
Abstract
Background
The prevalence and severity of perimenopausal symptoms are typically associated with multiple factors, including demographic characteristics. The sociodemographic characteristics of women living in rural areas differ from those residing in urban areas, and it has been suggested that these differences could potentially influence the prevalence of symptoms experienced during perimenopause.
Objectives
To evaluate if perimenopausal women living in Spanish rural areas have a higher prevalence of perimenopausal symptoms and assess their influence on health-related quality of life.
Methods
A cross-sectional study was conducted in a sample of 270 perimenopausal women residing in rural and urban areas. The participants completed the Cervantes Scale Short Version and Beck Depression Inventory 2.
Results
Perimenopausal women in rural areas reported a higher incidence of perimenopausal symptoms and a lower perception of health-related quality of life compared to those in urban areas, as evidenced by higher scores on the total Cervantes Scale Short Version scale (33.2 (±16.2) vs. 26.4 (±18.1), p = .001). No differences in the Beck Depression Inventory 2 score were detected.
Conclusions
Perimenopausal women residing in rural areas of Spain reported a higher prevalence of perimenopausal symptoms and experienced a poorer Health-Related Quality of Life compared to those living in urban areas of Spain.
Introduction
The hormonal changes that occur around menopause are typically accompanied by various clinical manifestations. These changes have been extensively described and systematized by the Stages of Reproductive Aging Workshop (STRAW-10). In particular, the period preceding menopause is referred to as the menopausal transition and consists of two stages: early (Stage −1) and late (Stage −2), and the twelve months following the last menstrual period are called the early postmenopausal stage (Stage +1). The period of time covering the transition to menopause and early postmenopause constitutes the perimenopause stage [Citation1,Citation2]. Perimenopause is currently recognized as a transitional period in a woman’s life, characterized by physiological, affective, psychological, and social changes. For many women, these changes can significantly impact their Health-Related Quality of Life (HRQoL) and self-esteem. However, the prevalence and severity of perimenopausal symptoms can vary and are typically associated with multiple factors, including physiological aspects, reproductive history, physical condition, and demographic characteristics [Citation3].
The sociodemographic characteristics of women in rural areas differ from those residing in urban areas. In this regard, it is well-established that women residing in rural areas encounter numerous obstacles that render them more vulnerable and additionally, research has highlighted that exposure to various endocrine disruptors may vary between women in urban and rural areas [Citation4–6]. Consequently, it has been suggested that these differences could potentially influence the prevalence of symptoms experienced during perimenopause. However, there is a limited number of studies comparing perimenopausal symptom and HRQoL in rural and urban women, and the results are contradictory. One study reported more intense climacteric symptoms in Mexican perimenopausal women living in urban areas [Citation7], while other studies reported more vasomotor and urogenital problems in midlife Indian women dwelling in rural areas [Citation8]. Moreover, findings indicated that a permanent place of residence in the country was an independent predictor of poorer quality of life in midlife (peri and pos-menopausal) Polish women [Citation9].
In this regard, there is not data on the prevalence of perimenopausal symptoms in Spanish rural women and the possible differences in HRQoL between perimenopausal women dwelling in rural and urban areas. Our study aims to evaluate HRQoL in perimenopausal women living in Spanish rural areas and compare it with those living in urban areas.
Materials and methods
A cross-sectional study was conducted between December 2019 and April 2023. Women from eight Autonomous Communities of Spain were invited to participate in the study through letters addressed to various women’s associations. Additionally, they were approached in person during routine health checkups with their primary care physicians or during gynecological cancer prevention consultations. Inclusion in the study was based on providing consent and meeting the following criteria: being between 45 and 55 years of age, experiencing increased variability in menstrual cycle length greater than 7 days in consecutive cycles, or having amenorrhea lasting 60 days or more but less than 1 year (according to clinical criteria of stages −1, −2 and +1, STRAW-10). The following exclusion criteria were applied: the presence of chronic diseases, mental disorders, or physical disability; history of radiotherapy or cytostatic treatment; previous bilateral oophorectomy or hysterectomy; current use or recent (within 3 months) history of menopausal hormone treatment or estrogen therapy; experiencing a significant negative life event or family process within the last 2 years; and having changed their place of residence within the last 10 years.
