
ABSTRACT
While there is a growing body of research suggesting that care leavers experience disadvantages in early adulthood. There is only one study at hand, that use panel data to analyze long term effects. Based on this idea, we examine data from the German Socio-Economic Panel (SOEP), covering a 50-year period, and use matching methods to compare care leavers who have been in residential care or lived with foster parents to a control group. The results indicate that being placed in out-of-home care is associated with disadvantages in terms of unemployment, life satisfaction and health. The results regarding satisfaction with leisure vary, and no clear picture emerges here. Differences in health are more relevant in late adulthood. Differences between residential care leavers and their peers are more stable over time than differences between former foster children and their peers.
Introduction
Inequalities that persist and deepen over a person’s life course often begin with early adult transitions into tertiary education, vocational training and paid employment. Young people with a challenging and disadvantaged family background are at particularly high risk of social exclusion (Stein & Munro, Citation2008). “Social exclusion” primarily refers to a delay in the transition to centralized social systems or the inability to make this transition without social support.
Some of these young people have been taken from their families and have grown up in out-of-home care. The most common reasons for children being taken into care in Germany are neglect, excessive demands on parents and physical and psychological abuse (Gerber, Citation2015). Young people who have been placed in foster families or residential care facilities are referred to as “looked-after children” or “children in care.” Their transition from adolescence to adulthood takes place in the context of leaving state care and moving on to independent living (Pinkerton, Citation2012). However, it is also possible that some youth move back to their families. A growing body of international research has revealed the poor outcomes for adults who experienced out-of-home care, foster care and/or residential care, as children, also known as care leavers. Compared to people who were not in care as children, care leavers are much more likely to have poorer educational qualifications, be homeless and suffer from mental health problems and unemployment (Sacker et al., Citation2021; Stein & Munro, Citation2008; Zeira et al., Citation2023).
Young people who have experienced out-of-home care are disadvantaged in several respects. Even when other factors are empirically controlled for, out-of-home care is a predictor of disadvantage in terms of unemployment, life satisfaction and satisfaction with leisure and health. However, many studies only examine care leavers relatively shortly after they have left care. An exception is the study by Zeira et al. (Citation2023), which uses propensity score matching to follow care leavers from 2000 to 2015. Their results show disadvantages in educational attainment for care leavers in comparison to their peers.
The existing research does show, however, that the disadvantages care leavers face in the course of their lives are very different to what other young adults experience. Young people leaving care usually experience “accelerated and compressed” transitions to independence, as in most countries they cannot routinely remain in residential or foster care beyond the age of 18 (sometimes 21). Even though residential care and foster care are very different, there are no differences between the forms of care with regard to transitions into adult life (Ehlke, Citation2020). These young people have also had to overcome adversities (e.g. abuse and neglect) in their early childhood before coming into care, and they cannot necessarily rely on their birth family or previous carers for ongoing emotional or financial support in adulthood (Jackson & Höjer, Citation2013). Finally, transitions to stable and secure employment are particularly challenging, as the educational attainment of young people in care is lower than that of their peers in the general population (Bryderup & Trentel, Citation2013; Jackson & Cameron, Citation2012). Due to these multiple disadvantages, care leavers are at high risk of social exclusion and poor outcomes throughout their lives (Stein & Munro, Citation2008).
However, the group of care leavers is not homogeneous. Stein (Citation2006) distinguishes between three types of care leavers. The first group comprises those “moving on” successfully. They had stability in their out-of-home care and “they have made sense of their family relationships so they could psychologically move on from them” (Stein, Citation2006, p. 277). They have graduated from school or are still attending school. The second group, the survivors, were more affected by instability and disruption during their time in care. They often have no education history and experience problems after leaving care, including periods of homelessness. The third group, the victims, had bad experiences in their families and were unable to compensate for these experiences while in care. They have problems at school and are often homeless and unemployed after leaving care. Notwithstanding these differences, care leavers as a whole are at a disadvantage compared to young people who have not experienced out-of-home care. More recent research emphasizes these findings and comes to similar conclusions (Muir et al., Citation2019). Mental health problems appear to correlate with higher rates of unemployment and financial difficulties (Eurochild, Citation2010; Muir et al., Citation2019). International comparative studies (Berlin et al., Citation2021; Cameron et al., Citation2018) have found that care leavers have lower educational qualifications and a higher risk of unemployment, with one third of care leavers, on average, not in employment. This is probably related to the fact that mainstream schools are not prepared for dealing with the special needs of children in care (Groinig et al., Citation2019; Strahl, Citation2020) and do not recognize the psychological burden they experience during the transition to working life (Atkinson & Hyde, Citation2019). The lack of support for care leavers in higher education is another reason why they often fail to reach their goals. They also lack social capital because they tend to have fewer relationships, networks and friendships outside of residential care (Göbel et al., Citation2021; Pluto et al., Citation2020; Törrönen, Citation2021).
In a recent study by Sacker et al. (Citation2021), census data from the Office for National Statistics (ONS) Longitudinal Study (England and Wales) were analyzed to examine the long-term effects of having been in care. The authors compared people who had been in residential and foster care as children with those who had grown up in parental homes up to 40 years later. Cared for children are economically disadvantaged in middle adulthood and into old age. “The need for public expenditure on health and welfare benefits such as the NHS, Universal Credit and Housing Benefit will be a life-long reality for many care leavers, coupled with a lower contribution to the public purse” (Sacker et al., Citation2021, p. 3). The type of care arrangement also plays a role: kinship care achieved the best results, followed by foster care, while residential care had the worst outcomes.
This article addresses two issues. The first is whether the inequalities faced by cared for children will persist in different stages of their lives. Like Sacker et al. (Citation2021), we examine three different cohorts (young, middle and late adulthood). In contrast to Sacker et al. (Citation2021), we use data from a German panel and a more sophisticated methodological approach to control for socio-economic differences, as we know that out-of-home care is related to family background. The second issue is whether these inequalities are dependent on the specific out-of-home care setting, i.e. residential or foster care.
