
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Aim
In this narrative review the potential and importance of handcycling are evaluated. Four conceptual models form the framework for this review; (1) the International Classification of Functioning, Disability and Health; (2) the Stress-Strain-Capacity model; (3) the Human-Activity-Assistive Technology model; and (4) the power balance model for cyclic exercise.
Methods
Based on international handcycle experience in (scientific) research and practice, evidence-based benefits of handcycling and optimization of handcycle settings are presented and discussed for rehabilitation, daily life and recreational sports.
Results
As the load can be distributed over the full 360° cycle in handcycling, peak stresses in the shoulder joint and upper body muscles reduce. Moreover, by handcycling regularly, the physical capacity can be improved. The potential of handcycling as an exercise mode for a healthy lifestyle should be recognized and advocated much more widely in rehabilitation and adapted sports practice.
The interface between handcycle and its user should be optimized by choosing a suitable person-specific handcycle, but mainly by optimizing the handcycle dimensions to one’s needs and desires. These dimensions can influence efficient handcycle use and potentially improve both endurance and speed of handcycling.
Conclusion
To optimize performance in rehabilitation, daily life and recreational sports, continued and more systematic research is required.
Handcycling allows users to travel farther distances at higher speeds and to train outdoors. It should be recognized as an alternative exercise modality for daily outdoor use, also already in early rehabilitation, while it contributes to a healthy lifestyle.
To individualize handcycle performance, the user-handcycle (assistive device) interface as well as the vehicle mechanics should be optimized to minimize external power and reduce friction, so that the upper body capacity can be efficiently used.
To optimize handcycling individual performance, both the physiological and biomechanical aspects of handcycling should be considered when monitoring or testing handcycle exercise.
Implications for rehabilitation
Introduction
People with lower-limb impairments depend on other forms of ambulation than walking for all their mobility and physical activity. If the upper body can still be physically active, the manual handrim wheelchair is the most common form of wheeled mobility [Citation1–3]. An alternative way of outdoor wheeled mobility to cover longer distances is the handcycle [Citation4–6]. Handcycles exist in a number of different forms, for example as an attachable unit to a wheelchair (with/without power assist) or as a fixed-frame tricycle with a number of different body positions and often with a range of gear settings (). The size of the tricycle or any other handcycle makes functional handcycling most suitable as an outdoor activity, obviously including indoor race tracks and/or gymnasia.
Figure 1. Two functionally different groups of handcycle configurations following the arm power (AP) and arm-trunk power (ATP) paradigm, combined with the current international classification for handcycle competition (H1–H5) [Citation7,Citation8]. H1, H2: classes for athletes with tetraplegia; H3: athletes lacking trunk function; H4: athletes with trunk function (classes H1, H2, H3, and H4 use arm powered (AP) handcycles); H5: athletes who can sit on their knees, they use arm-trunk powered (ATP) handcycles.
![Figure 1. Two functionally different groups of handcycle configurations following the arm power (AP) and arm-trunk power (ATP) paradigm, combined with the current international classification for handcycle competition (H1–H5) [Citation7,Citation8]. H1, H2: classes for athletes with tetraplegia; H3: athletes lacking trunk function; H4: athletes with trunk function (classes H1, H2, H3, and H4 use arm powered (AP) handcycles); H5: athletes who can sit on their knees, they use arm-trunk powered (ATP) handcycles.](/cms/asset/1ea68ae4-7a42-4859-a79f-04e6552b5d7c/idre_a_1815872_f0001_c.jpg)
Individuals with lower limb impairments have a high risk of obesity with the consequent risk for cardiovascular disease, due to inactivity and a subsequent negative impact on the energy balance, i.e., using less energy than taking in [Citation9–14]. Regular handcycling may help preserve fitness and health, as well as upperbody function [Citation15–23]. In addition, handcycling evolved into specialized sports disciplines under the umbrella of the UCI (Union Cycliste Internationale), and its popularity today is expressed in elite competitions at the Paralympics since 2004 [Citation24–26] and numerous races and events worldwide [Citation27,Citation28].
To optimize handcycling for rehabilitation, daily living or recreational sports even further, there is a need to balance the components of the individual, environment and assistive device. The current narrative review intends to provide a base of knowledge for today’s handcycling practice and presents starting points for continued handcycling research. Four inter-connected models form the conceptual framework throughout this narrative review, in which we attempt to draw the state-of-the-art in the scientific literature on handcycling.
The first framework, which is commonly used in the context of rehabilitation, preventive medicine and health care is the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization () [Citation29]. It is deemed appropriate as a communication tool among policy makers, countries, health care disciplines and professionals as well as a tool to set goals in both (individual) rehabilitation practice and sciences. Secondly, from an occupational health and preventive medicine perspective of the individual, the Stress-Strain-Capacity (SSC) model of van Dijk et al. [Citation31] has been suggested instrumental (). In health, physical, cognitive and/or mental stressors of work or daily life lead to physiological, mechanical and/or mental strains in the human system within the individual capacity boundaries. In upper body cyclic exercise, stressors may easily exceed individual capacity which may impact functioning as well as health. Thirdly, a more ergonomically-oriented framework for assistive technology design and fitting has been advised by Cook and Hussey: the Human-Activity-Assistive Technology - the HAAT-model () [Citation32]. In handcycling, the model potentially focuses on the optimal interaction among assistive device, individual and/or environment considering the cyclic propulsion task ahead. Lastly, to help understand and study upper body cyclic exercise in a more biophysical context, the power balance model for cyclic exercise was shown to be useful (). It was initially developed for speed skating and swimming by van Ingen Schenau [Citation35,Citation36]. Later, it was applied to handrim propulsion by van der Woude [Citation37–39], in wheelchair court sports by Mason [Citation40] and in handcycling by a number of research groups [Citation33,Citation34,Citation41–43].
