
Abstract
Dissecting cellulitis of the scalp (DCS) is a rare recurrent inflammatory disease of unknown etiology. Ideal treatment of DCS remains unclear. We treated DCS with 2940-nm erbium Yttrium-aluminum-garnet (YAG) laser in 12 patients and assessed the efficacy by Physicians Global Assessment (PGA), number of inflammatory nodules, abscesses, and area of alopecia. After a mean treating session of 2.2 months, 10 patients reached PGA 0 (initial PGA 1) or 1 (initial PGA ≥2). At the end of treatment, there was 84%, 100%, and 74% regression in nodules, abscesses, and alopecia area, respectively. No severe adverse effect was observed. 2940-nm erbium: YAG laser may be an effective and safe way to treat DCS resistant to other therapies.
Introduction
Dissecting cellulitis of the scalp (DCS), also known as perifolliculitis capitis abscedens et suffodiens (PCAS) or Hoffmann disease, is a rare condition mostly occurs in black males aged 20 to 40 years. The disease presents with suppurative nodules, interconnecting sinuses, and patchy hair loss. Deep follicular occlusion may be the most important pathology in DCS.
The etiology is not well understood, and ideal treatment of DCS remains unclear (Citation1). The aim of medical treatment is to reduce inflammation and to prevent secondary infection. Oral antibiotics and isotretinoin were first line therapy for DCS (Citation2). However, these treatments were often discontinued due to disease remission and relapse. Intralesional corticosteroids, incision and drainage were advocated for symptom relief. Case reports and series also reported use of tumor necrosis factor (TNF) inhibitors (Citation3,Citation4), surgical excision (Citation5) and laser therapy (Citation6,Citation7) in treating DCS.
2940-nm erbium yttrium-aluminum-garnet (YAG) laser wavelength is highly absorbed by water and collagen and is used for resurfacing the acne scar (Citation8). Previously, we have reported two cases of DCS successfully treated with 2940-nm erbium: YAG laser (Citation9). In this study, we conducted a single center prospective study to evaluate the efficacy and safety of 2940-nm erbium: YAG laser in treating DCS.
Methods
This is a prospective single center study conducted in the Department of Dermatology, Second Affiliated Hospital, Zhejiang University School of Medicine from November 2021 to November 2022. The diagnosis of DCS was based on physical examination and negative bacterial culture results. Consecutive adult, nonpregnant patients were included.
Compound lidocaine cream (25 mg prilocaine: 25 mg lidocaine/10g) was applied 1 h before laser treatment. All lesions on the scalp were treated with 2940-nm multifractional erbium: YAG laser (MCL Asclepion Laser Technologies) by using parameters of 300 µs, 21 j/cm2, 8 HZ with 0.56 mm spot size in N25 mode. Immediate cooling with ice were provided after each treatment and erythromycin ointment was prescribed for 7 days after the procedure. Sessions were repeated 4 weeks apart with 3 j/cm2 increase each, up to a maximum dose of 30j/cm2.
The patients were photographed with a digital camera before and after each session. Clinical efficacy was evaluated by two dermatologists independently. Physicians Global Assessment (PGA), number of inflammatory nodules, abscesses and area of alopecia were assessed at baseline, before each session, and 4 weeks after the last session. Area of alopecia was measured by percentage of hair loss of the scalp. A patient was considered in disease remission if PGA reached 0 (initial PGA 1) or 1 (initial PGA ≥2). Patients were asked about adverse events after laser treatment such as erythema, edema, pain and pigmentation. All patients were followed up via telephone at 6 months to check for recurrence.
All analyses were performed with the SPSS version 23.0 statistical package. Continuous data were described as mean ± SD. Categorial variables were expressed as counts (percentages).
Results
Twelve patients were included, all patients were male (). The mean age at symptom onset was 22.1 ± 5.8 years and the mean BMI was 23.9 ± 1.2 kg/m2. Seven (58%) patients tried treatments including oral antibiotics, isotretinoin, incision, and intralesional steroids previously. Four (33%) patients had initial PGA of 3, 5 (42%) patients had initial PGA of 2, and 3 (25%) patients had initial PGA of 1. Of the 12 patients, 2 patients with initial PGA of 1 were in disease remission after the first session (). Ten patients received the second session, with 3 patients in disease remission and 1 lost to follow-up. The uncured 6 patients received the third treatment, and 5 patients of them achieved disease remission. The mean number of treatment sessions needed to cure the lesions was 2.2 ± 0.9.
