% CI: −0.00, 0.34]). Two studies reported ALB levels on POD 1[Citation38,Citation41,], and the results showed no significant difference between the two groups (SMD = 1.68 [95% CI: −0.12, 3.48]). Seven studies reported ALB levels on POD 3 or 4 [Citation30, Citation32, Citation35–38, Citation41,]. The ERAS group showed higher ALB levels compared with the TC group (SMD = 1.09 [95% CI: 0.72, 1.45]). Six studies reported ALB levels on POD 7 [Citation30, Citation32, Citation35, Citation36, Citation38, Citation41]. The ERAS group showed higher ALB levels (SMD = 1.55 [95% CI: 0.75, 2.36]).
IL-6
Three studies reported IL-6 levels [Citation42, Citation45, Citation46]. The results showed no significant differences in preoperative IL-6 levels between the two groups (SMD = −0.19 [95% CI: −0.91, 0.53]). On POD 1 and POD 3, the levels of IL-6 were significantly lower in the ERAS group compared with the TC group (POD1: SMD = −1.08 [95% CI: −1.54, −0.62]; POD3: SMD = −1.57 [95% CI: −2.52, −0.63]).
All the efficacy outcomes mentioned above had been detailed in .
Table 3. Results of the meta-analysis comparing the efficacy between the ERAS group and TC group.
Safety of the ERAS program
Operative time
Thirteen studies reported operative time [Citation30–33, Citation35, Citation36, Citation38–41, Citation43–45]. The results showed no statistically significant difference between ERAS group and TC group (SMD = −0.06 [95% CI: −0.18, 0.05]).
Intraoperative bleeding volume
Ten studies reported intraoperative bleeding volume [Citation30–33, Citation35, Citation36, Citation38, Citation41, Citation43, Citation45]. The results showed no statistically significant difference between the two groups (SMD = −0.01 [95% CI: −0.16, 0.15]).
Number of lymph node dissection
Six studies reported number of lymph node dissection [Citation30–32, Citation36, Citation38, Citation41]. The results showed no statistically significant difference between the two groups (SMD = −0.06 [95% CI: −0.28, 0.15]).
Readmission rates
Five studies reported postoperative readmission rates [Citation31, Citation36, Citation40, Citation41, Citation44]. The results showed no significant difference between the two groups (RR = 1.22 [95% CI: 0.51, 2.96]).
The overall postoperative complication rate
Fifteen studies reported the overall postoperative complication rate [Citation30–44]. The results showed lower overall rates of postoperative complications in the ERAS group, compared with the TC group (RR = 0.76 [95% CI 0.60, 0.97]).
Each complication was analysed separately. The results showed no statistically significant difference in the incidence of anastomotic leakage, incision infection or liquefaction, intestinal obstruction, deep vein thrombosis, urinary tract infection, and pulmonary complications between the two groups. Pulmonary complications included lung infection, pneumonia, and pleural effusion. When analyzing lung infection separately, the ERAS group showed a possible trend towards significance (RR = 0.46 [95% CI: 0.21, 1.01]).
All the safety outcomes mentioned above had been detailed in .
Table 4. Results of the meta-analysis comparing the safety between the ERAS group and TC group.
Subgroup analysis
There was significant heterogeneity in our studies, particularly in the efficacy results. Therefore, subgroup analysis was used for the exploration of sources of heterogeneity. Recent studies (> 2015) showed that the time to first postoperative flatus was significantly longer compared with earlier studies (≤ 2015) (p = 0.006), but postoperative complications were more likely to be reduced in recent studies (p = 0.01) (Table S2). Male patients had longer hospital stay compared with female patients (p < 0.001). However, male patients had significantly fewer postoperative complications (p = 0.04) (Table S5). Subgroup analysis showed no statistical significance in terms of age (Table S3) and BMI (Table S4). The detailed results were presented in the supplementary tables (Tables S2–S5).