Figure 2. Four conceptual frameworks that fits in the evaluation of handcycle performance. (a) International Classification of Functioning, Disability and Health [Citation29] as applied for persons with a spinal cord injury. Reprinted from [Citation30], Copyright 2006, with permission from Elsevier. (b) Stress Strain Capacity Model [Citation30,Citation31]. Reprinted from [Citation30], Copyright 2006, with permission from Elsevier. (c) Human Activity Assistive Technology Model [Citation32]. (d) Power balance model [Citation33,Citation34]. Reprinted from [Citation33], with permission of author.
![Figure 2. Four conceptual frameworks that fits in the evaluation of handcycle performance. (a) International Classification of Functioning, Disability and Health [Citation29] as applied for persons with a spinal cord injury. Reprinted from [Citation30], Copyright 2006, with permission from Elsevier. (b) Stress Strain Capacity Model [Citation30,Citation31]. Reprinted from [Citation30], Copyright 2006, with permission from Elsevier. (c) Human Activity Assistive Technology Model [Citation32]. (d) Power balance model [Citation33,Citation34]. Reprinted from [Citation33], with permission of author.](/cms/asset/4103d198-07d5-439a-9d84-96f8ede79354/idre_a_1815872_f0002_b.jpg)
Based on these conceptual models the current review explores the physiological, biomechanical, ergonomic and technical details of handcycling and its potential to promote functioning, health and participation, as well as handcycle performance in recreational sports. The following overarching questions will be addressed in this narrative review:
What are the potential benefits of handcycling in rehabilitation, daily living and recreational sports and how can they be evaluated?
Which factors should be considered for optimizing individual handcycle performance and how can they be evaluated?
Methods
In this narrative review, the international literature on handcycling and relevant wheeled mobility was summarized in a collaborative effort of a team of international experts in the field of handcycling and wheelchair research, both in rehabilitation and adapted sports practice. Given the available literature, no explicit exclusion criteria were used for this narrative review. Available studies were critically assessed at any instance.
Results
Potential benefits of handcycling in rehabilitation, daily living and recreational sports
Following the ICF model of the WHO [Citation29], independent mobility is one of the main goals of rehabilitation of patients who are wheelchair bound. The functionality of the assistive device outdoors not only depends on the skills of the user or mechanical characteristics, it also highly depends on the environmental conditions; i.e., availability of (level) sidewalks, with curbs or steep sections [Citation29]. Power-support systems may be a solution in challenging terrain [Citation44], but a disadvantage may be (battery) costs, weight and thus their even larger difficulty to transport e.g., in a car [Citation45]. Moreover, a transfer into a car is probably one of the most strenuous activities for the upper extremities [Citation46]. Handcycling as an alternative for outdoor mobility should be explored as it may contribute to a healthy lifestyle. In addition, with an attachable unit, no transfers between propulsion modalities are needed.
Health benefits
Physiological and biomechanical strain
In handcycling, the full 360°, i.e., 100% of the movement cycle can be used [Citation5,Citation47–53], potentially employing most of the body musculature. The body muscles are alternatingly active throughout the 360° cycle during push and pull phases of handcycling and the task load is spread over time and larger alternating muscle groups [Citation54], reducing local and overall peak loads [Citation55]. One approach to assess the risk for overuse injuries is to analyze the force acting within the joint or the strain on the muscles that are stabilizing the joint. Both the forces as well as the strain can be calculated by inverse dynamics and with the aid of a biomechanical model, based on three-dimensional anatomical information, like the Delft Shoulder and Elbow Model (DSEM) [Citation55–58]. With respect to the shoulder overuse injury, which is a common problem in wheelchair users, higher mean and especially higher peak glenohumeral joint forces point to a higher risk for injuries [Citation59]. Additionally, high strain on the rotator cuff muscles can lead to fatigue which can result in less ability to stabilize the shoulder joint and can therefore increase the risk for shoulder injury. With use of the DSEM, handcycling is found to be less straining for the shoulder joint when directly compared to handrim wheelchair propulsion [Citation55]. The mean glenohumeral contact force during handcycling at 55 W is 45% of the body weight, whereas this is 75% during wheelchair propulsion at the same intensity level. The peak glenohumeral contact force at this intensity is about 100% of the body weight for handcycling, whilst this is 195% for wheelchair propulsion [Citation55]. Consequently, the risk of overuse injuries associated with the repetitive nature of propulsion is lower in daily outdoor handcycle use compared to outdoor wheelchair use. In addition, handcycling has a mechanical efficiency of 10–17% at submaximal level, while this is only 5–10% during handrim wheelchair propulsion [Citation4,Citation55,Citation60,Citation61]. Therefore, a switch to outdoor handcycling could be beneficial to reduce physiological and biomechanical strain of ambulation.