Figure 1. Flowchart of the participants.
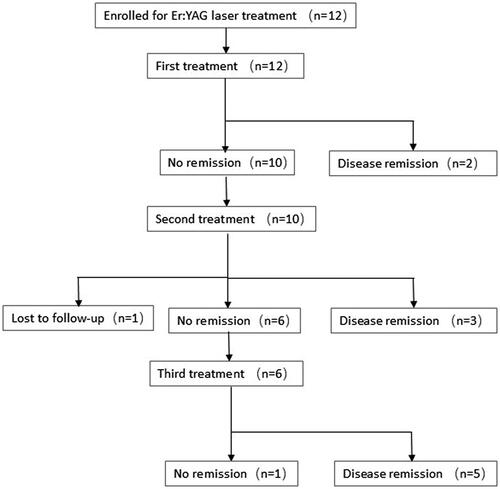
Table 1. Patient information.
After a mean duration of 2.2 months, the mean PGA score decreased from 2.1 to 1.2. We observed 31%, 61%, and 84% decrease in the number of nodules respectively (). Abscesses all disappeared at the end of the second session. The rate of hair regrowth was 10%, 51% and 74% at the end of first, second and third session. The main adverse effects of erbium:YAG laser were pain and erythema, which were reported in all patients. No post-inflammatory hyperpigmentation occurred. Two patients reported remission at the 6 months follow-up. Both patients had initial PGA of 3 and respond well to laser therapy. After lesion recurrence at 6 months follow-up, laser therapy was given to these two patients again with lesion improvement ().
Figure 2. Marked improvement of scalp lesion and hair regrowth before and after Erbium: YAG laser treatment sessions. Patient No.1 before (A) and after (B) 3 sessions. Patient No.6 before (C) and after (D) 3 sessions.
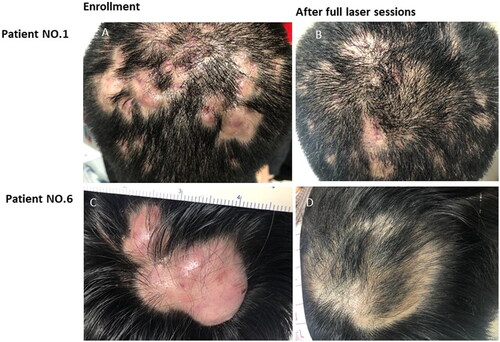
Table 2. Regression after Er:YAG laser sessions.
Discussion
DCS is a chronic inflammatory disease of scalp which most commonly occurs in black males aged 20 to 40 years old. The main manifestations of DCS including subcutaneous nodules and abscesses of the scalp, alopecia, with or without secondary bacterial infection, especially Staphylococcus aureus (Citation10). The key pathogenic change in DCS is follicular occlusion. Patients with DCS may exhibit other symptoms of follicular occlusion tetrad, including hidradenitis suppurativa, acne conglobate, and pilonidal sinus (Citation11). Although the etiology of DCS is still unclear, interleukin-1 and neutrophilic infiltration may play an important role (Citation12).
Evidence to define the ideal treatment is lacking. Most therapeutic options are based on case reports and case series. Oral antibiotics therapy and isotretinoin are the most given oral medications for DSC, which can both decrease disease activity to a moderate degree (Citation12). However, recurrence after discontinuation of treatment is often observed. Anti TNF agents, including adalimumab and infliximab, decrease inflammatory nodules and abcesses of DCS (Citation3). Moreover, photodynamic therapy (PDT), intralesional corticosteroids, and incision and drainage can be used to alleviate symptoms and pain.