Research Question
As mentioned in the section above, there is little knowledge about the later lives of people who were in care as children. According to the capability approach (Nussbaum, Citation2011), child and youth services should not focus on human capital (Otto, Citation2015; Robeyns, Citation2005a, Citation2005b), but on ensuring that young people have a good life. To measure the “effects” of out-of-home care, it is therefore necessary to take into account not only employment rates, but also life satisfaction and health.
It could also be argued, from a methodological perspective, that a comparison group of children who were not in care is necessary. Growing up in care is not a random factor. It is related to belonging to ethnic minorities, growing up in a single-parent family and/or being financially and socially disadvantaged (Eurochild, Citation2010; Jarczok et al., Citation2021; Tabel, Citation2020). It has also been argued that there is a “need for more outcome research, especially using more experimental and quasi-experimental designs” (Stein, Citation2006, p. 278). For ethical reasons, however, experiments cannot be conducted in this area. It is not possible to randomly place children in out-of-home care or not, as this would mean endangering their welfare in the name of science. To address this criticism, we will simulate an experiment using propensity score matching (Austin, Citation2011; Harris & Horst, Citation2016; Randolph et al., Citation2014; Rosenbaum & Rubin, Citation1983) and answer the following question:
1. At different stages of their lives, are there differences between adults who have been in out-of-home care (residential or foster care) as children, compared to a control group who have never lived in care, in terms of
current health status
satisfaction with leisure
being unemployed
current life satisfaction?
Method
To our knowledge, there are no data on out-of-home care and care leaving that cover a period of more than 50 years (Ahmed et al., Citation2021; Erzberger et al., Citation2019). However, in the German Socio-Economic Panel (SOEP) (Liebig et al., Citation2021) there is one question available in the “BIOL” dataset (the abbreviation has no special meaning) that asks: “How many years of your childhood (up to the age of 15) did you live with the following persons?” The answer options include both parents, one parent, or one parent plus a new partner, in various combinations. Growing up with other relatives is another possible answer. In line with our research question, we were interested in the answers “with foster parents” and “in residential care.”
The SOEP is a representative multi-cohort survey, which has been conducted since 1984. Every year, individuals in households are asked to provide information on topics such as unemployment, health, life satisfaction, etc. Sometimes additional samples are drawn or new variables are added to the survey, and not every variable is reported every year. For our analysis we use SOEP v38, which includes data from 1984 to 2021. Some (but not all) individuals participated in SOEP at multiple measurement points (Liebig et al., Citation2021). In this case our approach was similar to that of Sacker et al. (Citation2021), who used the ONS Longitudinal Study, also a representative multi-cohort survey.
In addition to the question of residential and foster care, we were interested in current health status, satisfaction with leisure, being unemployed and overall life satisfaction. This information is contained in the “PL” dataset.
Current health is measured via the question “How would you describe your current state of health?.” The answer options range from very good (1) to bad (5). This invites a subjective description of the respondent’s own state of health.
The answers to “How satisfied are you today with the following areas of your life?” – “With your leisure time?” range from 0 “completely dissatisfied” to 10 “completely satisfied.”
To measure the respondent’s current unemployment status, the questionnaire asks “Are you currently registered unemployed with the unemployment office?.”
Finally, current life satisfaction is measured via the question “How satisfied are you with your life, all things considered?,” with possible options ranging from 0 “low satisfaction” to 10 “high satisfaction.”Footnote1
These variables are only measured with single items. In order to take this and fluctuations in the responses into account, for example because a respondent was particularly satisfied or dissatisfied with their life at the time of the survey, we also calculated mean values for the corresponding variables over several measurement points. A sum score was calculated for being unemployed, by adding the number of periods of unemployment during the period in which the respondents took part in the SOEP. Control variables for the propensity score matching (see next section) are considered in the BIOL dataset. The PPATHL dataset was used for information on gender and migration background.
Preparing Propensity Score Matching and Missing Values
When all available data from 1984 to 2021 are considered, 663 participants stated that they had lived in residential care and 348 that they had lived with foster parents.Footnote2 Participants older than 70 years were excluded from our analysis because most of them had lived in care during or even before the Second World War. After these exclusions, 552 participants who had lived in residential care and 253 who had lived with foster parents remained in our sample. On average, 7.7 years (SD 5.4) were spent with foster parents and 5.4 years (SD 4.5) in residential care. 69 participants have lived with foster parents as well as in residential care. These participants contributed to both the foster care findings and the residential care findings. In Germany, people who have lived in care at some point in their childhood make up around two per cent of the population. Comparing the group who had once lived in care with the sample of 78,125 (we exclude all participants how are older than 70 years) who had never lived in care seemed to be an “unfair” comparison. As mentioned before, living in out-of-home care is correlated with social background variables (Jarczok et al., Citation2021; Schmidt et al., Citation2002; Tabel, Citation2020). On the other hand, having over 78,000 individuals as a control group was a great opportunity to conduct propensity score matching (Austin, Citation2011; Harris & Horst, Citation2016; Randolph et al., Citation2014). In propensity score matching, each participant in the treatment group (in this case, those who have been in care) is matched with a participant from the control group (those who have never been in care) based on selected variables. As matching variables we used sex (male – femaleFootnote3), year of birth (1915–2003 | M: 1972 | SD: 16), migration background (no migration background, indirect migration background if father or mother had a migration background, direct migration background if the respondent was born in a country other than Germany), place of childhood (1= large city, 2= medium-sized city, 3= small town, 4= countryside), father’s school-leaving qualification (1= no qualification, 2= lowest track (Hauptschule), 3= medium track (Realschule), 4= highest track (Gymnasium)), mother’s school-leaving qualification (see father). Since trend analyses are calculated with different age groups, we also considered when the respondents had first participated in the survey (1984–2021; M: 2008; SD 11), the number of times they had done so (1–38; M: 7 SD: 7), and their age when they had last participated (M: 42; SD 13.29).
The calculation of propensity score matching requires a dataset without missing values (Austin, Citation2011; Harris & Horst, Citation2016; Randolph et al., Citation2014). Missing values in the SOEP can be attributed not only to non-response, but also to the study design of the SOEP: that is, the same questions were not asked at all measurement points. The items about the father’s and mother’s school-leaving qualifications have missing values, although these two items seem very relevant (see ). Around one third of the participants answered that they did not know their parents’ school leaving-qualifications (see Results). There are also missing values for the dependent variables.