Active lifestyle
Inactivity is a potential risk in wheelchair users, as they generally show low activity levels throughout the day [Citation9,Citation62]. Promoting an active lifestyle within the early rehabilitation process, e.g., by handcycling, can help increase physical activity after discharge [Citation63]. Handcycling can be physiologically taxing when negotiating high speeds and/or power outputs. Nevertheless, given its physiological and biomechanical benefits, handcycling is also suitable as a safe training mode to regain and maintain fitness [Citation7,Citation62,Citation64–72]. It is also possible to safely train patients who have a very low physical capacity for instance due to a high cervical spinal cord lesion [Citation73–75] or because they are at the early start of rehabilitation [Citation6,Citation67,Citation76,Citation77]. Especially for those who are undertrained or those with a relatively high body mass in relation to their available active arm muscle mass, arm crank ergometers can be useful to be able to start training at a very low power output level [Citation74,Citation75].
Handcycling is essentially an outdoor activity and allows to commute and/or exercise outdoors, even simultaneously. Exercising in the green and natural environment has shown to have a larger effect on mood, self-esteem, blood pressure, tension, anger, confusion and depression compared to exercising in a plain laboratory environment [Citation78–80]. Exercise in the free leads to the perception of higher energy levels and positive feelings [Citation80].
Effects of exercising
Having a closer look on typical physiological markers predicting handcycling performance such as peak power and maximal lactate steady-state power as used in able-bodied sports seems obvious. Although not fully applicable, the general training guidelines, prescribed by the American College of Sports Medicine (ACSM) can be used as a starting point for developing training guidelines more specific for upper body exercise [Citation15,Citation17,Citation61,Citation66]. The recommendation for persons with chronic diseases and disabilities is to exercise three to five times a week, for 20–60 min, at an intensity of 40–70% of the heart rate reserve (HRR%) [Citation17].
The ergometer is often used in combination with physiological measurements and training protocols (). To evaluate upper body anaerobic exercise characteristics an all-out sprint effort (e.g., a Wingate test protocol or isokinetic sprint testing) has shown to be useful [Citation86–88]. The isokinetic sprint test protocol ranging 15–20 s duration has been employed recently by Zeller et al. [Citation87] and Kouwijzer et al. [Citation88] to evaluate sprint performance within handcycling. It is performed in a similar manner to testing able-bodied persons on a bicycle as the participant is instructed to maintain a maximal pace against a certain resistance load, mostly scaled to their body weight for the duration of the trial. In this way, peak, minimum and mean (anaerobic) power output and rate of fatigue can be determined [Citation86,Citation89]. In combination with an incremental step protocol a cardiopulmonary exercise test (CPET) can measure (aerobic) physiological values at peak power output [Citation43,Citation51,Citation52,Citation60,Citation61,Citation65,Citation67,Citation70,Citation71,Citation90–109]. It is important to individualize the graded exercise tests to gain the true peak values in individuals (with spinal cord injury) [Citation110]. Thus, peak values of (an)aerobic upper body performance and the CPET-based ventilatory thresholds can be determined, from which a personalized training scheme (i.e., load, frequency, duration) can be set in rehabilitation and (recreational) sports [Citation61,Citation72,Citation98,Citation111].
Table 1. Overview of research on handcycle training.
Amongst others, Valent et al. [Citation67,Citation76,Citation81] have investigated the effects of handcycle training on physical capacity. Within a group of persons with paraplegia and tetraplegia, they found that only the persons with paraplegia significantly improve their peak VO2 (+29%), peak power output (+42%) and muscle strength (e.g., +30% elbow extension) on a handrim wheelchair exercise test. The participants handcycled at least once a week within their clinical rehabilitation (average period of six months), however, were not following a specific training program. After the first year after discharge, no further significant improvements were found [Citation67]. Also, the effects of an additional structured training program within early clinical rehabilitation in the Netherlands was investigated in persons with spinal cord injury below the level of C5. Wheelchair capacity and muscle strength of a handcycling group were compared to a control group, who only following the regular rehabilitation program. The handcycle group trained in an add-on handcycle with synchronous setting (for 35–45 min twice a week) on top of their rehabilitation program and performed an extra test for handcycle capacity. No significant effect of an additional synchronous handcycling training over regular rehabilitation program was found for wheelchair capacity (peak power output and peakVO2). However, for the handcycling group, improvements of muscle strength and handcycle capacity in terms of peak power output (+22%) were found [Citation81]. In a third study, in which persons with tetraplegia followed a structured handcycling training two years after their injury occurred, handcycling seems to improve physical capacity. After 24 training sessions of 35–45 min at 60–80 HRR%, spread over 8–12 weeks, an increase of 8.7% in peakVO2 and 20.2% in peak power output was found [Citation76].
Since 2013 the HandBikeBattle (HBB), a yearly handcycle event in which participants complete a 20.2 km mountain time-trial (with ±900 m elevation), is held in Austria [Citation112]. All participants are screened and train in self-organizing teams of their rehabilitation center for a period of 4–5 months prior to the HBB event. Data from this project showed that self-regulated handcycle training over a period of five months can increase peak power output (+17%), peak oxygen uptake (+7%), peak ventilation (+9%) and reduce fat mass index (−6.3%), BMI (−2%) and waist circumference (−4%) [Citation65,Citation83,Citation113,Citation114].