Sensitivity analysis and publication bias
Sensitivity analysis of all study results showed that none of the individual studies significantly affected the overall results, indicating that our findings were stable and reliable.
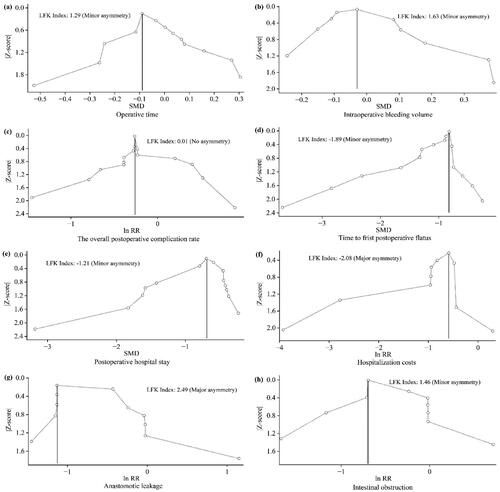
The LFK index was used to assess publication bias. The results indicated that there was no asymmetry in the operative time, the intraoperative bleeding volume, the incidence of overall postoperative complication, the time to first postoperative flatus, the length of hospital stay, and intestinal obstruction. However, there was significant publication bias in hospitalization costs and anastomotic leakage. The results were shown in .
Figure 4. Summary of the Doi plots for each outcome.
Figure 4 showed that publication bias was assessed by Doi plots for each outcome, and asymmetry was indicated using the LFK index for eight outcomes: (a) Operative time, (b) Intraoperative bleeding volume, (c) The overall postoperative complication rate, (d) Time to first postoperative flatus, (e) Postoperative hospital stay, (f) Hospitalization costs, (g) Anastomotic leakage, (h) Intestinal obstruction.
Discussion
So far, our study firstly performed systematic review and meta-analysis on the efficacy and safety of ERAS in LDG. Previous studies had summarized the role of laparoscopy in GC surgery [Citation47–50], as well as the use of ERAS Program in open and laparoscopic gastrectomy [Citation19, Citation21, Citation51–56]. However, our study only focused on the clinical application of ERAS in LDG patients.
Our study indicated that the implementation of the ERAS Program could effectively enhance the recovery of gastrointestinal function in patients after surgery, as evidenced by a significantly earlier time to first flatus (1.29 days) and a shorter time to first defecation (1.26 days) in the ERAS group. The results showed that ERAS could facilitate the recovery of intestinal function and physical strength, as well as alleviate the burden of recovery for the patients.
Postoperative complications were considered to be an important indicator of the success of surgical. The results showed that the overall postoperative complication rate was significantly lower in the ERAS group (p = 0.03). This indicated that incorporating ERAS Programs into standard surgical practice could greatly benefit patients and healthcare providers. Due to the different severity of postoperative complications and their impact on patients, we further analysed the main postoperative complications but found no statistical significance. Interestingly, pulmonary complications (including lung infection, pneumonia and pleural effusion) were not significantly different between the two groups. When analysing lung infections, a possible trend towards significance (p = 0.05) was observed, indicating a potential association that required further investigation. This might be due to differences in the ERAS items and methods used in each study, as well as variations in outcome assessment and measurement [Citation57]. The ERAS Program recommended avoiding nasogastric tube placement before surgery, implementing lung protective ventilation during surgery, preventing of nausea and vomiting, and promoting early ambulation after surgery to reduce postoperative pulmonary complications [Citation58]. The indicated the importance of ensuring the safety of ERAS Program.
Hospital stays and readmission rates were the crucial indicators in the medical care that could provide information about patient recovery and treatment effectiveness. Patients in the ERAS group spent fewer than 1.52 days in the hospital, indicating high quality of medical and nursing care. However, it was an important question in clinical practice whether successful ERAS Program could effectively reduce readmission rates and ultimately improve the life quality for patients [Citation59–61]. The readmission rates showed no significant difference between the ERAS and TC groups (p = 0.65). Although we did not reduce the readmission rate, the shorter hospital stays generally meant the better effect in patients’ treatment and the faster in the postoperative recovery. Additionally, the overall complication rate was also low, indicating that patients received effective treatment. The differences in readmission rates might be related to the different discharge and admission criteria in different regions.