Table 1. Missing values for variables considered in propensity score matching and for dependent variables.
Imputation Before Matching
First, we tested whether the missing data for the variables of school-leaving qualification (father and mother), leisure satisfaction and life satisfaction could be assumed to be missing at random, taking into account the entire data (if we only carry out the analysis with participants in foster and residential care there are no significant correlations). The analysis shows that missing values for parents’ school-leaving qualifications are linked with migration history. Missing values concerning satisfaction with leisure are also correlated with migration history. However, the correlations here can be considered small (r < .3). For the other variables, there are statistically significant but not meaningful (r < .1) correlations due to the large sample size. To use van Buuren’s concept (Citation2019), the data is not missing completely at random (MCAR), but lies somewhere between missing at random (MAR) and missing not at random (MNAR).
In the case of propensity score matching, it is also recommended to impute missing data. Here we followed the recommendations of Ling et al. (Citation2020) and Pishgar et al. (Citation2021). For the imputation, all the variables used in the propensity score matching and the subsequent t-tests were included. Predictive mean matching in the MICE (multiple imputation by chained equations) package in R was used for imputation. Ten imputed datasets were generated (van Buuren & Groothuis-Oudshoorn, Citation2011). The later following analysis runs ten times and we report the average across the 10 analyses.
Results of Propensity Score Matching
After the imputation we ran the propensity score matching using the R package MatchThem, which is based on MatchIt (Ho et al., Citation2022; Randolph et al., Citation2014) and provides a tool for matching with multiply imputed datasets (Pishgar et al., Citation2021). The nearest-neighbor procedure was used for the propensity score matching.
The quality of the propensity score matching was very good for both cases (residential and foster care). The standardized mean difference should be as close as possible to 0, but values greater than .1 are also acceptable. The variance ratio should be around 1 and the Kolmogorov-Smirnov statistics should be close to 0. The row distance indicates the absolute difference between the propensity scores of pairs of of each treated and control unit. presents the results before and after matching. As can be seen here, the results for the matching are very good apart from the first participation in the SOEP. The standardized mean difference and Kolmogorov-Smirnov statistics are close to .0 and the variance ratio is close to 1.0. Compared to the differences before matching, a clear equalization of the observed values can be seen. The analysis for the propensity score matching with foster care also shows good results. Here too, the first participation in SOEP is different after matching ().
Table 2. Propensity score matching results for residential care.
Table 3. Propensity score matching results for foster parents.
Trend Analysis
In line with the aim of our research, i.e. to analyze trends among adults who were placed in out-of-home care as children, our next step was to form three groups to reflect different life stages: 19–29 years, 30–49 years, and 50–69 years. Each person was assigned to a life phase; there is therefore no overlap between the groups. We formed these groups based on the difference between the date of the respondents’ last participation in the survey and their year of birth. It should be noted that the groups come from different birth cohorts. Even after imputation and propensity score matching the n’s between adults who experienced residential care as children and the control groups could differ, as there are still small differences in the variables first participation in the survey, number of participations and age at last participation. This means that people can be assigned to different age cohorts (for example, if one person took part in the survey for the last time at the age of 29 - but the “nearest neighbor” was 30).
However, forming different age groups enabled the number of cases to be kept sufficiently high. To calculate t-tests, the treatment group (residential or foster care) was compared with the control group (never in out-of-home care). Cohen’s d was calculated to determine the strength of the differences. Here we adhered to the general guidelines of small (0.2), medium (0.5) and large (0.8) when interpreting an effect (Cohen, Citation1988). Since we have calculated numerous t-tests, there is a possibility of an inflation of the alpha error (type I error false positive). One possibility to deal with that issue is to set a more conservative significance level (e.g. Holm, Citation1979), but this increases the possibility of type II errors (false negative) (Menyhart et al., Citation2021). There are various methods of dealing with multiple hypothesis testing. The best known are Bonferroni corrections and corresponding adjustments (e.g. Hochberg, Citation1988; Holm, Citation1979). A more recent approach to problems with multiple significance testing was introduced by Benjamini and Hochberg (Citation1995) and later adapted (Benjamini & Hochberg, Citation2000), the False Discovery Rate (FDR). In an article on different methods for alpha-level errors in multiple testing, Menyhart et al. (Citation2021) propose the FDR approach for confirmatory analysis (as in this paper). In this paper, an FDR error rate of 5% was set and the Benjamini-Hochberg adjusted p-values (Benjamini & Hochberg, Citation2000) are shown in the table. Applying the FDR correction separately for the analysis for adults who experienced residential care as children and adults who experienced foster care as children shows that the prior p-value threshold is .025 for analyses regarding residential care and .010 for analyses regarding foster care.
Results
In the following analysis, we have used the data after the propensity score matching. Placement in a foster family or a residential care facility appears to depend partly on background factors. Girls are more likely to be placed in foster care (56%), while boys are more likely to be placed in residential care (53%). Around one tenth of people who were in care as children were born outside Germany (residential care 13% | foster care 12%). Nine per cent of parents of adults who experienced residential care, as children were not born in Germany, while this applies to 6% of the parents of adults who experienced foster care, as children. Nine per cent of the mothers and 5% of the fathers of children who grow up in care have no school-leaving qualifications. Furthermore, a substantial number of the participants who have grown up in care do not know what qualifications their parents have (residential care: mother 27% | father 37%; foster care: mother 32% | father 39%). On average, the participants in the residential care group took part in the SOEP 6.52 times (SD: 5.93) and the participants in the foster care group 5.91 times (SD: 5.30).