To understand, individualize and optimize upper body training further, different training programs must be evaluated in a diverse and large population of wheelchair users, as they may respond differently to training than able-bodied persons would.
Factors for optimizing individual handcycle performance
Vehicle mechanics
Handcycling, either in rehabilitation, daily living or recreational sports, is a form of upper body exercise that leads to ambulation over a given distance and at a given speed. The individual produces upper body muscle work (En) that is transferred through a kinetic chain of upper body segments and muscles to the handlebars and cranks of the handcycle. The mechanical work that needs to be produced is to counteract the external power losses (Pext), due to drag or friction forces that impact the handcycle-user combination () [Citation33,Citation34]. To evaluate the handcycle performance and with the ambulant technology that is available for bicycling today, it is possible to measure the external power output. External power output is dynamically measured with strain gauge-based technologies at the crank, at the pedals or in the front wheel hub. The measurements are often combined with heart rate for a holistic approach. Each of these technologies was tested for reliability and have high degrees of ecological validity in cycling, and potentially in handcycling [Citation90,Citation103,Citation115,Citation116]. They can indeed reliably measure power output both in and outdoors, in training, racing or sports conditions, at both the lower and high-end of the performance spectrum and even at low levels of power output and speed [Citation91,Citation109,Citation117–119].
In EquationEquation (1)(1)
(1) the power balance in cyclic actions in general, hence including handcycling, is presented [Citation35].
(1)
(1)
The drag consists of rolling (Froll), internal (Fint) and air friction (Fair). When propelling up a slope an additional drag force is needed to overcome gravity (Fincl), however when propelling downslope, work is returned to the handcycle-user combination. When accelerating, an additional term is to be produced, namely mass times acceleration (m·a).
Rolling friction
Influencing factors of rolling resistance are in general similar to those for bicycles or wheelchairs [Citation37,Citation120–124]. Tire characteristics and pressure can substantially contribute to the rolling friction, therefore it is important inflate the tires on a regular basis. Also wheel size and alignment are critical keys in rolling friction, where a larger wheel will reduce the resistance. The weight of the device as well as of the user is other factor that will contribute to the resistance. In sports, where speed is important, a lightweight tricycle is the best option. However, in daily use, robustness is also important and one might choose for a heavier, but sturdier version.
Using either drag tests on special drums or on a treadmill on the one hand, using over ground coast down tests on the other, rolling friction coefficients for handcycle wheels can be estimated (0.003–0.017) [Citation109,Citation122,Citation125]. In those drag tests, the person is inert and not actively propelling the vehicle, thereby excluding the internal friction and the task dynamics from the measurements. Due to the low force magnitude and its multifactorial nature, even under standardized treadmill conditions, consistent outcomes are not self-evident [Citation125]. Nevertheless, the outcomes of such drag tests are used in research to individualize the resistance during exercise [Citation109,Citation122].
Internal friction
Internal friction is defined by the chain friction, the chain wheel characteristics, and gear characteristics and settings, the quality and the maintenance there-off. The chain, chain wheel, and gears in a handcycle are equal to bicycle materials, therefore, similar frictional losses are expected for both types of cycles. The internal frictional losses were estimated to be around 5% of the rolling resistance in chain driven bicycles [Citation124]. Estimated transmission losses can be as low as 2–3% and up to 15% and higher, with lower values for derailleur transmissions as opposed to built-in variable gear hubs [Citation124]. A derailleur gear has lower internal friction, whereas a hub gear is more robust. The choice of material is dependent on the task, sport versus commuting, or the environment in which one uses the handcycle (). Either way, maintenance is a critical factor to internal friction and rider safety, therefore e.g., regular greasing or tensioning of the chain is necessary, apart from checks on brake technology and visibility.
Air friction
Both rolling and internal friction forces are assumed to be independent of speed. Air drag, however, is highly speed dependent and will rapidly exceed rolling drag at higher velocities [Citation126–129]. Drag characteristics can be measured in wind tunnel tests, but also modelled and optimized in respect to handcycle types and settings [Citation130]. To reduce the air friction, the frontal/lateral drag area should be reduced, which is dependent on factors like seat type and inclination, wheel type and configuration. For instance, Mannion et al. [Citation128] found that a handcycle with a time trial set-up with disc wheels has a slightly higher frontal drag area, but a substantial lower lateral drag area, when compared to a handcycle road set-up with spokes. The choice of material is again dependent on the task ahead or the speed one needs to reach.
Upper body capacity
To overcome these external power losses, the handcycle user needs to produce upper body internal work (En). During submaximal steady state exercise, the gross mechanical efficiency (GME), the ratio between the external power output (Pext) and the energy cost (or upper body capacity, En), can be considered for optimizing the handcycle performance from an exercise physiology perspective [Citation131,Citation132]. When measuring propulsion technique characteristics, these can be linked to both mechanics and physiology. GME can be used to evaluate efficiency of different modes of upper body exercise, of different interface settings, as well as effects of motor learning or training during a submaximal steady state exercise [Citation39,Citation41,Citation43,Citation100,Citation109,Citation111,Citation133–139]. Obviously, GME is also affected by individual functionality, technique, skill and talent as well as the environment (see ICF, SSC and HAAT models [Citation29,Citation31,Citation32]).