Health-related quality of life
HRQoL was evaluated with the Short Version of the Cervantes Scale (C-SF). The C-SF is a self-administered questionnaire consisting of 16 items specifically designed to evaluate the impact of menopause on various domains. These domains include menopause and health, and the subdomains of vasomotor symptoms, overall health, aging, psychic, sexuality, and couple relationships. The C-SF can be utilized by both women with and without partners, through the use of a correction factor. In terms of scoring, menopause and health, as well as psychic, are considered negative domains, meaning that a score of 0 indicates the best state, while a score of 5 indicates the poorest state. In contrast, sexuality and relationships are positive domains where 0 indicates the poorest state and 5 indicates the best state. The instrument has been shown to have good psychometric properties, including good predictive criterion validity [Citation10,Citation11]. Moreover, in some studies, each item of the scale has been categorized into 3 levels, both for the menopause and health and psychological domains (low impairment = 0–1, moderate impairment = 2–3, and high impairment = 4–5) and for the sexuality and relationship domains (low impairment= 4–5, moderate impairment= 2–3 and high impairment = 0–1) [Citation12].
Depressive symptom level
The Beck Depression Inventory 2 (BDI-2) was employed to evaluate depressive symptom level. This is a self-administered questionnaire that assesses depressive symptoms within the two weeks prior to its completion, including the nine depressive symptoms outlined in DSM-IV. The questionnaire consists of 21 items that are rated on a Likert scale, yielding a total score between 0 and 63. Higher scores are compatible with a diagnosis of depression. Standard cutoff points are used to classify the scores into 4 groups, where scores of 10 or lower are considered normal and scores above 10 are compatible with a certain degree of depression, ranging from mild to severe. The BDI-2 has been validated for the Spanish population and has been used to assess HRQoL and depressive symptoms in women during the transition to menopause and postmenopause [Citation13,Citation14].
Statistical study and sample size calculation
The characteristics of the sample were described using various statistical measures. Categorical variables were presented as absolute values and percentages, while quantitative variables were expressed as means and standard deviations. We used the Kolmogorov-Smirnow test to check for the normality of the distribution in the different groups. The Chi-square test was used for the comparison of categorical variables. If the data were normally distributed, the mean scores on the tests were compared using Student’s t-test, whereas the Wilcoxon rank-sum test was used for non-normally distributed data. Levene’s test was used to evaluate the homogeneity of variances. Finally, Linear regression analysis was used to identify independent variables that could potentially affect HRQoL. All analyses were conducted using the SPSS statistical package (SPSS for Windows, 17.0; SPSS Inc.) and the level of statistical significance was set at a value of p < .05.
The sample size was calculated using the ENE 2.0 statistical program [Citation15] for the comparison of two means. One hundred and thirty-five in women were included in each arm of the study, providing a power of 90% to detect a difference of 6.7 points in the total C-SF score. This is the minimum difference considered to indicate that the woman perceives a change in her health status. This assumption is based on a mean value of the total C-SF score of 38.10 (SD ± 16.9) revealed by a bilateral T-Student test with a significance level of 5% [Citation11,Citation16].
Ethical considerations
The study was approved by the Research Ethics Committee of the Principality of Asturias, ref: 272/19 and the women gave their consent to participate in the study, with data storage complying with GDPR regulations.
