
Abstract
Purpose: Previous studies that evaluated the prevalence of hypertension in Nigeria were either clinic based, non-standardized or did not include out-of-clinic blood pressure (BP) measurement.
Materials and Methods: We selected a rural and an urban community in one state in each of the 6 geopolitical zones of Nigeria. Five consecutive BP of adults older than 18 years were measured in the clinic following which, each participant was provided with a home BP device to obtain duplicate morning and evening BP for 3 days.
Result: Out of 556 invited from Anambra State, South-East Nigeria, 490 (88%) consented. Overall, more women participated in both rural (115 vs 61, p < .0001) and urban (213 vs 101; p < .0001) sites. About 35.9% of participants had their home BP monitored. Of the 4890 clinic BP readings, 29.8%, 16.3%, 16.6%, 16.4% and 20.8% ended in 0,2,4,6 and 8 digits respectively. Only 0.8% ended in odd numbers. Of the identical BP readings,5 (0.20%), 6 (0.25%), 56 (2.30%) and 316 (12.9%) SBP and 8 (0.33%), 17 (0.70%), 93 (3.80%), 319 (13.1%) DBP had no difference in five, four, three and two values of the five consecutive readings.
Conclusion: REMAH is feasible and the quality of BP will ensure that the final results are robust.
Introduction
According to the 2016 Global Burden of Disease Study [Citation1], hypertension was the greatest cause of disease burden having been responsible for 89.9 million and 124.1 million disability adjusted life years (DALYs) in women and men respectively. In comparison to other 83 behavioral, environmental and occupational; and metabolic risks or clusters of risks, it was the leading risk factor for DALYs in women and second only to cigarette smoking in men. Emerging evidence [Citation2,Citation3] indicate that while the prevalence, awareness and control of hypertension is declining in many high income countries, the reverse is the case in many low and middle-income nations. Nigeria, the most populous Black nation expectedly contributes a major chunk to this burden. Recent standardised epidemiological survey to substantiate this claim is lacking.
A substantial number of studies [Citation4–6] have been conducted to ascertain the burden of hypertension in Nigeria. However, wide variations are reported in terms of prevalence due to varying target populations, non-uniform criteria for diagnosis and small sample size. The only nationwide survey on hypertension [Citation7] conducted so far in the country was carried out almost two decades ago. In addition to the obvious obsolete nature of that survey in the face of changing patterns of disease reported worldwide, the threshold value for diagnosis of hypertension used at that time was 160/95 mm Hg. Furthermore, this survey as well as other previous small regional studies [Citation4–6] considered the diagnosis of hypertension on the basis of clinic blood pressure alone. This approach underestimates the true burden of hypertension as recent methods of measuring blood pressure outside the clinic have revealed that a great number of individuals with normal clinic pressures (i.e. blood pressure less than 140/90 mmHg) are hypertensive when they are evaluated outside the clinic [Citation8,Citation9]. Hypertension masked to conventional clinic measurement confers a cardiovascular risk close to that of sustained hypertension [Citation10].
Removing the Mask on Hypertension (REMAH) study is a nationwide survey of hypertension which was designed to capture the individuals whose hypertension are ‘masked’ to clinic blood pressure evaluation. This present report is aimed at presenting the rationale and design of the study and the quality control of blood pressure measurement. To demonstrate the feasibility of REMAH, we included the baseline characteristics of the participants recruited from the South-East Nigeria; the first region that was surveyed.
Methods
Sampling/sample size
To determine the sample size that is sufficiently powered to estimate the prevalence of both masked and clinic hypertension, we used the prevalence rates of 10 and 40% respectively based on previous small survey of masked hypertension by our group [Citation9] and recent review of studies [Citation4,Citation6] on prevalence rates of hypertension in Nigeria. Considering a static confidence level of 95%, we estimated that we needed to evaluate home and clinic blood pressure in at least 812 and 2166 participants to estimate the prevalence of masked hypertension and clinic hypertension respectively within 1% margin of error. To account for attrition, we increased the numbers to 850 and 2600 respectively.