Over the past 50 years our understanding of upper body physiology has substantially improved through the lab-based work on arm crank exercise (ACE) of colleagues as Glaser [Citation140–142], Sawka [Citation92,Citation95,Citation143–148], Franklin [Citation149,Citation150], Pandolf [Citation151,Citation152], Hjeltnes [Citation153–158] and Frauendorf [Citation159–161]. They were also among the first to recognize the importance of understanding upper body work capacity and its physiology in the context of fitness and conditioning in rehabilitation practice, as is expressed in different handbooks for physiology in special populations and rehabilitation [Citation16–19,Citation26,Citation162,Citation163].
Handcycle types and settings
Besides our understanding of upper body physiology, the handcycle itself has also changed since the 1950s, when handcycles were basically converted bicycles with an asynchronous crank setting. Nowadays, the vast majority of the handcycles have a synchronous crank propulsion mode, have different gears and cranks, are light-weight and are often tuned to the task and the individual [Citation5]. This provides a wide range of different handcycle systems and settings, from daily use attach-units to fixed frame recumbent high performance sports handcycles, some with aerodynamic light weight carbon fiber frames and highly tuned to the individual athlete ().
Attach-unit handcycle
The attach-unit (or add-on) handcycle offers outdoor mobility for wheelchair users by simply attaching a crank system in front of their own handrim wheelchair, therefore, no strenuous transfer from one to another wheelchair is needed. In addition, the handcycle user does not need to make another transfer, when going inside, as the user still sits in his own wheelchair after detaching the crank set. In comparison with the handrim wheelchair, the attach-unit makes it easier to access difficult terrain and attain higher velocities that are comparable to cycling, up to 25 km/h [Citation6]. In combination with quad grips and hub-based gears, the handcycle is a good option for outdoors, also for those with a poor hand function.
Handcycle settings
Different handcycle setups are in use, depending on the user’s disability, the topography of the hometown or cycling course and the purpose of handcycling. There are many factors of the handcycle setup which can improve performance, comfort or prevent the risk for overuse, such as: body position, placement of the crank (distance and height), crank length and width, handgrip type and angle, gear setting, wheel camber and materials (). Most studies concentrate on the improvement of performance and studied the effect of a change in handcycle setup on mechanical efficiency and maximal (aerobic or sprint) power or speed production in different populations, ranging from able-bodied participants to elite athletes (). However, so far, there are no clear evidence-based guidelines on how to individually adjust the handcycle best to its user.
Figure 3. Overview of potential adjustments/configurations of a fixed frame handcycle.
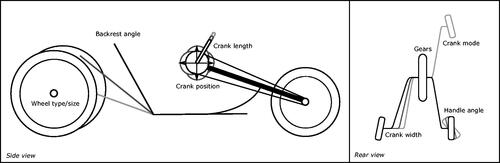
Table 2. Overview of research on handcycle dimensions.
Synchronous versus asynchronous
Synchronous handcycling was shown to be more efficient and leading to higher peak power output compared to asynchronous handcycling [Citation41,Citation100,Citation109,Citation164,Citation165]. It is assumed that greater energetic cost of asynchronous handcycling is associated to the need for increased muscular work in the upper extremities and trunk to stabilize the steering direction of the front wheel, whilst producing propulsion power. In contrast to handcycling, asynchronous arm cranking seems to be more efficient than synchronous [Citation137,Citation172–174]. In arm cranking steering is not possible, removing the need for the stability of the steering wheel. This seems to support the hypothesis that due to stabilization of the crank system asynchronous handcycling is less efficient than synchronous. So far, no detailed analyses are available to test this hypothesis. Yet, based on current research [Citation41,Citation47,Citation100,Citation109,Citation164,Citation165], we would recommend a synchronous crank mode for any form of handcycling.
Gearing/cadence
One of the benefits of handcycling is in the availability and use of (a wide variation and task-specific) gears. Gearboxes can vary in number among as less as three up to in the twenties. Using different combinations of chain wheels help to optimize towards the environmental conditions or individual work capacity even further, also in people with poor arm/hand function. At submaximal exercise levels, different gears or cadences lead to different levels of GME and physical strain at the same power output [Citation42,Citation100,Citation111,Citation136,Citation166,Citation167]. This indicates a (muscle contraction) speed and force dependency that potentially affects the overall cost of coasting as well as the force effectiveness. Gearbox range settings are extremely critical in mountainous environments for any handcyclist [Citation104]. Based on current literature, a cadence of around 50–60 rpm is recommended at submaximal level [Citation42,Citation100,Citation111,Citation165,Citation175].
Crank length
The role of crank length is also an aspect of setting with a possible mechanical advantage. For synchronous arm crank ergometry it was found that able-bodied participants could reach a higher peak power output (+12%) when the crank length increased from ±139 mm (19% of the arm length) to ±190 mm (26% of the arm length). With this increase in crank length, the optimal cadence decreases and the optimal handle speed increases [Citation169]. In a case study, in which an elite handcyclist performed tests in his own race handcycle, which was connected to a cycle ergotrainer, muscle activation in different settings was measured. It could be shown that muscle activity could be reduced by increasing the crank length from 160 mm to 175 mm, for performance at 130, 160, and 190 W [Citation176]. When considering mechanical efficiency for athletes in a recumbent sports handcycle, a crank length of 180 mm will lead to higher values compared to a length of 220 mm. For an intensity level of 90 W, it was shown that when one handcycles with a 180 mm long crank at 85 rpm, a relative increase of 19% was present over handcycling with a 220 mm long crank at 70 rpm [Citation136]. Commercially available cranks range from 150 to 220 mm in length. As a preference towards a crank length of 175–190 mm is seen [Citation136,Citation169,Citation176], we advise to keep the crank length around those values in combination with a sufficiently accommodating gear set in the context of the user and environment.