Results
Two hundred and eighty-nine women, aged between 45 and 55 years, from 8 Autonomous Communities of Spain were invited to participate in the study. These women met the main clinical criteria of perimenopause based on their menstrual cycle, as defined by STRAW-10. All participants completed the C-SF and BDI-2 questionnaires. Nineteen women (6.5%) provided incorrect, non-valid data or did not answer all the items in the questionnaires and were subsequently excluded. The remaining 270 women were included in the study. Of the sample, 135 women had resided during the last 10 years in population centers considered to be rural because they had a population density of ≤ 2000 inhabitants. The remaining 135 women resided in urban centers with a population density exceeding 2000 inhabitants. Within this urban group, 70 lived in centers with a population between 2000 and 100,000 inhabitants, while 65 women resided in metropolises with more than 100,000 inhabitants.
The sociodemographic and clinical characteristics of both populations are shown in . In the urban sample, a higher number of women reported consuming alcohol. However, within this group, 32.6% reported occasional alcohol consumption, 11.9% drank less than 3 units per week, and only 6.7% drank 3 or more units per week. The percentage of women in the rural population sample who reported drinking 3 or more units of alcohol per week was similar, at 4.4%. Regarding sexual activity, a higher percentage of women reported being sexually active compared to those in urban areas (96.3% in rural areas vs. 87.4% in urban areas, p = .008). Sexual activity was defined as engaging in sexual intercourse, masturbation, or caressing on a regular or sporadic basis, with either a heterosexual or homosexual partner.
Table 1. Sociodemographic and clinical characteristics of the sample.
Health-related quality of life
Perimenopausal women residing in rural areas showed a poorer perception of health-related quality of life, as indicated by the total C-SF score, compared to those in urban areas. The mean values for total C-SF and for the different domains and subdomains are shown in . Women in rural areas scored significantly higher than their urban counterparts in the domains of menopause and health, and psychological state, as well as in the subdomains of vasomotor symptoms, health, and aging. However, no statistically significant differences were observed in the domains of sexuality and couple relationships.
Table 2. Health-related quality of life according to the short cervantes scale administered to women living in rural and urban areas.
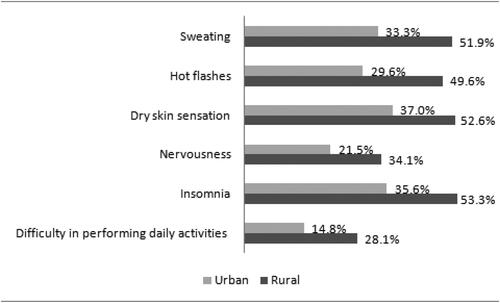
When analyzing the scores indicating moderate or high affectation (score ≥ 3) in various items of the scale where differences were found between women living in rural and urban areas, several observations were made. Women in rural areas, in addition to experiencing a higher incidence of hot flashes (OR 1.67; 95% CI 1.22–2.28), also reported a higher incidence of sweating (OR 1.55; 95% CI 1.16–2.07), insomnia (OR 1.50; 95% CI 1.13–1.97), nervousness (OR 1.58; 95% CI 1.06–2.36), difficulty in performing daily activities (OR 1.46; 95% CI 1.05–2.03) and a sensation of dry skin (OR 1.42; 95% CI 1.08–11.86) ().
Figure 1. Percentage of women with scores producing moderate or high impairment (score ≥ 3) on the various C-SF items.
Notes: Percentage of women with scores producing moderate or high affectation (score ≥ 3) in the different items of the C-SF: Sweating, p = 0.002, hot flushes, p = 0.001, dry skin, p = 0.01, nervousness, p = 0.003, insomnia p = 0.003, difficulties in performing daily tasks p = 0.008. Chi-square test
Depressive symptom level
When analyzing the BDI-2 scores, the rural and urban groups did not differ in terms of the percentage of women who scored above the diagnostic limit compatible with some form of depression (28.1% vs. 25.9%, p = .681).
In addition to rural residency, other factors related to the C-SF total score in the total sample included the presence or absence of some level of depression (46.7 ± 13.5 vs 23.8 ± 15.8, p < .001), age older or younger than 50 years (32.2 ± 17.1 vs 27.8 ± 17.6, p = .027), presence or absence of obesity (37.4 ± 19.9 vs 28.1 ± 16.4, p = .002), presence or absence of physical activity (27.1 ± 16.9 vs 33.8 ± 18.3, p = .001), and the presence or absence of sexual activity (28.6 ± 16.9 vs 43.7 ± 18.6, p < .001). The bivariate analysis comparing the overall C-SF scores in the rural and urban populations is shown in .