To have a representative sample of the entire country, this sample size was apportioned to each of the 6 geopolitical regions in accordance with the 2006 census distribution () [Citation11]. We chose the specific sampling units using a multistage cluster sampling method. In the first stage, we chose one state out of the each six geopolitical zones followed by the local government area and later the specific enumeration areas by simple random sampling in the second and third stage respectively.
Figure 1. Map of Nigeria showing the division into the geopolitical zones and population figures according to 2006 nationwide census [Citation11]. (M stands for Million).
![Figure 1. Map of Nigeria showing the division into the geopolitical zones and population figures according to 2006 nationwide census [Citation11]. (M stands for Million).](/cms/asset/9b59122e-fc10-40b1-b3b8-e559bdef7790/iblo_a_1612706_f0001_b.jpg)
Ethics
REMAH complies strictly with the guidelines for conducting research in human subjects as spelt out in Helsinki Declaration [Citation12]. The University of Abuja Teaching Hospital Health Research Ethics Committee approved REMAH study. Potential participants were educated about the study in a language they understood very well and consenting individuals signed the informed consent. Following the evaluation, in line with the principles of beneficence as enunciated in Belmont Report [Citation13], consultant cardiologists reviewed results of the blood pressure, electrocardiogram, cholesterol and fasting blood glucose before they were made available to the participants. The physicians thereafter referred those who had obvious abnormality including hypertension, diabetes and dyslipidemia to the nearest secondary health centers to the study site.
Community mobilization
Ahead of the actual visit by the field workers, each regional representative carried out a sensitization meeting with the traditional and religious leaders of the communities to be visited. At such meetings, REMAH investigators educated the community leaders about the rationale and objectives of the study. The stakeholders meeting afforded the leaders opportunity to ask questions on grey areas of the study. Awareness is also created using the town criers and community social media fora especially in the urban areas.
Research management
The Circulation Health Research Laboratory of the University of Abuja is responsible for the overall coordination of REMAH including quality control. The office also hired and trained 8 field workers (2 women and 6 men) in technical issues including blood pressure measurement, ECG recording, blood sampling and questionnaire administration. Two trainings were mounted, one prior to the fieldwork and the second midway into the project. To ensure consistency, the same field workers carried out the research in all the 6 regions of the country. Local adhoc staff were recruited in each locality to encourage community participation. The locally recruited staff however are not involved in the technical aspects of the study. The Circulation Health Research Laboratory constructs and maintains the database; runs the statistical analysis and ensures strict compliance to the protocol. Six coordinators, one for each geopolitical zones of the country were responsible for community moblisation and ensuring smooth exercise in their respective zones. Two investigators meetings have held since the inception of REMAH.
General design
Selected communities are mapped, houses systematically numbered and visited to obtain informed consents from interested household members aged 18 yrs and above. Consenting respondents are invited to a mobile clinic where various physical and clinical examinations are carried out, including anthropometry, electrocardiography, blood pressure measurement, questionnaire administration and specimen collection. Biological specimens are handled using standard procedure and transferred to Circulation Health Research Laboratory at the University of Abuja for analysis. Results from the laboratory analysis, ECG and questionnaire data are archived in password-protected computers (See ).
Figure 2. Study design of the REMAH study.
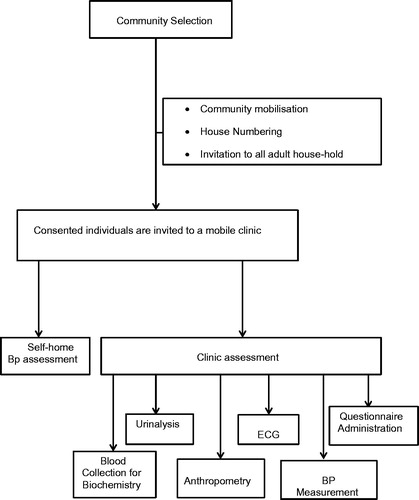
Figure 3. Cross-classification of hypertension. Diagnostic threshold for out-of-office BP assessment depicted include self-measured home BP (home), Day-time ambulatory BP (Day), Night time ambulatory BP (Night) and 24 hour ambulatory BP (24-h).