In clinical practice, it was crucial to alleviate the disease burden on patients. Our results indicated that hospitalization costs were lower in the ERAS group, which might lead to a higher level of cost-effectiveness. These findings were generally consistent with previous studies on ERAS Program in laparoscopic gastric cancer surgery [Citation21, Citation51, Citation52, Citation62–64], which might explain the shorter hospital stays and fewer postoperative complications. The key strategy of the ERAS Program was to provide higher quality care at lower costs. However, the study on laparoscopic colorectal surgery showed that the level of compliance with ERAS Program was associated with lower complication rates and shorter hospital stays [Citation65]. Compliance continued to play a key role in implementing and maintaining ERAS Program [Citation66]. Improved compliance to the ERAS Program had been shown to improved postoperative outcomes in previous studies [Citation67–69]. Vifnali et al. found that the ERAS group could reach an overall compliance rate of 85.7% [Citation70]. The successful implementation of ERAS Program required a multidisciplinary team, which needed to communication and cooperation in an effective way [Citation71]. We found that several ERAS items were implemented in the TC group. To visually compare and highlight the differences between ERAS and TC groups, we collected all ERAS items in the included studies and plotted them by the radar chart () [Citation72]. indicated that the studies in ERAS group did not fully comply with the ERAS Program. Theoretically, the complete implementation of ERAS Program could achieve better clinical outcomes, but in clinical practice, most patients were only able to implement some parts of items [Citation73]. Therefore, the implementation and compliance of ERAS Program remained the greatest challenges in clinical practice.
The IL-6 and CRP levels in the blood served as indicators for inflammation and tissue damage, reflecting the acute inflammatory response and extent of involvement of inflammatory tissues [Citation74]. In our study, postoperative IL-6 and CRP levels showed lower in the ERAS group. Furthermore, our study showed that postoperative ALB levels with moderate changes were at a high level in the ERAS group. This adequately supported the concept that laparoscopic surgery by the guidance of the ERAS Program was beneficial to the improvement of nutritional status in GC. The improvement of nutritional status and the acceleration of postoperative recovery made early multimodal treatment possible, which might lead to better oncological outcomes.
There was a certain heterogeneity in our study. The I2value for heterogeneity was approximately between 52% and 95%. Several subgroup analyses were used to explore potential sources of heterogeneity (Tables S2, S3, S4 and S5). According to the release of ERAS guidelines for gastrectomy in July 2014 [Citation18], we believed that subgroup analysis would have certain research significance in 2015. Based on the year of study publication (Early ≤ 2015 or Recent > 2015) (Table S2), we found that patients after 2015 had longer time to first flatus and lower overall postoperative complication rate. Furthermore, our radar chart also visually demonstrated the widespread use of the ERAS Program in clinical practice since 2015 (). Based on the gender ratio (gender ≤ 2.20 or gender > 2.20) (Table S5), our study found that although males had a longer hospital stays than females, they experienced fewer overall complications. However, substantial statistical heterogeneity was observed in the subgroup analysis, which might be attributed to qualitative heterogeneity that we were unable to eliminate completely, such as differences in surgical criteria and technical protocols among medical institutions. Furthermore, poor or varied compliance to ERAS Program could exacerbate heterogeneity.
The advantages of our research were as follows. First, this study was the first meta-analysis on the efficacy and safety of ERAS Program in LDG, and we tried to extract all available data to provide more comprehensive and accurate guidance for clinical practice. Second, we included the most comprehensive RCTs from the database to date, covering all aspects related to laparoscopic distal stomach. Third, we extracted the data of ERAS items in ERAS and TC group respectively, and further used the radar charts to intuitively show the differences of ERAS items in clinical practice between the two groups. Finally, in order to better understand the consistency and reliability of our study, we conducted several subgroup analysis to systematically explore the reasons for the high heterogeneity of study results. We also used Doi plots and LFK index to assess the risk of publication bias more intuitively and visually, compared to the funnel plot and Egger’s test.