Residential Care
Firstly, we were interested in whether there were differences when comparing adults who experienced residential care, as children with those not living in residential care (Control Group (CG)). We began by examining cases between the ages of 19 and 69, then looked at different age groups in the following analysis (18–29 | 30–49 | 50–69). With the exception of the most recently collected data on satisfaction with leisure, we found a significantly higher level of disadvantage among those formerly accommodated in residential care. Adults who experienced residential care, as children reported a poorer state of health, both at the current time of measurement (: residential care M: 2.79 vs. CG M: 2.49 p < .001) and in terms of average state of health (: residential care M: 2.69 vs. CG M: 2.34 p < .001). There were also statistically significant differences in life satisfaction in both calculated variants. Overall, the previously institutionalized children were more likely to state that they had been unemployed in the course of their lives (residential care M: 1.38 vs. CG M: .68 p < .001). In terms of effect size, the differences in the areas of health, life satisfaction and unemployment can be rated as small.
Table 4. Differences between adults who experienced residential care, as children and control group, ages 19 to 69.
Residential Care, As Children; Ages 19 to 29
In the subsequent analysis, we used the propensity score data and divided the dataset into three age groups. The first group had left care only a few years ago. They were between 19 and 29 years old (mean: 24 years). The results showed significant differences in terms of health, life satisfaction and unemployment, with worse outcomes for adults who experienced residential care, as children. Looking at the effect sizes (Cohen’s d), these differences can be interpreted as small to medium. Former care leavers also differed from the control group in terms of average satisfaction with leisure (: residential care: 6.69 vs. CG: 7.21 p < .001), but this difference was not observed when looking at current satisfaction with leisure (: residential care: 7.04 vs. CG: 6.94 p = .778).
Table 5. Differences between adults who experienced residential care, as children and control group, ages 19 to 29.
Residential Care, Ages 30 to 49
The next age group we analyzed was between 30 and 49 years old (mean age: 40). There are still differences in unemployment (: residential care: 1.66 vs. CG: .82). Former children in care are also more dissatisfied with their lives overall. This finding is confirmed both for average life satisfaction and when the last measurement point is taken into account. In the cases of health and satisfaction with leisure, a significant difference can be found only for the averaged measurement. Here, the differences in the last available measurement are no longer statistically significant (: residential care: 2.55 vs. CG: 2.37 p = .073), but there is still a statistically significant difference in the average value (: residential care: 2.67 vs. CG: 2.46 p = .024)
Table 6. Differences between adults who experienced residential care, as children and control group, ages 30 to 49.
Residential Care, Ages 50 to 69
The last group we looked at participated in the SOEP between the ages of 50 and 69 (mean age: 59). In this, the oldest of the groups analyzed, the differences in health between adults who experienced residential care, as children and the control group are again statistically significant, both for the last available measurement (: residential care: 2.91 vs. CG: 2.52 p < .001) and for the values averaged over several measurement points (: residential care: 3.04 vs. CG: 2.76 p < .001). There are also differences in life satisfaction between the two measurement methods. Unemployment continues to be a risk in the oldest group, affecting those who were in residential care as children significantly more often than those who were not (: residential care: 1.37 vs. CG: .71 p = .004).
Table 7. Differences between adults who experienced residential care, as children and control group, ages 50 to 69.
Residential Care: Differences Over a Lifetime
To better illustrate how differences between adults who experienced residential care, as children and the control group develop over the course of a lifetime, we have plotted the mean scores in two figures. The first figure shows the differences in health and unemployment, the second the differences in leisure and life satisfaction.
The differences in health between previously institutionalized children and the control group already exist at a young age (18 to 29 years). However, these differences become smaller in middle age bracket, as can be seen from the effect size (). Moreover, differences in health measured at a certain point in time are no longer statistically significant. Between the ages of 50 and 69, however, the measured differences in health increase again. Overall, it can be seen that health in both groups deteriorates over the course of a lifetime ().
Figure 1. Mean differences between adults who experienced residential care, as children and control group over their lifetime (health and unemployment).
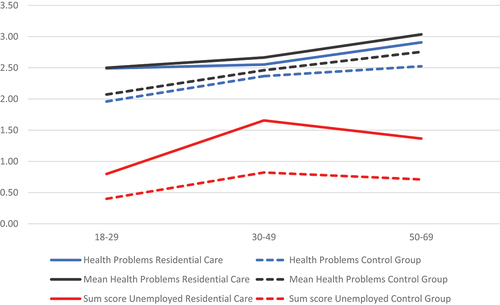
In terms of satisfaction with leisure, our results do not show a clear picture. Regardless of age, there are measurable differences when we focus on the average value of satisfaction with leisure, but not when we look only at the last measurement point. This is the case in all three age groups analyzed. Over time, a decline can be observed in both groups in the middle stage of life and a subsequent increase for the 50 to 69 age range.
General life satisfaction provides clearer results: even at a young age, care leavers differ from their peers. These differences appear to persist over time, but at a slightly lower level, and continue to exist into old age. This is primarily due to an increase in the life satisfaction of care leavers in the 30 to 49 age group (). Former children in care are much more likely to be affected by unemployment over the course of their lives than their peers ().
Figure 2. Mean differences between residential care leavers and control group over their lifetime (leisure and life satisfaction).

Foster Care
The calculations in this analysis were carried out for adults who had been placed with foster parents during their childhood. Here too, three life stages were considered.
First, we investigated whether there were differences between adults who experienced foster care, as children and the control group across all age brackets. The results showed a significant difference in health regardless of which definition was considered (mean p = .003 or individual measurement time p = .002). With regard to satisfaction with leisure, the results showed no significant differences (p > .05 for both single measurement and mean measurement). In terms of life satisfaction, respondents who had grown up with foster parents differed from the control group. The results also showed that those who had grown up in foster families were more frequently affected by unemployment (: foster care: .96 vs. CG: .44 p = .002).
Table 8. Differences between adults who experienced foster care, as children and control group, ages 19 to 69.
Foster Care, Ages 18 to 29
In the 18 to 29 age range (mean age: 23), differences in terms of health status, leisure, life satisfaction and unemployment are not significant (). It is important to take into account the small number of cases when interpreting the results. For health, life satisfaction and unemployment, the effect size is above Cohen’s d > .3 and the small number of cases could be a reason why the results are not significant in a statistical interpretation.
Table 9. Differences between adults who experienced foster care, as children and control group, ages 19 to 29.