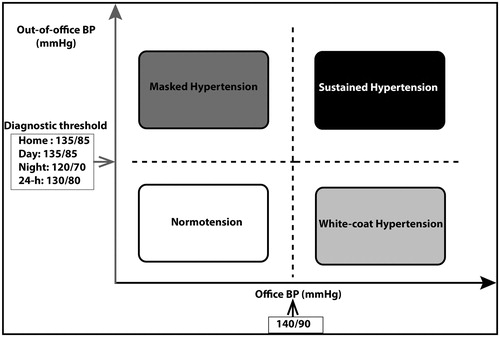
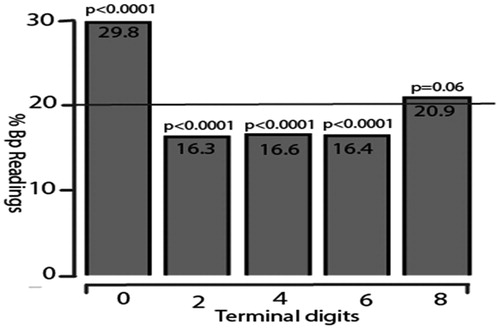
Figure 4. Terminal digit of the five consecutive systolic and diastolic blood pressure (BP) readings (4890 readings, 2445 each of systolic and diastolic BP measurements taken from each of the 490 participants). Numbers along the horizontal axis denote the terminal digits and the percentages are on the vertical axis. The reference line of 20% denotes the expected. *P for equal proportions (20% expected for each of the five end digits).
Blood pressure measurement
Office
Observers received training on blood pressure measurement using the British Hypertension Society video. They measured brachial blood pressure by auscultation of the Korotkoff sounds at the non-dominant arm, according to the 2013 guidelines of the European Society of Hypertension [Citation14]. After the participants had rested in the sitting position for at least 5 minutes, the observers obtained five consecutive blood pressure readings at an interval of 30 to 60 seconds. Systolic and phase V diastolic blood pressures were determined to the nearest 2 mm Hg. Standard cuffs that had a 12 × 24 cm inflatable portion were used. If the upper arm circumference exceeded 31cm, larger cuffs with 15 × 35 cm bladder were used instead.
Home
Following the evaluation at the mobile clinic, individual participants are trained on how to use the validated [Citation15] oscillometric device (OMRON 705IT, OMRON Health Care Europe). They are guided on how to measure their own blood pressure by the fieldworkers under the supervision of the observers immediately afterwards. Each participant went home with the oscillometric device to measure his or her blood pressure two times in the morning shortly after waking up and two times in the evening before going to bed for 3 days. A recording card with provisions for entering the blood pressure values were also provided for the subjects with which they enter the blood pressure readings immediately they were collected.
Quality control for office and home blood pressure measurement
The following measures are to improve the quality of blood pressure measurement. First, the last digit of the blood pressure value must be even i.e., 0, 2, 4, 6, or 8 (and not 3, 5, 7, or 9). Digit preferences of the observers are monitored at 1-monthly intervals throughout the REMAH project. Second, during the initial and at the mid-term training, the observers must pass a test requiring them to read blood pressures from a video tape featuring a falling mercury column with Korotkoff sounds (Blood pressure measurements, British Medical Association, London, England) and the readings must comply within 5 mm Hg of those of experienced physicians. For the home blood pressure monitoring, household members usually younger and more educated accompanied their older illiterate relations and were helpful in ensuring that the procedure for home blood pressure monitoring was strictly adhered to and records properly entered in the cards provided.
Cross-classification of hypertension
Measurement of blood pressure outside the clinic environment using self-measured home or ambulatory blood pressure monitoring allows the classification of individuals into true normotensive, white coat hypertensive, masked hypertensive and sustained hypertensive subjects. The true normotensive individuals have normal pressure in both clinic and outside the clinic environment. The white coat hypertensive individuals have blood pressure in the hypertensive range when their blood pressures are measured in the clinic but normal range when measured out of the clinic. The masked hypertensive patients have normal blood pressure in the clinic environment but blood pressure in the hypertensive range outside the clinic; while the sustained hypertensive patients have elevated pressure both in the clinic and outside the clinic environment ().