However, there were some limitations in our study. First, all the included studies were from Asia (including China, Japan, and South Korea), which might have introduced selection bias. Since the incidence of GC had been steadily increasing in these countries, Western countries had little experience with GC [Citation75]. Therefore, most existing studies on ERAS in GC were mostly focused on Asian populations. Future updates would be necessary for different countries and regions. Second, subgroup analysis showed a high level of heterogeneity and risk of bias, which could be partially explained by the inherent limitations of some studies included in this meta-analysis. These limitations might include operator skill level, incomplete application of the ERAS Program in clinical practice, and using different perioperative management before the release of the ERAS guidelines for gastrectomy. Third, in the process of collecting studies, the vast majority of studies only reported short-term results, while few studies reported long-term results (including survival time, disease-free survival, tumour regression, etc.). Therefore, our studies also did not calculated any long-term results [Citation44]. In the future, we hoped to have standardized and qualified large sample clinical randomized trials to support this aspect of research. Finally, differences in compliance might have influenced the results of our study. Future studies should standardize outcome reporting and program implementation to avoid reducing the benefits of ERAS Program due to different levels of compliance.
Conclusion
In conclusion, our systematic review and meta-analysis comprehensively assessed the efficacy and safety of the ERAS Program in LDG. The combination of the ERAS Program and LDG resulted in accelerated recovery of gastrointestinal function, shorter hospital stays, lower costs, reduced overall postoperative complications, and improved nutritional status without increasing operation time, bleeding volume, lymph node dissection, or readmission rates. Therefore, the ERAS Program as a standard perioperative management for LDG could provide evidence-based medical evidence for clinical practice.
Author contributions
Concept and design: Qihui Tian and Bo Zhu; data collection and analysis: Hongying Wang and Tianyu Guo; drafting of the article: Qihui Tian; critical revision of the article: Bing Yao and Yefu Liu; study supervision: Bo Zhu. All authors have given their approval for the article.
Ethical approval
Ethical approval was not required for this study.
Supplemental Material
Download MS Word (37.7 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Authors of included studies should be contacted individually for further details.
References
- Machlowska J, Baj J, Sitarz M, et al. Gastric cancer: epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int J Mol Sci. 2020;21(11):1. doi: 10.3390/ijms21114012.
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2021;71(3):209–14.
- Smith JK, McPhee JT, Hill JS, et al. National outcomes after gastric resection for neoplasm. Arch Surg. 2007;142(4):387–393. doi: 10.1001/archsurg.142.4.387.
- Johnston FM, Beckman M. Updates on management of gastric cancer. Curr Oncol Rep. 2019;21(8):67. doi: 10.1007/s11912-019-0820-4.
- Zhu Z, Li L, Xu J, et al. Laparoscopic versus open approach in gastrectomy for advanced gastric cancer: a systematic review. World J Surg Oncol. 2020;18(1):126. doi: 10.1186/s12957-020-01888-7.
- Kim W, Kim HH, Han SU, et al. Decreased morbidity of laparoscopic distal gastrectomy compared with open distal gastrectomy for stage I gastric cancer: short-term outcomes from a multicenter randomized controlled trial (KLASS-01). Ann Surg. 2016;263(1):28–35. doi: 10.1097/SLA.0000000000001346.
- Lee HJ, Hyung WJ, Yang HK, et al. Short-term outcomes of a multicenter randomized controlled trial comparing laparoscopic distal gastrectomy with D2 lymphadenectomy to open distal gastrectomy for locally advanced gastric cancer (KLASS-02-RCT). Ann Surg. 2019;270(6):983–991. doi: 10.1097/SLA.0000000000003217.