Foster Care, Ages 30 to 49
In the next age cohort (30 to 49), respondents were on average 40 years old. Compared to the group that did not grow up in out-of-home care, differences can only be seen in the probability of being unemployed (: foster care: 1.26 vs. CG: .49 p = .008). The analysis showed no significant differences in terms of health status, satisfaction with leisure or life satisfaction.
Table 10. Differences between adults who experienced foster care, as children and control group, ages 30 to 49.
Foster Care, Ages 50 to 69
Finally, we analyzed the group of 50- to 69-year-olds, with an average age of 60. What is striking here are the differences in health status, to the disadvantage of those who grew up with foster parents (: health problems: foster care: 3 vs. CG: 2.68 p = .018 | mean health problems: foster care: 3.12 vs. CG: 2.84 p = .015). The analysis showed no differences with regard to satisfaction with leisure. However, we did find a difference between adults who experienced foster care, as children and the control group with regard to life satisfaction, measured at the last measurement point (: foster care: 6.95 vs. CG: 7.43 p = .046). These findings should be treated with caution, as the adjusted p-value calculated to account for multiple testing is not significant (see section 3.4). In this sense, there are no differences between adults who experienced foster care as children and the control group at the age between 50 and 69.
Table 11. Differences between adults who experienced foster care, as children and control group, ages 50 to 69.
Foster Care: Differences Over a Lifetime
As in our analysis of adults who grew up in residential care, we also present the results for former foster children over their lifetimes (). If we look at the overall trend, we can see that the differences in health only become significant between the ages of 50 and 69 (however, not if the adjusted p-value is taken into account, but a tendence can still be recognized – adjusted p ~ .6). Both, the foster group and the control group rate their own health as worse between the ages of 50 and 69 (). Respondents who grew up with foster parents are more likely to be unemployed in the 30 to 49 age range than their peers in the control group (). However, the difference disappears in the highest age group, and unemployment decreases among adults who experienced foster care, as children compared to the 30 to 49 age group.
Figure 3. Mean differences between adults who experienced foster care, as children and control group over their lifetime (health and unemployment).
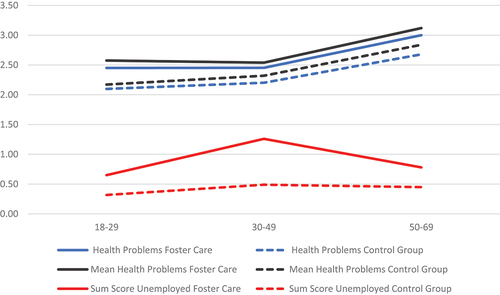
Figure 4. Mean differences between adults who experienced foster care, as children and control group over their lifetime (health and unemployment).
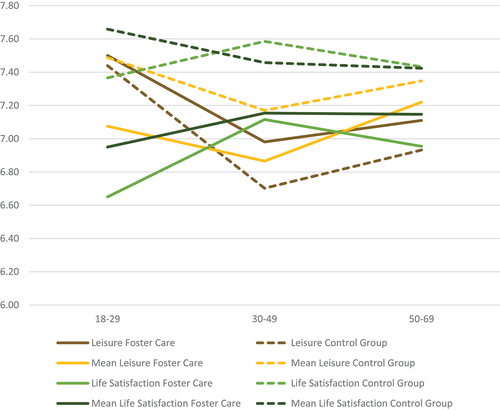
With regard to leisure, there are no differences between adults who experienced foster care, as children and the control group. As already shown in , satisfaction with leisure decreases in middle age bracket and increases again in old age bracket (). The analysis also found no differences in life satisfaction. However, the trend here depends on the measurement. If only the last measurement point is used, life satisfaction peaks in the 30 to 49 age group before falling again slightly. In the 50 to 69 age group, there is no significant difference (adjusted p-value) between respondents who grew up with foster parents and the control group (). If the mean value is used, however, a slight decrease can be assumed in the control group, while the foster care group shows a slight increase between the 18 to 29 and 30 to 49 age groups. However, there are no significant differences between the two groups.
Discussion and Limitations
With the exception of Sacker et al. (Citation2021), this study is one of the first attempts to consider different life stages of care leavers and compare them to a control group. We used data from an official socio-economic panel for the trend analysis. Using propensity score matching, we compared young people who had experienced out-of-home care (foster care and residential care) with their peers at the ages of 18 to 29, 30 to 49 and 50 to 69. In order to obtain more stable and reliable results, we calculated the last available value for health, satisfaction with health and life satisfaction, as well as an average value of all data over time. We also took into account the number of periods of unemployment the respondents had experienced.
The results show that growing up in permanent or temporary residential care has an impact on work, health and wellbeing. The only area where differences are not consistently discernible – and should therefore be interpreted with caution – is satisfaction with leisure. People who grew up in residential care have health-related disadvantages as young adults aged 18 to 29. These differences decrease in the middle age bracket but then increase again in the older age bracket, when health problems increase anyway. Residential care leavers are also generally more dissatisfied with their lives and more often unemployed. It can therefore be assumed that the disadvantage is lifelong and persistent.
The results look different when we consider the group who grew up with foster parents. In post-adolescence (ages 18 to 29) there are no differences between these young people and their peers. However, the number of participants at this stage is fairly small, so the results may be underestimated in a statistical way and should therefore be treated with caution. In the middle age bracket (30–49) those raised by foster parents are more likely to be unemployed, and in the old age bracket (50–69) they are more likely to complain about their health. However, when looking at the adjusted p-value in late adulthood, the results show no differences between adults who experienced foster care as children and the control group, but a trendence can still be seen.
Nevertheless, the risk of social exclusion (see Stein & Munro, Citation2008) remains stable from early adulthood (18–29) to middle adulthood (30–49) in terms of unemployment rates and life satisfaction and even health, which are more significant in late adulthood (50–69). The differences in satisfaction with leisure must be interpreted with caution, as the results depend on how this satisfaction was measured. The disadvantages are more pronounced for youth growing up in residential care.