Other measurements
Anthropometry
Height and weight are measured with a stadiometer to the nearest 0.1 cm and 0.1 kg respectively. Measurements are carried out with the shoes off, light clothing on, and no cap or headgear. However, in a case where an individual insists on wearing a headcover, a light head cover is allowed. The waist circumference is measured with a non-expansible tape without clothing or light clothing, in between the lower coastal margin and the iliac crest with the arm relaxed by the side. The waist circumference should be done preferably after an overnight fast but in the event where this is not feasible, the time of the last meal must be documented. Hip circumference is measured at the maximum width of the buttocks.
ECG
Trained fieldworkers obtained a 16 sec standard 12 lead ECG with a paperless Cardiax device (http://www.rdsm.eu/cardiax.html) interfaced with a computer. The digitally recorded ECG was printed both electronically and as hard copy using the Cardiax software, version 3.50.2 (RDSM, Hasselt, Belgium), for quality checks by trained cardiologists. Voltages and duration of ECG waves were measured to the nearest 0.1mv and 1 ms respectively. To improve ECG quality, fieldworkers were trained periodically on subject positioning, electrode placement and skin preparation. The cardiax software is embedded with a filter function with which low frequency noise emanating from movement, respiration, and baseline wander and high frequency noise emanating from power-line or radiated electromagnetic influence were filtered before the final signal acquisition. Cut-off values were set at 0.05 hz and 150 Hz for low and high frequency filters respectively; in accordance with the AHA recommendations [Citation16].
Biochemical examination
Biological samples are collected with the appropriate recipients for biochemical examination (glucose, lipids and creatinine in the blood; creatinine, protein in the urine) and are handled according to standard laboratory practice. Aliquot of serum and urine are store in −20 °C freezer in the designated tertiary hospital within the region and are transported later to the REMAH biobank at the University of Abuja Teaching Hospital.
Questionnaire
The fieldworkers administered a modified World Health Organization STEPS questionnaire to collect information on relevant medical history, alcohol and cigarette consumption, and intake of medications. Physical activity is assessed using the International Physical Activity Questionnaire [Citation17,Citation18]. Weight and height were measured with a weighing scale and stadiometer respectively and body mass index calculated as body weight in kilograms divided by height in meters squared. Diabetes mellitus was a self-reported diagnosis, use of anti-diabetic drugs or fasting or random plasma glucose equal to or exceeding 7.0 or 11.1 mmol/L.
Database management and statistical analysis
For database management and statistical analysis, we used SAS software version 9.4. (SAS Institute, Cary, NC). At the end of fieldwork in each community, the field supervisor sends in data in the form of questionnaire, ECG data and biological samples to the circulation laboratory or the biobank as the case may be. A statistician knowledgeable on SAS software coded the questionnaire and trained technicians keyed in all data in a password-protected computer while the paper forms are stored in a fireproof cabinet. ECG data are exported in XML format to an external device. Biological specimens are identified with a code that is made up of the unique identification number, the type of specimen and date of collection.
Data integrity
Duplicate datasets are compared with the PROC COMPARE procedure in SAS to detect input errors. We used means and standard deviation to express central tendency and spread of the data. We identified outliers and checked each variable so identified with the paper questionnaire. For comparison of means and proportions, we used Student’s t-test and the χ2 statistic, respectively. Statistical significance was a P-value less than 0.05 on two-sided tests.
Results
Characteristics of participants recruited from South-East Nigeria
Recruitment commenced on April 2017 at Anambra State, South-East Nigeria at the rural settlement of Awkuzu, Oyi Local Government Area and was followed by that of the urban community of Omagba, Onitsha North Local Government. Of the 556 (176 in Awkuzu and 380 in Omagba) invited to participate, 490 (176 in Awkuzu and 314 in Omagba) consented, giving a response rate of 100 and 86.4% for the rural and urban communities respectively. About 66.9% of participants in both rural and urban communities were women. Participants in rural area were older, thinner, smoked more cigarette and consumed more alcohol. Women were more obese and had significantly higher heart rates as compared to men in both rural and urban areas. Sustained hypertension in women of the rural (42.0% vs 31.6%) and urban (26.5% vs 25.6%) as well as the white-coat hypertension in the rural (22.0% vs 5.26%) and urban (16.2% vs 12.8) were apparently higher compared to men. However, masked hypertension showed tendency to be higher in males compared to females in both the rural (10.5% vs 6.0%) and urban (18.0% vs 13.2%) sites (). reports on the hemodynamic parameters of the participants according to sex and study site. Office systolic pressure (P<0.05) and diastolic pressure (P<0.05) were higher in women than men in rural site. Home systolic and diastolic pressure tended to be higher in rural women but reverse was the case of the latter in urban men.