- Japanese Gastric Cancer Association. Japanese gastric cancer association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. 2021;24(1):1–21. doi: 10.1007/s10120-020-01042-y.
- Huscher CGS, Mingoli A, Sgarzini G, et al. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer. Ann Surg. 2005;241(2):232–237. doi: 10.1097/01.sla.0000151892.35922.f2.
- Adachi Y, Suematsu T, Shiraishi N, et al. Quality of life after laparoscopy-assisted Billroth I gastrectomy. Ann Surg. 1999;229(1):49–54. doi: 10.1097/00000658-199901000-00006.
- Kitano S, Iso Y, Moriyama M, et al. Laparoscopy-assisted billroth I gastrectomy. Surg Laparoscopy Endoscopy. 1994;4(2):146–148.
- Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–617. doi: 10.1093/bja/78.5.606.
- Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: enhanced recovery after surgery (ERAS) group recommendations. Arch Surg. 2009;144(10):961–969.) doi: 10.1001/archsurg.2009.170.
- Cerantola Y, Valerio M, Persson B, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: enhanced recovery after surgery (ERAS(®)) society recommendations. Clin Nutr. 2013;32(6):879–887. doi: 10.1016/j.clnu.2013.09.014.
- Nelson G, Bakkum-Gamez J, Kalogera E, et al. Guidelines for perioperative care in gynecologic/oncology: enhanced recovery after surgery (ERAS) society recommendations-2019 update. Int J Gynecol Cancer. 2019;29(4):651–668. doi: 10.1136/ijgc-2019-000356.
- Song W, Wang K, Zhang RJ, et al. The enhanced recovery after surgery (ERAS) program in liver surgery: a meta-analysis of randomized controlled trials. SpringerPlus. 2016;5(1):207. doi: 10.1186/s40064-016-1793-5.
- Grasu RM, Cata JP, Dang AQ, et al. Implementation of an enhanced recovery after spine surgery program at a large cancer center: a preliminary analysis[J]. J Neurosurg Spine. 2018;29(5):588–598. doi: 10.3171/2018.4.SPINE171317.
- Mortensen K, Nilsson M, Slim K, et al. Consensus guidelines for enhanced recovery after gastrectomy. Br J Surg. 2014;101(10):1209–1229. doi: 10.1002/bjs.9582.
- Yao Y, Yao YC. Meta-analysis of accelerating rehabilitation surgery in laparoscopically assisted radical gastrectomy for distal gastric cancer. Journal of Modern Medicine and Health. 2019;35(1):43–47. +51.
- Cao S, Zheng T, Wang H, et al. Enhanced recovery after surgery in elderly gastric cancer patients undergoing laparoscopic total gastrectomy. J Surg Res. 2021;257:579–586. doi: 10.1016/j.jss.2020.07.037.
- Li Z, Wang Q, Li B, et al. Influence of enhanced recovery after surgery programs on laparoscopy-assisted gastrectomy for gastric cancer: a systematic review and meta-analysis of randomized control trials. World J Surg Oncol. 2017;15(1):207. doi: 10.1186/s12957-017-1271-8.
- Li M Z, Wu W h, Li L, et al. Is ERAS effective and safe in laparoscopic gastrectomy for gastric carcinoma? A meta-analysis. World J Surg Oncol. 2018;16(1):17. doi: 10.1186/s12957-018-1309-6.
- Zhang MK, Peng ZH, Huang H, et al. Meta-analysis of the role of enhanced recovery after surgery in laparoscopic radical gastrectomy for gastric cancer. Journal of Laparoscopic Surgery. 2021;26(8):567–575.
- Gu Y, Chen G, Zhang Y, et al. The relationship among the location, age and clinicopathologic features of gastric cancer patients[J]. Progress in Modern Biomedicine. 2019;19(16):3119–3123.
- Liu K, Yang K, Zhang W, et al. Changes of esophagogastric junctional adenocarcinoma and gastroesophageal reflux disease among surgical patients during 1988-2012: a single-institution, high-volume experience in China. Ann Surg. 2016;263(1):88–95. doi: 10.1097/SLA.0000000000001148.
- Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019;10(10):ED000142. doi: 10.1002/14651858.ED000142.
- McGrath S, Zhao X, Steele R, et al. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020;29(9):2520–2537. doi: 10.1177/0962280219889080.
- Friedrich JO, Adhikari NKJ, Beyene J. Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med Res Methodol. 2007;7(1):5. doi: 10.1186/1471-2288-7-5.
- Furuya-Kanamori L, Barendregt JJ, Doi SAR. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int J Evid Based Healthc. 2018;16(4):195–203. doi: 10.1097/XEB.0000000000000141.
- Chen Hu J, Xin Jiang L, Cai L, et al. Preliminary experience of Fast-Track surgery combined with Laparoscopy-Assisted radical distal gastrectomy for gastric cancer. J Gastrointest Surg. 2012;16(10):1830–1839.,. doi: 10.1007/s11605-012-1969-4.
- Kim JW, Kim WS, Cheong JH, et al. Safety and efficacy of fast-track surgery in laparoscopic distal gastrectomy for gastric cancer: a randomized clinical trial. World J Surg. 2012;36(12):2879–2887. doi: 10.1007/s00268-012-1741-7.
- Zhang ZB. Clinical study of fast track surgery combined with laparoscopic resection for distal gastric cancer. Qingdao University, 2013.
- Zhu CL, Fu T, Cai X. Fast-track surgery could improve postoperative recovery in radical distal gastrectomy patients. Journal of Modern Oncology. 2016;24(12):1926–1930.
- Ren K. Application of rapid rehabilitation concept in abdominal cavity distal radical gastric cancer. Journal of Medical Forum. 2017;38(7):65–66. +69.
- Xu X. Evaluation of the effect of Enhanced recovery after surgery (ERAS) on laparoscopy-assisted distal gastrectomy. Shanxi Medical University,2017.
- Yang Y. The application of enhanced recovery after surgery combined with laparoscopy-assisted distal gastrectomy for gastric cancer. Nanchang University, 2017.
- Zhu XC, Hu JP, Wang Y. Safety and feasibility of fast track surgery combined with laparoscopic in distal gastrectomy. The Practical Journal of Cancer. 2017;32(5):760–762.
- Kang JR. Application of fast track surgery in laparoscopic radical gastrectomy for distal gastric cancer. Journal of Qilu Nursing. 2017;23(18):3–6.
- Zheng H. Application of enhanced recovery after surgery in perioperative period patients with laparoscopic radical gastrectomy[D]. Guangdong Medical University, 2018.
- Kang SH, Lee Y, Min SH, et al. Multimodal enhanced recovery after surgery (ERAS) program is the optimal perioperative care in patients undergoing totally laparoscopic distal gastrectomy for gastric cancer: a prospective, randomized, clinical trial. Ann Surg Oncol. 2018;25(11):3231–3238. doi: 10.1245/s10434-018-6625-0.
- Wu YF. The clinical application of Enhanced recovery after surgery (ERAS) on complete laparoscopic radical of distal gastric cancer. Zhejiang University,2019.
- Jin ZJ. Comparative study of the effects of different perioperative management methods on patients undergoing total laparoscopic surgery for gastric cancer. Hebei Medical University, 2019.
- Song XC, Lu YW, Wu C, et al. Application of enhanced recovery after surgery in total laparoscopic D2 radical resection for distal gastric cancer. Journal of Clinical Surgery. 2020;28(5):456–459.
- Tian YL, Cao SG, Liu XD, et al. Randomized controlled trial comparing the short-term outcomes of enhanced recovery after surgery and conventional care in laparoscopic distal gastrectomy (GISSG1901). Ann Surg. 2022;275(1):e15–e21. doi: 10.1097/SLA.0000000000004908.