The results of existing research on care leavers are often limited to the period immediately after leaving care and focus on their accelerated transition to adulthood. The inequalities that have previously been identified (Berlin et al., Citation2021; Cameron et al., Citation2018; Eurochild, Citation2010; Muir et al., Citation2019) persist in the later stages of life, as our research and that of Sacker et al. (Citation2021) show. The topic of integration into the labor market is particularly relevant in this respect. The challenges that care leavers face when integrating into the labor market decrease as they get older. However, employment is an ongoing challenge for care leavers, and not just in young adulthood. Other research supports the hypothesis that our results can be explained by lower rates of educational attainment (Bryderup & Trentel, Citation2013; Jackson & Cameron, Citation2012) and by schools or universities not providing enough support for children living in or leaving care (Groinig et al., Citation2019; Kliche & Täubig, Citation2019; Townsend et al., Citation2023). Köngeter et al. (Citation2016) point out the lack of support for care leavers in educational institutions. Young people in care receive less support to complete school, which probably explains their lower employment rates, and more ideas are needed to support care leavers in education throughout their life course. The question is whether child and youth welfare and other support systems are working well together to address this issue. Courtney and Hook (Citation2017) show that simply extending the length of time children spend in foster care can have an impact on employment. At the same time, schools and teachers need to be better prepared for the special situation of children in care.
There are differences between the two forms of out-of-home care that we looked at in our analysis. The disadvantages are more obvious for youth growing up in residential care. Statistically, however, it should not be concluded that foster care is preferable to residential care. A comparison of the two groups is not straightforward, since the background variables (e.g. migration background, parents’ schooling) are not the same in both groups. In other words, it is not a matter of chance whether someone is growing up with foster parents or in residential care. Further research is needed on this question, looking more closely at the actual setting of residential and foster care. It should be noted that both types of care have diversified and now take many different forms.
Bearing in mind these points, we can nonetheless observe that people who have lived in foster care are disadvantaged in only two of the four aspects considered: they are more likely to be unemployed in middle adulthood and they report more health problems in late adulthood. In contrast, those who grew up in residential care experience the same disadvantages but also report lower life satisfaction than their peers.
More recent studies emphasize the importance of contextual factors such as country characteristics (Park et al., Citation2022). Previous studies have focused heavily on individual factors and policies, but we do not know much about the meso-level, i.e. that of the organization or country. In the middle age bracket (ages 30 to 49), adults who have lived either in residential care or with foster parents are disadvantaged in terms of unemployment. Our results support the findings of Sacker et al. (Citation2021), who found evidence that foster care has better long-term outcomes (i.e. in middle and late adulthood) than residential care. A key reason for this, as pointed out by Mendes et al. (Citation2023), is that care leavers from institutions receive the least ongoing support.Footnote4 However, countries differ in the organization of care and in the effects of different forms of care. Mendes et al. (Citation2023) are referring to Australia, and Sacker et al. (Citation2021) to England and Wales. In this context, changes in the care system over time – changes whose desirable and undesirable consequences only become noticeable later – must also be taken into account. However, socio-economic and ecological circumstances can also influence the results. In our results, the 50 to 69 age group is less affected by unemployment, which may also be due to the different economic circumstances in which they grew up (that is, there may be more jobs available for low-skilled workers). In this context, it should also be mentioned that we calculate sum scores for the unemployment outcomes. Participants who complete the questionnaire more frequently may have a higher unemployment score. However, due to the propensity score matching, the differences in participation rates between adults who experienced foster care and/or residential care as children and the control group are likely to be rather small.
Further studies are needed to assess the effects of growing up in public care more fully and to capture the different dimensions of inequality. While aspects such as the transition to the labor market and/or vocational education are important in early adulthood, differences in health tend to occur later in life. We therefore need research examining a period of at least 30 years, but it is almost impossible to find data for such a long period of time. In both residential and foster care, political and pedagogical changes in the out-of-home care system were only observed after a relatively long period of time. It could be that young people living in care today see the relevant issues differently. Until further data are available, a better understanding of the long-term effects of out-of-home care can only be gained using secondary data analysis or retrospective studies.
Our analysis is based on SOEP data. Using secondary data is a cost-effective and time-saving way to gain more insight into the long-term effects of out-of-home care, but the method has its limitations. SOEP is a large study with different foci, and children in care were obviously not at the center of the panel’s design. We were therefore only able to control for sociodemographic characteristics in the analysis and had no further information about the reasons why the respondents had been in care. Factors that lead to or are related to out-of-home placement, such as problem behaviors, aggression and clinical acuity, were not taken into account. We tried to map the socio-economic background via the parents’ level of education.
There is also no information about the residential care facilities the respondents had lived in or about the quality of the care provided. In order to maintain a sufficient sample size, different arrangements and lengths of time spent in out-of-home care were not taken into account. In addition, the socio-economic panels collect data on very different aspects of life. They therefore often rely on single items, which do not have the same validity as psychometric scales. To deal with this problem, we calculate mean scores over time, considering several measurement points, and compare these results with those produced when only the last measurement point is considered. Finally, our results are based on panel analysis, not longitudinal studies of individual development.
Our research is also innovative from a methodological point of view. Comparing children in care with all of their peers is not appropriate. We therefore used propensity score matching to obtain a similar control group based on socio-demographic variables. From a professional point of view, however, it is necessary to ask what the goals of residential care are; this also raises the methodological question of the “right” control group. Should residential care enable a life comparable to that of peers from similar backgrounds, who are usually disadvantaged, or should it be oriented toward a typical middle-class socialization and corresponding life course?
Disclosure statement
No potential conflict of interest was reported by the author(s).
Notes
1. We use the translation of the questions from https://paneldata.org/.
2. It should be noted here that, contrary to other countries in Germany, the proportion of cases in residential care is on average more than twice as high as in foster care. Residential care and foster care are different forms of assistance in Germany. But unlike in the USA, the form of care is not directly related to the level of support provided to young people.
3. The option “other” is only available in more recent versions of the SOEP, so we have to use a dichotomous form.
4. In 2021, Social Code Book VIII – Child and Youth Welfare responded to this gap and introduced a mandatory form of “aftercare.” However, nationwide implementation has not yet been completed.