Quality control of blood pressure readings
Out of a total of 4890 blood pressure readings (2445 each of systolic and diastolic readings) observed, only 39 (0.80%) ended in odd digits. Figure 3 shows the terminal digit preference of the BP observers. Terminal zero, two, four and six digits were recorded in 29.8%, 16.3%, 16.6% and 16.4 % respectively (P<0.0001) while terminal eight digit was recorded in 20.9 % of readings (P=0.06) ().
Table 1. Characteristics of participants by sex and study site.
Table 2. Haemodynamic characteristics by sex and study site.
Discussion
REMAH study is aimed at defining the true burden of hypertension in the most populous sub-Saharan African country. The aim of the current article is to provide the rationale and design of REMAH; demonstrate its feasibility and report on the quality of blood pressure measurement; the main phenotype of interest. To our knowledge, REMAH is the first nationwide survey on hypertension that will determine the prevalence of white-coat, masked and sustained hypertension in Nigeria. The recruitment and the data generated so far from the South East Nigeria indicate that REMAH is feasible and the result will be a valuable resource that will lay foundation for future research and policy formulation for control of hypertension.
In the past, public health attention in sub-Saharan Africa focused on communicable diseases. Emerging data [Citation19,Citation20] however, indicate that NCDs of which cardiovascular diseases are a major component; have become a main concern in this region of the world and may even overtake infectious diseases by the year 2030. On the premise that high blood pressure is the main driver of cardiovascular diseases (CVDs), addressing the epidemic of CVDs in sub- Saharan Africa must include screening for, treating of and research in hypertension as a top priority.
One of the major hindrances towards planning public health strategies to control the scourge of cardiovascular diseases is lack of standardized population based data. Few available reports on NCDs in Nigeria and most other low and middle-income countries are based either on hospital or non-standardized population data. Many factors challenge mounting standardized epidemiological study in low resource settings. They range from lack of adequate research infrastructure, poor funding and non-availability of demographic parameters. REMAH is being coordinated by the Circulation Health Research Laboratory of University of Abuja. The principal investigator received training at the Hypertension and Cardiovascular Epidemiology Unit of the University of Leuven. He was trained using the same methodologies employed to set up standardized cardiovascular epidemiological research in Europe [Citation21,Citation22], South America [Citation23] and China [Citation24]. Following his training, he established the Nigerian Population Research on Environment Gene and Health [Citation25] in a middle income housing estate at Lugbe Abuja Nigeria. REMAH, which is funded by the Tertiary Education Trust Fund, is aimed at expansion of the research work at Lugbe and it is designed to overcome some of the challenges encountered in the course of carrying out the NIPREGH project.