Table 3. Overall health-related quality of life score in rural and urban women.
A linear regression model including age, sexual activity, rural or urban residence, and presence or absence of depression level, yielded an R2 = 0.4087, p < .001. In this model, the presence of depression symptoms explains an average increment of 21.6 points in the C-SF total score, while the absence of sexual activity and residing in a rural area exert a comparable influence, accounting for an average increase of 8.3 points and 6.9 points, respectively, in the C-SF total score.
Discussion
Perimenopause is a variable stage of women’s lives that typically begins around 2–8 years before menopause and continues up to 12 months after the last menstrual period. During this period, most women experience physical and psychological changes associated with fluctuations in estrogen levels, which can have an impact on HRQoL.
Moreover, various sociocultural factors may influence how individual women perceive perimenopausal symptom and our study found that residing in a rural area exerts a negative impact on HRQoL. These findings align with results from previous studies conducted among Indian, Turkish, Polish and Peruvian perimenopausal/postmenopausal women [Citation17–20]. However, our data differ from a previous study carried out in a sample of perimenopausal women residing in Mexico City, which reported more intense climacteric symptoms than indigenous Zapotec-speaking women dwelling in a rural area, but the authors of that study suggest that this difference may be influenced by cultural factors [Citation7]. Our findings also differ from results that did not detect significant differences in QoL between Indian postmenopausal women living in rural and urban areas [Citation21], and partially differ from another study among a sample of Spanish postmenopausal women. That study reported a greater frequency of menopausal symptoms in urban women, while rural women experienced more hot flushes although rural women experienced more hot flushes, depression, joint pain and tingling, albeit with less severity than urban women [Citation22]. However, it is important to note that one of these studies was conducted among peri- and postmenopausal women, while the other did not include perimenopausal women.
It is now widely recognized that the diagnosis of perimenopause should be based on symptoms and signs rather than hormone levels, as the latter can be inaccurate due to their variability [Citation3,Citation23]. Thus, based on the STRAW + 10 model, the characteristics of the menstrual cycle are the main criteria for identifying this stage, with hormonal biomarkers being used only as supporting criteria. In our study, the sample was selected from women presenting changes in the menstrual cycle according to stages −2, −1, and +1 of the STRAW + 10 criteria. These individuals had been residing in population centers with a population density of ≤ 2000 inhabitants for the past decade. Therefore, our sample is a robust representation of women in the perimenopausal stage residing in rural areas across multiples autonomous communities of Spain.
In our study, the mean values of the total C-SF fell within the range considered normal for women of that age group based on normative C-SF scales derived from the Spanish population [Citation16]. Vasomotor symptoms are the most common reason for medical consultation during perimenopause and represent a clinical scenario that may lead to an increase in the number of medical consultations, and this poses a particular challenge in rural areas where access to medical services is often more limited. Some studies have even reported hot flash prevalence rates as high as 80 to 85% across all menopausal stages [Citation24,Citation25]. In our study, the overall prevalence of hot flashes was 70% among the total sample but reached 80% in rural women.
In our sample, obese women obtained a worse overall mean C-SF total score compared to non-obese women, consistent with the results of the SWAM study [Citation26]. Furthermore, our data align with the prevalence of depressive symptoms among perimenopausal women as reported in another study [Citation27] and they reveal no significant differences between perimenopausal women in rural and urban settings, which is in line with findings from other studies [Citation28,Citation29].
Our study has certain limitations. Firstly, it is a cross-sectional study, and the data were collected primarily from self-reports, which suggests that the findings should be interpreted with caution. Secondly, some questionnaires were completed amidst the backdrop of the COVID-19 pandemic, a period characterized by heightened stress levels, particularly evident in urban areas. Lastly, our sample was confined to participants from 8 Autonomous Communities, potentially limiting the generalizability of our findings to other geographic regions.