References
- Ahmed, S., Rein, A., & Schaffner, D. (2021). Ökosystem Heim als entkoppelte Welt: Perspektiven von Care Leavern auf den Sozialisationskontext Heim. Gesellschaft – Individuum – Sozialisation Zeitschrift Für Sozialisationsforschung, 2(2). https://doi.org/10.26043/GISo.2021.2.1
- Atkinson, C., & Hyde, R. (2019). Care leavers’ views about transition: A literature review. Journal of Children’s Services, 14(1), 42–58. https://doi.org/10.1108/JCS-05-2018-0013
- Austin, P. C. (2011). An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behavioral Research, 46(3), 399–424. https://doi.org/10.1080/00273171.2011.568786
- Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B (Methodological), 57(1), S. 289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
- Benjamini, Y., & Hochberg, Y. (2000). On the adaptive control of the false discovery rate in multiple testing with Independent statistics. Journal of Educational and Behavioral Statistics, 25(1), S. 60–83. https://doi.org/10.2307/1165312
- Berlin, M., Kääriälä, A., Lausten, M., Andersson, G., & Brännström, L. (2021). Long‐term NEET among young adults with experience of out‐of‐home care: A comparative study of three Nordic countries. International Journal of Social Welfare, 30(3), 266–279. https://doi.org/10.1111/ijsw.12463
- Bryderup, I., & Trentel, M. Q. (2013). The importance of social relationships for young people from a public care background. European Journal of Social Work, 16(1), 37–54. https://doi.org/10.1080/13691457.2012.749219
- Cameron, C., Hollingworth, K., Schoon, I., van Santen, E., Schröer, W., Ristikari, T., Heino, T., & Pekkarinen, E. (2018). Care leavers in early adulthood: How do they fare in Britain. Finland and Germany? Children and Youth Services Review, 87, 163–172. https://doi.org/10.1016/j.childyouth.2018.02.031
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed). L. Erlbaum Associates.
- Courtney, M. E., & Hook, J. (2017). The potential educational benefits of extending foster care to young adults: Findings from a natural experiment. Children and Youth Services Review, 72, 124–132. https://doi.org/10.1016/j.childyouth.2016.09.030
- Ehlke, C. (2020). Care Leaver aus Pflegefamilien: die Bewältigung des Übergangs aus der Vollzeitpflege in ein eigenverantwortliches Leben aus Sicht der jungen Menschen. Beltz Juventa.
- Erzberger, C., Herz, A., Koch, J., & Lips, A., van Santen, E., Schröer, W., & Seckinger, M., (Eds.), (2019). Sozialstatistische Grundlage sozialer Teilhabe von Care Leaver*innen in Deutschland: Datenreport auf der Basis der Erziehungshilfeforschung und repräsentativer Paneluntersuchungen. https://doi.org/10.18442/068
- Eurochild. (2010). Children in alternative care national surveys (2nd ed).
- Gerber, C. (2015). Krisenintervention und Inobhutnahme. In J. Merchel Ed., Handbuch Allgemeiner Sozialer Dienst (ASD).(2., aktual. und erw. Aufl. ed. pp. 257–267). Reinhardt.
- Göbel, S., Hadjar, A., Karl, U., & Jäger, J. A. (2021). Agency and the school-to-work transition of care leavers: A retrospective study of Luxembourgish young people. Children and Youth Services Review, 122, 105636. https://doi.org/10.1016/j.childyouth.2020.105636
- Groinig, M., Hagleitner, W., Maran, T., & Sting, S. (2019). Bildung als Perspektive für Care Leaver? Bildungschancen und Bildungswege junger Erwachsener mit Kinder- und Jugendhilfeerfahrung. In Schriftenreihe der ÖFEB-Sektion Sozialpädagogik (1st ed., Vol. 4). Verlag Barbara Budrich.
- Harris, H., & Horst, S. J. (2016). A brief guide to decisions at each step of the propensity score matching process. Advance online publication. https://doi.org/10.7275/yq7r-4820
- Hochberg, Y. (1988). A sharper Bonferroni procedure for multiple tests of significance. Biometrika, 75(4), 800–802. https://doi.org/10.1093/biomet/75.4.800
- Ho, D. E., Imai, K., King, G., & Stuart, E. A. (2022). Matching as nonparametric preprocessing for reducing model dependence in parametric causal inference. 3. https://doi.org/10.1093/pan/mpl013
- Holm, S. (1979). A simple sequentially rejective multiple test procedure. Scandinavian Journal of Statistics, 6(2), S. 65–70.
- Jackson, S., & Cameron, C. (2012). Leaving care: Looking ahead and aiming higher. Children and Youth Services Review, 6(6), 1107–1114. https://doi.org/10.1016/j.childyouth.2012.01.041
- Jackson, S., & Höjer, I. (2013). Prioritising education for children looked after away from home. European Journal of Social Work, 1(16), 1–5. https://doi.org/10.1080/13691457.2012.763108
- Jarczok, M., Knecht Krüger, B., Mitrovic, T., Gérard, G., & Jud, A. (2021). Care leaver needs and accessibility: Findings from the first large‐scale project in Switzerland. Child & Family Social Work, 26(1), 11–25. https://doi.org/10.1111/cfs.12785
- Kliche, H., & Täubig, V. (2019). Begleitung schulischer Übergänge in Wohngruppen der Kinder- und Jugendhilfe. Soziale Passagen, 11(1), 47–63. https://doi.org/10.1007/s12592-019-00321-5
- Köngeter, S., Schröer, W., & Zeller, M. (2016). The drawback of getting by—implicit imbalances in the educational support of young people in and leaving care in Germany. In P. Mendes & P. Snow (Eds.), Young people transitioning from out-of-home care: International research, policy and practice (1. Aufl., p. 173–196). Palgrave Macmillan UK; Palgrave Macmillan.