- Han SL, Ruo QJ. The impact of fast track surgery on host cell-mediated immunfly and inflammatory responses in patients after gastrectomy for gastric cancer. Chinese Journal of Aesthetic Medicine. 2010;19(z2):124–125.
- Li L, Sun GF, Xin JJ, et al. Effect of fast track surgery on immune function after laparoscopic surgery for patients with gastric cancer. Journal of Precision Medicine. 2015;30(4):451–454.
- Lei X, Wang Y, Shan F, et al. Short-and long-term outcomes of laparoscopic versus open gastrectomy in patients with gastric cancer: a systematic review and meta-analysis of randomized controlled trials. World J Surg Oncol. 2022;20(1):405. doi: 10.1186/s12957-022-02818-5.
- Lou S, Yin X, Wang Y, et al. Laparoscopic versus open gastrectomy for gastric cancer: a systematic review and meta-analysis of randomized controlled trials. Int J Surg. 2022;102:106678. doi: 10.1016/j.ijsu.2022.106678.
- Zeng F, Chen L, Liao M, et al. Laparoscopic versus open gastrectomy for gastric cancer. World J Surg Oncol. 2020;18(1):20. doi: 10.1186/s12957-020-1795-1.
- Zhang Y, Ji G, Tao KX, et al. Application of laparoscopic and open gastrectomy in enhanced recovery after surgery for gastric cancer: analysis of data from multiple centers in China. Journal of Southern Medical University. 2021;41(12):1828–1834.
- Wee IJY, Syn NLX, Shabbir A, et al. Enhanced recovery versus conventional care in gastric cancer surgery: a meta-analysis of randomized and non-randomized controlled trials. Gastric Cancer. 2019;22(3):423–434. doi: 10.1007/s10120-019-00937-9.
- Ni X, Jia D, Guo Y, et al. The efficacy and safety of enhanced recovery after surgery (ERAS) program in laparoscopic digestive system surgery: a meta-analysis of randomized controlled trials. Int J Surg. 2019;69:108–115. doi: 10.1016/j.ijsu.2019.07.034.
- Li Z, Zhao Q, Bai B, et al. Enhanced recovery after surgery programs for laparoscopic abdominal surgery: a systematic review and meta-analysis. World J Surg. 2018;42(11):3463–3473. doi: 10.1007/s00268-018-4656-0.
- Ding J, Sun B, Song P, et al. The application of enhanced recovery after surgery (ERAS)/fast-track surgery in gastrectomy for gastric cancer: a systematic review and meta-analysis. Oncotarget. 2017;8(43):75699–75711. doi: 10.18632/oncotarget.18581.
- Huang ZD, Gu HY, Zhu J, et al. The application of enhanced recovery after surgery for upper gastrointestinal surgery: meta-analysis. BMC Surg. 2020;20(1):3. doi: 10.1186/s12893-019-0669-3.
- Changsheng H, Shengli S, Yongdong F. Application of enhanced recovery after surgery (ERAS) protocol in radical gastrectomy: a systemic review and meta-analysis. Postgrad Med J. 2020;96(1135):257–266. doi: 10.1136/postgradmedj-2019-136679.
- Ljungqvist O, de Boer HD, Balfour A, et al. Opportunities and challenges for the next phase of enhanced recovery after surgery: a review. JAMA Surg. 2021;156(8):775–784. doi: 10.1001/jamasurg.2021.0586.
- Tian YL, Cao SG, Liu XD, et al. Short- and long-term outcomes associated with enhanced recovery after surgery protocol vs conventional management in patients undergoing laparoscopic gastrectomy. World J Gastroenterol. 2020;26(37):5646–5660. doi: 10.3748/wjg.v26.i37.5646.
- Lyu H, Wick EC, Housman M, et al. Patient satisfaction as a possible indicator of quality surgical care. JAMA Surg. 2013;148(4):362–367. doi: 10.1001/2013.jamasurg.270.