Positioning cranks/handles
Especially for recreational handcycle users, to whom maximal performance is not the main goal, an optimal handcycle-user interface should not only strive to improve performance but also contribute to lowering the risk for overuse injuries, sliding in the seat, and instability. High upper extremity ranges of motion and reaching the limits of joint excursions are considered as risk factors for repetitive strain injuries [Citation177].
The height of the crank axis is one of the settings that might contribute to this strain. When comparing the crank axis height at shoulder level with a crank axis height of shoulder level – 15% of the arm length, no effects on mechanical efficiency or shoulder load could be found in synchronous handcycle ergometry in a group of wheelchair users with spinal cord injury [Citation139]. Within an experimental set-up a crank axis height at acromion/shoulder level is often used or recommended [Citation43,Citation133,Citation177]. In practice, however, an even lower setting is used; the crank axis height at mid-sternum is often seen, especially with “bullhorn” cranks [Citation75,Citation76,Citation81].
Also, the distance of the crank axis to the shoulder was investigated for both an arm crank ergometer and a recumbent handcycle attached to an ergometer. In submaximal synchronous arm cranking, an elbow angle of 30°, with 0° being full extension, resulted in a small, but significant increase for mechanical efficiency (+0.02%), oxygen uptake (+0.03%) and ventilation (+0.05%) over 15°, as was found for both male and female able-bodied participants [Citation133]. When handcycling in a recumbent position at a mean of 61.5 W with 69 rpm, no effects of crank axis distance (elbow angle 15° vs 30°) on mechanical efficiency or shoulder load were found for wheelchair dependent persons with spinal cord injury [Citation139]. In addition, with able-bodied male participants, four different crank positions (94–97–100–103% of arm length) were tested in a recumbent position, under the submaximal conditions of 30 and 60 W with 70 rpm. As the distance of crank axis to shoulder increased, the elbow extended and the shoulder protracted. The work load is more evenly distributed in a closer crank position (94%), at which the speed fluctuations in the cycle are reduced. Mechanical efficiency, oxygen uptake and heart rate did not change across crank positions [Citation49]. In a similar study, performed with trained handcyclists however, the same four crank positions were investigated at 50 and 70% of their peak power output [Citation50]. Results showed that the upper limb kinematics differ between crank positions. In addition, at 70% of the peak power output, the oxygen consumption is more favorable for a crank position 97 or 100% of the arm length, compared to the 94 and 103% [Citation50].
Within sports, the sitting position is dependent on the classification system, in the lower classes (H1–4), i.e., for athletes with less lower limb and trunk function, a recumbent position is mandatory. In the highest class (H5), where the athlete has no restrictions in balance and trunk strength, the kneeling position is optional [Citation178]. The recumbent position allows an arm powered (AP) propulsion, as the kneeling position allows for an arm trunk powered (ATP) propulsion (). Peak power output was found to be higher for ATP, resulting in a higher physiological strain. Therefore, the gross mechanical efficiency is slightly higher during AP [Citation43].
Different handlebar angulation, crank width as well as chain ring forms have also been experimented with [Citation87,Citation179]. The handgrips should be fixed to the crank with a 30° angle (pronation of the forearm) to optimize power generation during sub-maximal handcycling [Citation53]. Additionally, Faupin et al. [Citation177], modelled different crank positions, based on 3 D kinematic measurements, in order to find the risk factors for repetitive strain injuries. They suggested that the distance between the handgrips should match shoulder width to minimize this kind of injury.
Backrest
With respect to the glenohumeral contact force and the muscle force of the infraspinatus and supraspinatus, a more upright backrest (60°) causes less load on the shoulder than a more reclined backrest (15°, 30° or 45°) [Citation139]. For daily use, a more upright backrest might be recommendable.
However, to reduce air friction, a more reclined backrest is recommended in sports. Without backrest it is possible to cycle at higher velocities than with a backrest inclination of 65° or 45° [Citation167]. This last recommendation only applies for persons with good trunk stability. Persons with high level spinal cord injury (e.g., tetraplegia or a high-level paraplegia above T6) are unable to follow this recommendation.