Although REMAH is a large-scale cross-sectional study, it is hoped that it will lay a foundation for future longitudinal study and as such, high quality blood pressure phenotype at the inception will ensure that future results are robust. Three criteria i.e. end-digit preference, percentage of identical readings and number of odd BP readings were used to ensure good quality of BP in REMAH study. The quality of BP phenotype reported in the first phase of REMAH is similar to that in previous standardized studies [Citation22,Citation23,Citation26,Citation27]. The ongoing Gaoyou Study [Citation26] in the Jiangsu Province of China is aimed at determining the clustering of risk factors associated with hypertension. The observers obtained three consecutive blood pressure measurements from randomly selected participants. Of the 26,898 BP readings, 17.2, 20.4, 20.3, 19.8 and 22.4% ended in a 0, 2, 4, 6 and 8 respectively. 67(0.03%) readings ended in an odd number. Similarly, in the GEnotipo, Fenotipo y Ambiente de la HiperTensión Arterial en UruguaY (GEFAHT-UY) study [Citation23], three trained observers measured BP five times consecutively at each of two home visits and one clinic visit. Only 21.6% of the SBP and DBP readings ended in 0 and the occurrence of odd readings ranged from 0.1% to 0.6%. The quality characteristics of the conventional BP recorded in the South East Nigeria in REMAH study was also similar to what was earlier reported in the Nigerian Population Research on the Environment Gene and Health (NIPREGH) study [Citation27]. Overall, REMAH met the quality standards reported in other surveys [Citation22,Citation23,Citation26,Citation27] and clinical trials [Citation28–30] in Nigeria [Citation27], Europe [Citation22,Citation28], China [Citation26], and Uruguay [Citation23]. However, the quality standards in REMAH is obviously higher than what was reported in a clinical practice setting in Nigeria. Ayodele et al. [Citation31] evaluated zero end digit preference in blood pressure recording among 383 patients attending a hypertension specialist clinic in Ogbomosho, South-West Nigeria. The zero end-digit preference was very common as 98.7 and 57.7% of blood pressure measurements by nurses and doctors respectively ended with a zero digit.
Including out-of-office blood pressure measurement in REMAH is in line with the current ESH/ESC Hypertension Guideline [Citation32]. The guideline recommends that diagnosis of hypertension should be based on repeated office BP measurement or out of office BP measurement with ABPM and/or HBPM if logistically and economically feasible. For hypertensive patients, self-monitoring of blood pressure not only helps to discover masked uncontrolled hypertension, it also improves control of blood pressure to target level [Citation33]. Many validated monitors for self-measurement of BP is affordable and are easy to operate as demonstrated by many illiterate REMAH study participants in the rural community of South-East Nigeria. Furthermore, future research may aim at use of SIM (subscriber identity module) card enabled blood pressure monitors that can transmit blood pressure readings from remote rural sites to central servers through which hypertension experts can assist local health care providers or laypersons in providing care to people living with hypertension.
Conclusion
We have demonstrated that REMAH is feasible and that a high quality standard is maintained in measurement of blood pressure, the main phenotype of interest. REMAH is therefore poised to provide a valuable data that will inform policies targeted at control of hypertension, the greatest contributor to the global disease burden.
Acknowledgements
The authors gratefully acknowledge the support of the following traditional and community leaders in whose respective communities REMAH fieldwork is taking place 1. Chief George Echesi, the President General, Awkuzu Progressive Union; 2. Ven Isreal Odita, the Archdeacon, Omagba Archdeaconry (Anglican Communion) Onitsha; 3. His Royal Highness (HRH) Monday Udoewah, the Clan Head of Ubium Clan, Nsit Ubium LGA, Akwaibom State; 4. Mr. Habila N. Garba, District Head of Ture, Ture District Office, Kaltungo Chiefdom, Kaltungo LGA, Gombe State; 5. Alhaji Adamu Musa, Chairman Shongo Housing Estate Residents Association (SHERA) Gombe State; 6. HRH Alhaji Attahiru Bungudu, Emir of Bungudu, Zamfara State. Mrs. Maureen Amaechi provided valuable administrative and clerical support to REMAH project.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Gakidou E, Afshin A, Abajobir AA, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1345–1422.
- Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–450.
- Ataklte F, Erqou S, Kaptoge S, et al. Burden of undiagnosed hypertension in sub-Saharan Africa. A systematic review and meta-analysis. Hypertension. 2015;65:291–298.
- Akinlua JT, Meakin R, Umar AM, et al. Current prevalence pattern of hypertension in Nigeria: a systematic review. Plos One. 2015;10:e0140021
- Adeloye D, Basquill C, Aderemi AV, et al. An estimate of the prevalence of hypertension in Nigeria: a systematic review and meta-analysis. J Hypertens. 2015;33:230–242.
- Ogah OS, Okpechi I, Chukwuonye II, et al. Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. WJC. 2012;4:327–340.
- Akinkugbe OO. Non-Communicable Diseases in Nigeria: Final Report of a National Survey. Series 4. Lagos; 1997.
- Franklin SS, O’Brien E, Thijs L, et al. Masked hypertension: a phenomenon of measurement. Hypertension. 2015;65:16–20.