In light of these considerations, we believe that our findings are of interest to health authorities responsible for tackling the depopulation of rural areas. In particular, our study provides valuable insights that can inform healthcare planning specifically tailored to women in rural areas, highlights the prevalence of depression symptoms during perimenopause and their impact on the HRQoL as well as the negative influence of rural residency on HRQoL.
Conclusions
Perimenopausal women residing in rural areas of Spain reported a higher prevalence of perimenopausal symptoms and experienced a poorer Health-Related Quality of Life compared to those living in urban areas of Spain.
Disclosure statement
The authors declare no conflicts of interest.
Additional information
Funding
References
- Harlow SD, Gass M, Hall JE, et al. Executive summary of the stages of reproductive aging workshop + 10: addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012;97(4):1–6. doi: 10.1210/jc.2011-3362.
- Ambikairajah A, Walsh E, Cherbuin N. A review of menopause nomenclature. Reprod Health. 2022;19(1):29. doi: 10.1186/s12978-022-01336-7.
- Santoro N, Roeca C, Peters BA, et al. The menopause transition: signs, symptoms, and management options. J Clin Endocrinol Metab. 2021;106(1):1–15. doi: 10.1210/clinem/dgaa764.
- Połtyn-Zaradna K, Zatońska K, Basiak A, et al. Sociodemographic characteristic of changes in smoking patterns in rural and Urban population of PURE Poland study: findings from 6-year follow up. BMC Public Health. 2019;19(1):6. doi: 10.1186/s12889-018-6354-0.
- Bogar S, Ganos E, Hoormann K, et al. Raising rural women’s voices: from self-silencing to self-expression. J Women Aging. 2017;29(6):515–529. doi: 10.1080/08952841.2016.1256732.
- Carli F, Tait S, Busani L, et al. Exposure to endocrine disruptors (di(2-Ethylhexyl)phthalate (DEHP) and bisphenol A (BPA)) in women from different residing areas in Italy: data from the LIFE PERSUADED project. Int J Mol Sci. 2022;23(24):16012. doi: 10.3390/ijms232416012.
- Carranza-Lira S, Flores-Miranda MA, Gómez-Brigada I. [Comparison of climacteric syndrome symptoms among perimenopausal women from Mexico city and one zapotec community of Oaxaca, Mexico]. Ginecol Obstet Mex. 2010;78(2):116–120.
- Dasgupta D, Ray S. Vasomotor and urogenital problems at midlife: a study on rural and urban women in India. Ann Hum Biol. 2015;42(3):268–275.
- Żołnierczuk-Kieliszek D, Kulik TB, Jarosz MJ, et al. Quality of life in peri- and post-menopausal polish women living in lublin province–differences between urban and rural dwellers. Ann Agric Environ Med. 2012;19(1):129–133.
- Coronado PJ, Borrego RS, Palacios S, et al. Structural validity of a 16-item abridged version of the cervantes health-related quality of life scale for menopause: the cervantes Short-Form scale. Menopause. 2015;22(3):325–336. doi: 10.1097/GME.0000000000000321.
- Coronado PJ, Monroy M, Fasero M, et al. Predictive and criterion validity of the Cervantes-SF menopause quality of life questionnaire. Menopause. 2021;28(8):935–942. doi: 10.1097/GME.0000000000001790.
- Fasero M, Hernández A, Varillas-Delgado D, et al. Women with low quality of life by cervantes-short form scale choose menopausal hormone therapy. Eur J Obstet Gynecol Reprod Biol. 2020;252:43–49. doi: 10.1016/j.ejogrb.2020.06.019.
- De la Rosa-Cáceres A, Stasik-O’Brien S, Rojas AJ, et al. Spanish adaptation of the inventory of depression and anxiety symptoms (IDAS-II) and a study of its psychometric properties. J Affect Disord. 2020;271:81–90. doi: 10.1016/j.jad.2020.03.187.