- Liebig, S., Goebel, J., Schröder, C., Grabka, M., Richter, D., Schupp, J., Bartels, C., Fedorets, A., Franken, A., Jacobsen, J., Kara, S., Krause, P., Kröger, H., Metzing, M., Nebelin, J., Schacht, D., Schmelzer, P., Schmitt, C., & Schnitzlein, D. (2021). Deutsches Institut für Wirtschaftsforschung. Sozio-oekonomisches Panel, Daten der Jahre 1984–2019 (SOEP-Core, v36). https://doi.org/10.5684/SOEP.V36
- Ling, A., Montez-Rath, M., Mathur, M., Kapphahn, K., & Desai, M. (2020). How to apply multiple imputation in propensity score matching with partially observed confounders: A simulation study and practical recommendations. Journal of Modern Applied Statistical Methods, 19(1), Artikel jmasm.eP3439. https://doi.org/10.22237/jmasm/1608552120
- Mendes, P., Bollinger, J., & Flynn, C. (2023). Young people transitioning from residential out-of-home care in Australia: The case for extended care. Residential Treatment for Children & Youth, 40(3), 348–362. https://doi.org/10.1080/0886571X.2022.2139330
- Mendes, P., & Snow, P. (2016). Young people transitioning from out-of-home care: International Research, policy and practice (1st ed.). Palgrave Macmillan UK: Palgrave Macmillan.
- Menyhart, O., Weltz, B., Győrffy, B., & Delcea, C. (2021). MultipleTesting.com: A tool for life science researchers for multiple hypothesis testing correction. Public Library of Science One, 16(6), e0245824. https://doi.org/10.1371/journal.pone.0245824
- Muir, S., Purtell, J., Hand, K., & Carroll, M. (2019). Beyond 18: The longitudinal study on leaving care wave 3 research report: Outcomes for young people leaving care in Victoria. Australian Institute of Family Studies.
- Nussbaum, M. C. (2011). Creating capabilities: The human development approach. Belknap Press of Harvard University Press.
- Otto, H. U. (Ed.). (2015). Technical and vocational education and training: Volume 20. facing trajectories from school to work: Towards a capability-friendly youth policy in Europe.
- Park, S. E., Okpych, N. J., Harty, J. S., & Courtney, M. E. (2022). County-level factors matter: The role of contextual factors in foster youths’ extended foster care participation and human capital outcomes. Child Maltreatment. https://doi.org/10.1177/10775595221088226
- Pinkerton, J. (2012). Understanding young people’s transitions from state care: The need for connections. Diskurs Kindheits- und Jugendforschung, 3(7), 309–319.
- Pishgar, F., Greifer, N., Leyrat, C., & Stuart, E. (2021). Match Them: Matching and weighting after multiple imputation. The R Journal, 13(2), 228. https://doi.org/10.32614/RJ-2021-073
- Pluto, L., Schrapper, C., & Schröer, W. (2020). Was bewegt die Forschung zur Heimerziehung: Stand und Perspektiven: ein Positionspapier im Rahmen der Initiative, Zukunftsforum Heimerziehung“ Wissenschaftliche Dokumentation. IGFH – Internationale Gesellschaft für erzieherische Hilfen.
- Randolph, J. J., Falbe, K., Manuel, A. K., & Balloun, J. L. (2014). A step-byStep guide to propensity score matching in R Practical Assessment, Research & Evaluation. 18
- Robeyns, I. (2005a). The capability approach: A theoretical survey. Journal of Human Development, 6(1), 93–117. https://doi.org/10.1080/146498805200034266
- Robeyns, I. (2005b). Selecting capabilities for quality of life measurement. Social Indicators Research, 74(1), 191–215. https://doi.org/10.1007/s11205-005-6524-1
- Rosenbaum, P. R., & Rubin, D. R. (1983). The central role of the propensity score in observational studies for causal effects Biometrika. Biometrika, 70(1), 41–55. https://doi.org/10.1093/biomet/70.1.41
- Sacker, A., Murray, E., Lacey, R., & Maughan, B. (2021). The lifelong health and wellbeing trajectories of people who have been in care: Findings from the looked-after children grown up project the LACGro project. Nuffield Trust. https://doi.org/10.13140/RG.2.2.14371.58403
- Schmidt, S., Hohm, P., Macsenaere, & Petermann. (2002). Effekte erzieherischer Hilfen und ihre Hintergründe. In Schriftenreihe des Bundesministeriums für Familie, Senioren, Frauen und Jugend. (Vol. 219).
- Stein, M. (2006). Research review: Young people leaving care. Child and Family Social Work, 11(3), 273–279. https://doi.org/10.1111/j.1365-2206.2006.00439.x
- Stein, M., & Munro, E. R. (Eds.). (2008). Young people’s transitions from care to adulthood: International research and practice. Jessica Kingsley Publishers.
- Strahl, B. (2020). Heimerziehungsforschung in Deutschland: Eine Expertise für das „Zukunftsforum Heimerziehung“ Expertise. IGFH - Internationale Gesellschaft für erzieherische Hilfen.
- Tabel, A. (2020). Empirische Standortbestimmung der Heimerziehung: Fachwissenschaftliche Analyse von Daten der amtlichen Kinder- und Jugendhilfestatistik: im Rahmen der Initiative, Zukunsftsforum Heimerziehung“. Expertise. IGFH-Eigenverlag.
- Törrönen, M. (2021). Social relationships and their connection to mental health for young people who have been in the care system. The British Journal of Social Work, 51(3), 927–944. https://doi.org/10.1093/bjsw/bcab028
- Townsend, I. M., Reupert, A. E., & Berger, E. P. (2023). Educators’ experiences of an Australian education program for students in out-of-home care. Child & Youth Services, 44(2), 168–193. https://doi.org/10.1080/0145935X.2022.2046461
- van Buuren, S. (2019). Flexible imputation of missing data (2nd ed.). Chapman and Hall/CRC Interdisciplinary Statistics Ser. CRC Press LLC. https://ebookcentral.proquest.com/lib/kxp/detail.action?docID=5455460
- van Buuren, S., & Groothuis-Oudshoorn, K. (2011). Mice multivariate imputation by chained equations in R. Journal of Statistical Software, 45(3). https://doi.org/10.18637/jss.v045.i03
- Zeira, A., Achdut, N., & Benbenishty, R. (2023). Predicting educational attainments and enrollment to higher education: A longitudinal study of care leavers in Israel. Research in Higher Education, 64(8), 1165–1190. https://doi.org/10.1007/s11162-023-09742-x