
Dear Editor,
Alopecia areata (AA) is a common autoimmune dermatosis characterized by nonscarring hairless patches that can involve the scalp and/or any other site where hair is present (Citation1). Classically, patterns of scalp alopecia were categorized as patchy AA, alopecia ophiasis, alopecia sisaipho, diffuse AA, and alopecia totalis/alopecia universalis. And it was reported that different patterns of alopecia may be related to the clinical prognosis of patients (Citation2). Our case illustrates that alopecia areata can mimic the clinical manifestations of androgenic alopecia.
Case report
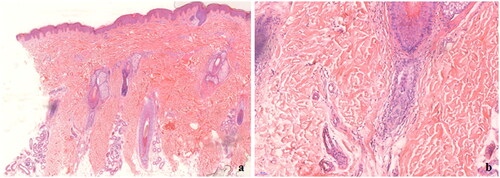
A 17-year-old teenager presented to the dermatology department with a 6-year history of diffuse hair loss. The patient and his family reported that the hair loss began suddenly and stabilized quickly after a few months, with no regrowth in the patch of alopecia. He denied any extra-scalp hair loss but had a family history of alopecia areata. His father, who had accompanied him to our clinic, had lost all his hair. Physical examination demonstrated the frontal and bilateral temporal hairline shifted back in a characteristic ‘U’ shape, and the occipital hair density was slightly reduced (). The hair pull test was negative. Examination with a dermatoscopy showed more than 20% hair diameter variability as a characteristic finding for androgenetic alopecia. Scalp biopsy specimens obtained from the alopecic rim revealed that the number of follicles decreased significantly with a few lymphocyte infiltrations (). Although the pathologic findings in alopecia areata vary with the biopsy site and the course of the disease, the diagnosis of alopecia areata is still not clear.
Figure 1. (a–d) Characteristic “U” pattern hair loss; (e–h) a dramatic hair regrowth after 3 months of treatment with tofacitinib.
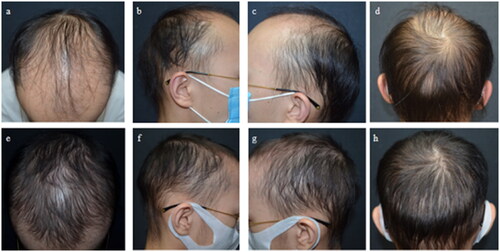
Figure 2. Histopathologic features (hematoxylin-eosin staining). (a) The numbere of follicles decreased significantly with high proportions of follicles in catagen or telogen (original magnification ×50). (b) Vertical columns of connective tissue can be seen (original magnification ×200).
The patient had been treated with topical minoxidil for half a year before came to our clinic, however, without any improvement. With his father’s agreement, diagnostic therapy with tofacitinib was given. After 3 months, a dramatic response of hair regrowth was observed (). Eventually, we confirmed the patient’s diagnosis to alopecia areata with pattern hair loss.
Discussion
Androgenic alopecia (AGA) in adolescent population is not rare (Citation3). Men with AGA typically describe slow, progressive, asymptomatic hair loss with a ‘female pattern’ or ‘male pattern’ distribution (Citation3). We suspect that the patient may have co-existing AA because of his family history and the atypical progression of hair loss. Despite the atypical histopathology of AA, the chronicity of the patient’s disease and the uselessness of minoxidil alone followed by rapid and excellent treatment feedback with oral tofacitinib all support the diagnosis of AA. As mentioned above, the histopathologic features of AA depend on the acuity of inflammation in the biopsied area (Citation4). Biopsy specimens from areas of the advanced stage can present with high proportions of follicles in catagen or telogen, even lack of an inflammatory cell infiltration.
Limited studies have suggested the possibility of Janus kinase (JAK) inhibitors for the treatment of AGA. The term ‘microinflammation’ in AGA represented a slow and indolent process. Different from AA, the inflammation of AGA mainly infiltrates the infundibular and isthmic, which was hypothesized to involved the pathogenesis. However, a recent case report showed 4 AA patients successfully treated with JAK inhibitors but with pattern distribution hair regrowth (Citation5). In addition, a small explorer trial showed no significant difference between minoxidil alone and minoxidil combined with 0.1% betamethasone dipropionate for AGA (Citation6). The role of inflammation in AGA remains to be investigated.
Our patient presented with what we believe is a novel clinical manifestation of AA. Follow-up studies are needed to identify this ‘pattern distribution AA’ individuals and investigate what’s special about such clinical phenotype.
Ethical statement
The patients in this manuscript have given written informed consent to publication of their case details.
Author contributions
All authors contributed to the final manuscript. J-DH collected the clinical data and drafted the manuscript. Corresponding authors WS read and revised the manuscript. All authors contributed to the articleand approved the submitted version.
Supplemental Material
Download MS Power Point (28.7 MB)Acknowledgements
All authors thank the patient in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Gilhar A, Etzioni A, Paus R. Alopecia areata. N Engl J Med. 2012;366(16):1–2.
- Lee H, Choe SJ, Lee WS. Method for describing patterns and distributions of alopecia areata which may be helpful for patient characterization and predicting prognosis. J Dermatol. 2019;46(8):739–740.
- Griggs J, Burroway B, Tosti A. Pediatric androgenetic alopecia: a review. J Am Acad Dermatol. 2021;85(5):1267–1273.
- Whiting DA. Histopathologic features of alopecia areata: a new look. Arch Dermatol. 2003;139(12):1555–1559.
- Yale K, Pourang A, Plikus MV, et al. At the crossroads of 2 alopecias: androgenetic alopecia pattern of hair regrowth in patients with alopecia areata treated with oral Janus kinase inhibitors. JAAD Case Rep. 2020;6(5):444–446.
- Gheisari M, Hamidi AB, Hamedani B, et al. Androgenetic alopecia; an attempt to target microinflammation. Dermatol Ther. 2020;33(2):e13266.