- Odili AN, Thijs L, Hara A, et al. Prevalence and determinants of masked hypertension among black nigerians compared with a reference population. Hypertension. 2016;67:1249–1255.
- Stergiou GS, Asayama K, Thijs L, et al. Prognosis of white-coat and masked hypertension: International Database of HOme blood pressure in relation to Cardiovascular Outcome. Hypertension. 2014;63:675–682.
- ICFMacro NPCNNa. Nigeria Demographic and Health Survey 2008. Abuja, Nigeria. National Population Commission and ICF Macro; 2013.
- Assembly sWM. Declaration of Helsinki: recommendations guiding physicians in biomedical research involving human subjects. Bull Pan Am Health Organ. 1990;24:606–609.
- Sims JM. A brief review of the Belmont report. Dimens Crit Care Nurs. 2010;29:173–174.
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–2219.
- El Assaad MA, Topouchian JA, Asmar RG. Evaluation of two devices for self-measurement of blood pressure according to the international protocol: the Omron M5-I and the Omron 705IT. Blood Press Monit. 2003;8:127–133.
- Kligfield P, Gettes LS, Bailey JJ, et al. Recommendations for the standardization and interpretation of the electrocardiogram. Part I: the electrocardiogram and its technology. A scientific statement from the American Heart Associatione Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorese by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2007;49:1109–1127.
- Oyeyemi AL, Oyeyemi AY, Adegoke BO, et al. The Short International Physical Activity Questionnaire: cross-cultural adaptation, validation and reliability of the Hausa language version in Nigeria. BMC Med Res Methodol. 2011;11:156.
- Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395.
- Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002-2030. Ann Trop Med Parasitol. 2006;100:481–499.
- Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442
- Jin Y, Kuznetsova T, Tikhonoff V, et al. Left ventricular structure in relation to the human SAH gene in the European Project on Genes in Hypertension. Hypertens Res. 2009;32:145–151.
- Kuznetsova T, Staessen JA, Kawecka-Jaszcz K, et al. Quality control of the blood pressure phenotype in the European Project on Genes in Hypertension. Blood Press Monit. 2002;7:215–224.
- Luzardo L, Sottolano M, Lujambio I, et al. Quality of the blood pressure phenotype in the GEnotipo, Fenotipo y Ambiente de la hipertension arterial en UruguaY (GEFA-HT-UY) study. Blood Press Monit. 2014;19:339–345.
- Zhang L, Li Y, Wei FF, et al. Strategies for classifying patients based on office, home, and ambulatory blood pressure measurement. Hypertension. 2015;65:1258–1265.
- Odili AN, Ogedengbe JO, Nwegbu M, et al. Nigerian Population Research on Environment, Gene and Health (NIPREGH) — objectives and protocol. J Biomed Res. 2014;28:360–367.
- Lu YC, Li SS, Zhang HF, et al. Quality control of the blood pressure phenotype in the Gaoyou population study. Blood Press. 2016;25:162–168.
- Odili AN, Ameh VO, Ogedengbe J, et al. Quality of blood pressure phenotype in the Nigerian populaion research on environment gene and health. Blood Press Monit. 2014;19:220–225.
- Wingfield D, Cooke J, Thijs L, et al. Terminal digit preference in the Syst-Eur trial. Blood Press Monit. 2002;7:169–178.
- Canner PJ, Borhani NO, Oberman A, et al. The Hypertension Prevention Trial: assessment of the quality of blood pressure measurements. Am J Epidemiol. 1991;134:379–392.
- Dischinger P, DuChene A. Quality control aspects of blood pressure measurements in the Multiple Risk Factor Interventional. Trial Contr Clin Trials. 1986;7:137–57S.
- Ayodele OE, Sanya EO, Okunola OO, et al. End digit preference in blood pressure measurement in a hypertension specialty clinic in southwest Nigeria. Cardiovasc J Afr. 2012;23:85–89.
- Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104.
- Bray EP, Holder R, Mant J, et al. Does self-monitoring reduce blood pressure? Meta-analysis with meta-regression of randomized controlled trials. Ann Med. 2010;42:371–386.