- Gibbs Z, Lee S, Kulkarni J. Factors associated with depression during the perimenopausal transition. Womens Health Issues. 2013;23(5):e301-307–e307. doi: 10.1016/j.whi.2013.07.001.
- Busquets LB, Marino AP. Cálculo del tamaño muestral (TM) con el programa Ene 2.0: manual del programa, documentación y ejemplos [Internet]. Gráficas Monterreina; 2005. https://books.google.es/books?id=1j1INQAACAAJ.
- Coronado PJ, Monroy M, Fasero M, et al. Population-based norms for the Cervantes-SF short-form questionnaire assessing health-related quality of life in menopause. Maturitas. 2021;146:34–41. doi: 10.1016/j.maturitas.2021.01.004.
- Sharma S, Mahajan N. Menopausal symptoms and its effect on quality of life in urban versus rural women: a cross-sectional study. J Midlife Health. 2015;6(1):16–20. doi: 10.4103/0976-7800.153606.
- Taşkıran G, Özgül S. Individual characteristics associated with menopausal symptom severity and menopause-Specific quality of life: a rural perspective. Reprod Sci. 2021;28(9):2661–2671. doi: 10.1007/s43032-021-00545-y.
- Kaczmarek M, Pacholska-Bogalska J, Kwaśniewski W, et al. The association between socioeconomic status and health-related quality of life among Polish postmenopausal women from urban and rural communities. Homo. 2017;68(1):42–50. doi: 10.1016/j.jchb.2016.11.004.
- Beas R, Díaz-Pardavé C, Arriola-Montenegro J, et al. Severity of climacteric symptoms among Peruvian women from an urban coastal community and a rural andean community. Rural Remote Health. 2021;21(2):6457.
- Paulose B, Kamath N. Quality of life of postmenopausal women in urban and rural communities. J Menopausal Med. 2018;24(2):87–91. doi: 10.6118/jmm.2018.24.2.87.
- Martínez JA, Palacios S, Chavida F, et al. Urban-rural differences in spanish menopausal women. Rural Remote Health. 2013;13(2):1865.
- Voedisch AJ, Dunsmoor-Su R, Kasirsky J. Menopause: a global perspective and clinical guide for practice. Clin Obstet Gynecol. 2021;64(3):528–554. doi: 10.1097/GRF.0000000000000639.
- El Khoudary SR, Greendale G, Crawford SL, et al. The menopause transition and women’s health at midlife: a progress report from the study of women’s health across the nation (SWAN). Menopause. 2019;26(10):1213–1227. doi: 10.1097/GME.0000000000001424.
- Santoro N. Perimenopause: from research to practice. J Womens Health (Larchmt). 2016 Apr;25(4):332–339. doi: 10.1089/jwh.2015.5556.
- Gold EB, Crawford SL, Shelton JF, et al. Longitudinal analysis of changes in weight and waist circumference in relation to incident vasomotor symptoms: the study of women’s health across the nation (SWAN). Menopause. 2017;24(1):9–26. doi: 10.1097/GME.0000000000000723.
- Bromberger JT, Kravitz HM. Mood and menopause: findings from the study of women’s health across the nation (SWAN) over 10 years. Obstet Gynecol Clin North Am. 2011;38(3):609–625. doi: 10.1016/j.ogc.2011.05.011.
- Tang R, Luo M, Li J, et al. Symptoms of anxiety and depression among chinese women transitioning through menopause: findings from a prospective community-based cohort study. Fertil Steril. 2019;112(6):1160–1171. doi: 10.1016/j.fertnstert.2019.08.005.
- King EM, Kaida A, Prior J, et al. Resilience and psychosocial factors linked to symptom experience during the menopause transition for women living with HIV. Menopause. 2022;29(4):430–439. doi: 10.1097/GME.0000000000001926.