Limitations in the evaluation of handcycle performance
Ergometer
Arm crank ergometry tests functional capacity and allows for the analysis of a handcyclist’s physiology without the influence of bike set-up on their data. This can help monitor physiological progress over time. It can also prove useful when comparing experienced athletes with athletes who are new to the sport. Additionally, with a custom made ergometer e.g., developed by Krämer et al. [Citation180], different handcycle crank and handlebar settings could be tested, adding a different level of performance testing over commercially available ergometers. However, as in able-bodied sport, the choice of the ergometer used for physiological testing can influence the results. As arm cranking is insufficiently specific to other modes of wheeled mobility, arm crank exercise testing in itself is not a valid alternative to evaluate efficiency and/or peak or submaximal power capacity [Citation55,Citation60,Citation134,Citation146,Citation181]. Also, when using ergometers that fix the front (steering) wheel in a stable manner, the internal validity of the experiment can be questionable. As mentioned above, the possibility to steer comes with the need to stabilize the system. With an ergometer, this effort is often cancelled out. In addition, commercially available ergometers often have an asynchronous crank mode, whereas a synchronous mode is mostly seen in handcycling. For those studying handcycling, there are important methodological approaches to consider.
Participants
Many of the studies done in handcycling and discussed in this review concerns able-bodied male participants. This is a poor representation of handcycle users, as the population of individuals relying on their upper body for exercise is quite diverse.
Firstly, the female population is underrepresented in the research. For instance, for wheelchair propulsion, a difference between the sexes was found in able-bodied participants. Chaikhot et al. [Citation182] investigated 30 females and 30 males and found a lower gross mechanical efficiency, lower comfortable propulsion speed, higher local perceived exertion and higher push percentage for females compared to males. In addition, Krämer et al. [Citation53] found a difference between sexes in handcycling technique, whereas female participants tend to pull for propulsion, male push and pull. This, however, was found by accident as only three females and 12 males were tested with another aim than comparing sexes. Therefore, this should be interpreted with caution. These studies show that a difference between sexes might be present, even though it was not explicitly investigated for handcycling.
Secondly, the (level of) impairment will probably influence the physiological and biomechanical responses. Overall, more research with actual handcyclists, both in rehabilitation and sports setting, of both sexes should be stimulated.
Conclusion
Since “exercise is medicine” is an important message, it is critical that for persons reliant on upper body exercise that suitable exercise modalities are available. This review has indicated that handcycling is an appropriate exercise modality that can be used in (early) rehabilitation, for daily outdoor ambulation and recreational sports. It has been demonstrated to be feasible and easily accessible in a variety of settings and various tests can be administered. Thus, its potential should be recognized and advocated much more widely in rehabilitation and adapted sports. To optimize performance in rehabilitation, recreation and sports, a biophysical approach should be applied, optimizing both the (mechanical) interface and upper body work capacity. Continued and more systematic research is required to further stimulate handcycle use.
Disclosure statement
The authors report no conflicts of interest.
References
- Vignier N, Ravaud J, Winance M, et al. Demographics of wheelchair users in France: results of national community-based handicaps-incapacités-dépendance surveys. J Rehabil Med. 2008;40:231–239.
- Smith EM, Giesbrecht EM, Mortenson WB, et al. Prevalence of wheelchair and scooter use among community-dwelling Canadians. Phys Ther. 2016;96:1135–1142.
- LaPlante MP, Kaye HS. Demographics and trends in wheeled mobility equipment use and accessibility in the community. Assist Technol. 2010;22:3–17.
- van der Woude L, Dallmeijer AJ, Janssen TWJ, et al. Alternative modes of manual wheelchair ambulation: an Overview. Am J Phys Med Rehabil. 2001;80:765–777.
- Hettinga FJ, Valent LJ, Groen W, et al. Hand-cycling: an active form of wheeled mobility, recreation, and sports. Phys Med Rehabil Clin N Am. 2010;21:127–140.
- Hettinga FJ, de Groot S, van Dijk F, et al. Physical strain during handcycling under daily living conditions. Med Sci Sport Exerc. 2010;42:570–571. [Internet]. Available from: http://journals.lww.com/00005768-201005001-01685
- van Breukelen K. Handbiken, ongekende mogelijkheden met betrekking tot vervoer, fitness, recreatie en sport. 1999.
- van Breukelen K. Rolstoel performance: man-machine-match. Gouda (The Netherlands): Double performance; 2014.
- van den Berg-Emons RJ, Bussmann JB, Haisma JA, Sluis TA, et al. prospective study on physical activity levels after spinal cord injury during inpatient rehabilitation and the year after discharge. Arch Phys Med Rehabil. 2008;89:2094–2101.
- Ellenberg M, MacRitchie M, Franklin B, et al. Aerobic capacity in early paraplegia: implications for rehabilitation. Paraplegia. 1989;27:261–268.
- Goswami A, Ghosh AK, Ganguli S, et al. Aerobic capacity of severely disabled Indians. Ergonomics. 1984;27:1267–1269.
- de Groot S, Post MW, Hoekstra T, et al. Trajectories in the course of body mass index after spinal cord injury. Arch Phys Med Rehabil. 2014;95:1083–1092.
- Haisma JA, Bussmann JB, Stam HJ, et al. Physical fitness in people with a spinal cord injury: the association with complications and duration of rehabilitation. Clin Rehabil. 2007;21:932–940.
- Lagerström AC, Wahman K. Food and Weight. In: Lagerström AC, editor. The art of healthy living with physical impairments. Stockholm (Sweden): Spinalis, Instant Book; 2014.
- ACSM. Guidelines for exercise testing and prescription. 1995.
- Spurway N, MacLaren D, editors. Exercise Physiology in special populations. Edinburgh (UK): Churchill Livingstone Elsevier; 2008.
