
Dear Editor,
We reported a 54-year-old man with a long history of mild plaque psoriasis presented to our Dermatology Unit with multiple confluent erythematous scaling psoriatic plaques on his trunk and lower and upper limbs developed during his third course of lenalidomide treatment for multiple myeloma. The Psoriasis Area and Severity Index (PASI) was 14 (). The patient reported two more recent episodes of psoriasis exacerbation concomitantly with lenalidomide treatment. Each relapse of psoriasis started a few days after the beginning of each course of lenalidomide, which was administered orally at a dosage of 25 mg and 15 on alternate days during the first and the second course, respectively. In both cases psoriasis improvement was rapidly achieved after discontinuation of lenalidomide and a short course of oral prednisone. No infections occurred in the last months. Concomitantly with lenalidomide, he was treated with daratumumab, enoxaparin sodium, lansoprazole, acyclovir and montelukast. We proposed to avoiding discontinuation of lenalidomide and to starting topical treatment with calcipotriol and betamethasone valerate foam. Psoriasis improved after 4 weeks of the aforementioned therapy (PASI 9) with further clinical improvement. Phototherapy was also suggested as a maintenance therapy and the patient reached PASI 90 (). Lenalidomide is a targeted immunomodulatory drug and an analogue of thalidomide. In 2006, lenalidomide was approved by the FDA for the treatment of multiple myeloma (MM) in patients who had received at least one previous therapy (Citation1). Lenalidomide has multiple mechanisms of action, including immunomodulatory, antiangiogenic and antineoplastic effects (Citation2). Lenalidomide produces antitumor activity by multiple mechanisms: it activates CD8 T cells, reduces the number of regulatory T cells, enhances T-cell immune synapses, and increases the ratio of T-helper 1 subsets over T-helper 2 subsets (Citation3). Lenalidomide inhibits proliferation and induces apoptosis of certain hematopoietic tumor cells. Furthermore, Lenalidomide blocks tumor angiogenesis by inhibiting the migration and adhesion of endothelial cells and the formation of microvessels (Citation2). Lenalidomide is more effective than thalidomide in inducing T cell proliferation and enhancing IL-2 and interferon γ (IFNγ) production. Finally, this drug could also inhibit the production of proinflammatory cytokines such as tumor necrosis factor-α (TNF-α), IL-1, IL-6 and IL-12 and may increase the production of the anti-inflammatory cytokine IL-10 (Citation2,Citation3). The most common toxicities of lenalidomide are hematological, including neutropenia, anemia and thrombocytopenia. Non-hematologic adverse effects include gastrointestinal disorders, fatigue, skin rash, pruritus, cough, pyrexia, dyspnea, peripheral edema, infection, insomnia, muscle cramps, tremor, and dizziness (Citation4). Moreover, lenalidomide use has been associated with severe skin disorders, such as toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome (SJS), and drug reaction with eosinophilia and systemic symptoms (DRESS) (Citation2). To the best of our knowledge, this is the first reported case of psoriasis exacerbation induced by lenalidomide. Until now, two cases of psoriasis induced by thalidomide have been described (Citation5,Citation6) ,and several exacerbations of psoriasis by thalidomide have been reported in literature (Citation7,Citation8). Although the mechanism by which these reactions occur is not fully understood, a role of lenalidomide on TNF-α has been suggested. The most widely accepted hypothesis suggests there is an interaction between TNF-α and interferon alfa (IFN-α). Recently, some Authors confirmed that TNF regulates type I-IFN production by plasmacytoid dendritic cells (pDCs) and that anti-TNF therapy causes its increase, leading to paradoxical psoriasis (Citation9). Although exacerbation of psoriasis by lenalidomide is a rare event, it should be promptly managed by a dermatologist in order to avoid discontinuation of life-sparing therapies.
Figure 1. (a–c) Clinical presentation of exacerbation of psoriasis.
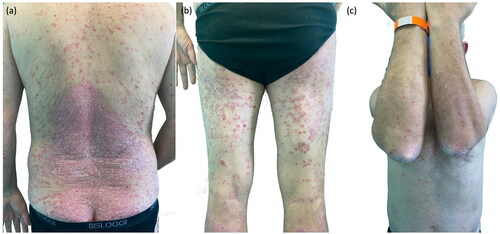
Figure 2. (a–c) Clinical resolution after phototherapy and topical treatment.

Ethical approval
The patient referred in this manuscript gave his written informed consent to the publication of their case details.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Additional information
Funding
References
- Shah SR, Tran TM. Lenalidomide in myelodysplastic syndrome and multiple myeloma. Drugs. 2007;67(13):1869–1881.
- Blair HA. Lenalidomide: a review in previously treated follicular lymphoma. Drugs. 2020;80(13):1337–1344.
- Zhu YX, Kortuem KM, Stewart AK. Molecular mechanism of action of immune-modulatory drugs thalidomide, lenalidomide and pomalidomide in multiple myeloma. Leuk Lymphoma. 2013;54(4):683–687.
- Holstein SA, McCarthy PL. Immunomodulatory drugs in multiple myeloma: mechanisms of action and clinical experience. Drugs. 2017;77(5):505–520.
- Ferrazzi A, Zambello R, Russo I, et al. Psoriasis induced by thalidomide in a patient with multiple myeloma. BMJ Case Rep. 2014;2014(jun27 1):bcr2014204469–bcr2014204469.
- D'Arena G, Galdo G, Musto P. Thalidomide-induced psoriasis in a patient with multiple myeloma. Postgrad Med J. 2019;95(1121):171.
- Dobson CM, Parslew RA. Exacerbation of psoriasis by thalidomide in behçet’s syndrome. Br J Dermatol. 2003;149(2):432–433.
- Varma K, Finlay AY. Exacerbation of psoriasis by thalidomide in a patient with erythema multiforme. Br J Dermatol. 2006;154(4):789–790.
- Mylonas A, Conrad C. Psoriasis: classical vs. Paradoxical. The Yin-Yang of TNF and type I interferon. Front Immunol. 2018;9:2746.