- Khorgami Z, Andalib A, Aminian A, et al. Predictors of readmission after laparoscopic gastric bypass and sleeve gastrectomy: a comparative analysis of ACS-NSQIP database. Surg Endosc. 2016;30(6):2342–2350. doi: 10.1007/s00464-015-4477-2.
- Lyon A, Solomon MJ, Harrison JD. A qualitative study assessing the barriers to implementation of enhanced recovery after surgery. World J Surg. 2014;38(6):1374–1380. doi: 10.1007/s00268-013-2441-7.
- Liu Q, Ding L, Jiang H, et al. Efficacy of fast track surgery in laparoscopic radical gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials. Int J Surg. 2018;50:28–34. doi: 10.1016/j.ijsu.2017.12.026.
- Wang LH, Zhu RF, Gao C, et al. Application of enhanced recovery after gastric cancer surgery: an updated meta-analysis. World J Gastroenterol. 2018;24(14):1562–1578. doi: 10.3748/wjg.v24.i14.1562.
- Yu Z, Zhuang CL, Ye XZ, et al. Fast-track surgery in gastrectomy for gastric cancer: a systematic review and meta-analysis. Langenbecks Arch Surg. 2014;399(1):85–92. doi: 10.1007/s00423-013-1148-4.
- Pisarska M, Pędziwiatr M, Małczak P, et al. Do we really need the full compliance with ERAS protocol in laparoscopic colorectal surgery? A prospective cohort study. Int J Surg. 2016;36(Pt A):377–382. doi: 10.1016/j.ijsu.2016.11.088.
- Messenger DE, Curtis NJ, Jones A, et al. Factors predicting outcome from enhanced recovery programmes in laparoscopic colorectal surgery: a systematic review. Surg Endosc. 2017;31(5):2050–2071. doi: 10.1007/s00464-016-5205-2.
- Okrainec A, Aarts MA, Conn LG, et al. Compliance with urinary catheter removal guidelines leads to improved outcome in enhanced recovery after surgery patients. J Gastrointest Surg. 2017;21(8):1309–1317. doi: 10.1007/s11605-017-3434-x.
- ERAS Compliance Group. The impact of enhanced recovery protocol compliance on elective colorectal cancer resection: results from an international registry. Ann Surg. 2015;261(6):1153–1159.
- Pecorelli N, Hershorn O, Baldini G, et al. Impact of adherence to care pathway interventions on recovery following bowel resection within an established enhanced recovery program. Surg Endosc. 2017;31(4):1760–1771. doi: 10.1007/s00464-016-5169-2.
- Vignali A, Elmore U, Cossu A, et al. Enhanced recovery after surgery (ERAS) pathway vs traditional care in laparoscopic rectal resection: a single-center experience. Tech Coloproctol. 2016;20(8):559–566. doi: 10.1007/s10151-016-1497-4.
- Pearsall EA, Meghji Z, Pitzul KB, et al. A qualitative study to understand the barriers and enablers in implementing an enhanced recovery after surgery program. Ann Surg. 2015;261(1):92–96. doi: 10.1097/SLA.0000000000000604.
- Li X, Li Y, Guo K, et al. Evidence based social science in China paper 3: the quality of social science RCTs published from 2000-2020. J Clin Epidemiol. 2022;141:64–73. doi: 10.1016/j.jclinepi.2021.09.014.
- Fangzheng Y, Hao W, Dongsheng W, et al. The effect of perioperative ERAS pathway management on short-and long-term outcomes of gastric cancer patients. Natl Med J China. 2020;100(12):922–927.
- Feng J, Li K, Li L, et al. The effects of fast-track surgery on inflammation and immunity in patients undergoing colorectal surgery. Int J Colorectal Dis. 2016;31(10):1675–1682. doi: 10.1007/s00384-016-2630-6.
- Salvans S, Grande L, Dal Cero M, et al. State of the art of enhanced recovery after surgery (ERAS) protocols in esophagogastric cancer surgery: the Western experience[J]. Updates Surg. 2023;75(2):373–382. doi: 10.1007/s13304-022-01311-8.