After a mean treating period of 2.2 months with the erbium: YAG laser, symptoms improved with 100% regression in abscess and 84% regression in inflammatory nodules. The erbium: YAG laser emits light at a wavelength of 2940 nm, which is close to the absorption peak pf water (3000 nm). Superficial ablation occurs with nearly all of the energy absorbed in the epidermis and papillary dermis (Citation13). The superficial tissue ablation causes thermal damage which may attenuate the inflammatory reaction in the lesions of DCS.
More impressively, erbium: YAG laser treatment led to hair regrowth on the scalp, which was not described in previous studies. Patchy alopecia could bring anxiety, and even lead to decrease of life quality especially to young adults. Histologically, scarring alopecia in DCS was characterized by destroyed hair caused by follicles neutrophilic inflammation. The number of hair follicles increased after erbium: YAG laser treatment in a mice model (Citation14).
2940 nm erbium: YAG laser may be an effective and safe treatment for patients with DCS.
Consent statement
Informed consents were provided by patients for publication of the cases.
Authors contribution statement
Mengjun Xu collected the data and wrote the manuscript. Suiqing Cai revised the manuscript. Jianliang Yan designed the treatment and performed the laser therapy.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Data available on request from the authors.
Additional information
Funding
References
- Thomas J, Aguh C. Approach to treatment of refractory dissecting cellulitis of the scalp: a systematic review. J Dermatolog Treat. 2021;32(2):1–4. doi:10.1080/09546634.2019.1642441.
- Segurado-Miravalles G, Camacho-Martinez FM, Arias-Santiago S, et al. Epidemiology, clinical presentation and therapeutic approach in a multicentre series of dissecting cellulitis of the scalp. J Eur Acad Dermatol Venereol. 2017;31(4):e199–e200. doi:10.1111/jdv.13948.
- Alzahrani M, Coste V, Konstantinou MP, et al. Treatment of dissecting cellulitis of the scalp wth tumor necrosis factor inhibitors: a retrospective multicenter study. Clin Exp Dermatol. 2023;48(5):528–530. doi:10.1093/ced/llad036.
- Brandt HR, Malheiros AP, Teixeira MG, et al. Perifolliculitis capitis abscedens et suffodiens successfully controlled with infliximab. Br J Dermatol. 2008;159(2):506–507. doi:10.1111/j.1365-2133.2008.08674.x.
- Nijhawan RI. Staged full-thickness excisions and porcine xenograft placement for extensive dissecting cellulitis of the scalp. Dermatol Surg. 2019;45(10):1324–1327. doi:10.1097/DSS.0000000000001732.
- Krasner BD, Hamzavi FH, Murakawa GJ, et al. Dissecting cellulitis treated with the long-pulsed Nd:YAG laser. Dermatol Surg. 2006;32:1039–1044.
- Boyd AS, Binhlam JQ. Use of an 800-nm pulsed-diode laser in the treatment of recalcitrant dissecting cellulitis of the scalp. Arch Dermatol. 2002;138(10):1291–1293. doi:10.1001/archderm.138.10.1291.
- Cenk H, Sarac G. Effectiveness and safety of 2940-nm multifractional Er:YAG laser on acne scars. Dermatol Ther. 2020;33:e14270.
- Xu M, Yan J. 2940-nm multifractional erbium: yttrium-aluminum-garnet laser for the treatment of dissecting cellulitis of the scalp: case reports and literature review. J Dermatol. 2022;49:e230–e231.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Vasanth V, Chandrashekar BS. Follicular occlusion tetrad. Indian Dermatol Online J. 2014;5(4):491–493. doi:10.4103/2229-5178.142517.
- Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174(2):421–423. doi:10.1111/bjd.13999.
- Riggs K, Keller M, Humphreys TR. Ablative laser resurfacing: high-energy pulsed carbon dioxide and erbium: yttrium-aluminum-garnet. Clin Dermatol. 2007;25(5):462–473. doi:10.1016/j.clindermatol.2007.07.003.
- Ke J, Guan H, Li S, et al. Erbium: YAG laser (2,940 nm) treatment stimulates hair growth through upregulating wnt 10b and beta-catenin expression in c57bl/6 mice. Int J Clin Exp Med. 2015;8:20883–20889.