- Durstine JL, Moore GE. ACSM’s Exercise management for persons with chronic diseases and disabilities. Chapaign (IL): Human Kintecs, ACSM; 2003.
- Durstine JL, Painter P, Franklin BA, et al. Physical activity for the chronically ill and disabled. Sports Med. 2000;30:207–219.
- Frontera WR, Slovnik DM, Dawson DM. Exercise in rehabilitation medicine. Champaign (IL): Human Kinetics Publishers; 2006.
- Garber CE, Blissmer B, Deschenes MR, et al.; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–1359.
- Rimmer JH. Health promotion for people with disabilities: the emerging paradigm shift from disability prevention to prevention of secondary conditions. Phys Ther. 1999;79:495–502.
- Rimmer JH, Marques AC. Physical activity for people with disabilities. Lancet. 2012;380:193–195.
- Rimmer JH, Braddock D. Health promotion for people with physical, cognitive and sensory disabilities: an emerging national priority. Am J Health Promot. 2002;16:220–224.
- Anon. Official Website of the Paralympic Movement. Available from: http://www.paralympic.org/cycling
- UCI. Union Cycliste Internationale (UCI). 2015.
- Vanlandewijck YC, Thompson WR. The Paralympic Athlete. Chichester (UK): Wiley-Blackwell; 2011.
- Anon. MoveForward. [cited 2018. April 4]. Available from: http://moveforward.nu/
- Anon. Support for soldiers at the Battleback centre. RBL. [cited 2018 Apr 4]. Available from: https://www.britishlegion.org.uk/get-support/recovery/the-battle-back-centre/
- WHO. International Classification of Funtioning, Disability and Health. Geneva (Switzerland): WHO; 2001.
- van der Woude LHV, de Groot S, Janssen TWJ. Manual wheelchairs: research and innovation in rehabilitation, sports, daily life and health. Med Eng Phys. 2006;28:905–915.
- Dijk F, Dormolen M, Kompier M, et al. Herwaardering model arbeidsbelastbaarheid. TSG. 1990;68:3–10.
- Cook A, Polgar J, Encarnação P. Assistive technologies 5th edition: principles and practice. 5th ed. St. Louis (MO): Elsevier; 2020.
- Arnet U. Handcycling: a biophysical analysis. Amsterdam (The Netherlands): Vrije Universiteit; 2012.
- Groen WG, van der Woude LV, De Koning JJ. A power balance model for handcycling. Disabil Rehabil. 2010;32:2165–2171.
- van Ingen Schenau G, Ingen Schenau G. v. Cycle power: a predictive model. Endeav New Ser. 1988;12:44–47.
- van Ingen Schenau GJ. Power balance applied to speed skating. Vrije Universiteit te Amsterdam; 1981.
- van der Woude L, Veeger HE, Dallmeijer AJ, et al. Biomechanics and physiology in active manual wheelchair propulsion. Med Eng Phys. 2001;23:713–733.
- van der Woude L. Manual wheelchair propulsion: an ergonomic perspective. 1989.
- van der Woude LHV, de Groot G, Hollander AP, et al. Wheelchair ergonomics and physiological testing of prototypes. Ergonomics. 1986;29:1561–1573.
- Mason BS, van der Woude LV, Goosey-Tolfrey VL. The ergonomics of wheelchair configuration for optimal performance in the wheelchair court sports. Sports Med. 2013;43:23–38.
- Bafghi HA, de Haan A, Horstman A, et al. Biophysical aspects of submaximal hand cycling. Int J Sports Med. 2008;29:630–638.
- Kraaijenbrink C, Vegter RJK, Hensen AHR, et al. Different cadences and resistances in submaximal synchronous handcycling in able-bodied men: effects on efficiency and force application. PLoS One. 2017;12:e0183502.
- Verellen J, Meyer C, Janssens L, et al. Peak and submaximal steady-state metabolic and cardiorespiratory responses during arm-powered and arm-trunk-powered handbike ergometry in able-bodied participants. Eur J Appl Physiol. 2012;112:983–989.
- Kloosterman MGM, Eising H, Schaake L, et al. Comparison of shoulder load during power-assisted and purely hand-rim wheelchair propulsion. Clin Biomech (Bristol, Avon). 2012;27:428–435.
- Pr GCE, Jr. Levy Dietrich FD, et al. Wheelchair users’ perceptions of and experiences with power assist wheels. Am J Phys Med Rehabil. 2010;89:225–234.
- Nawoczenski DA, Clobes SM, Gore SL, et al. Three-dimensional shoulder kinematics during a pressure relief technique and wheelchair transfer. Arch Phys Med Rehabil. 2003;84:1293–1300.
- Kraaijenbrink C, Vegter RJK, Hensen AHR, et al. Biomechanical and physiological differences between synchronous and asynchronous low intensity handcycling during practice-based learning in able-bodied men. J Neuroeng Rehabil. 2020;17:29.
- Quittmann OJ, Abel T, Albracht K, et al. Biomechanics of all-out handcycling exercise: kinetics, kinematics and muscular activity of a 15-s sprint test in able-bodied participants. Sport Biomech. [Internet]. 2020 May 7 [cited 2020 May 8]:[1–24]. Available from: https://www.tandfonline.com/doi/full/https://doi.org/10.1080/14763141.2020.1745266
- Vegter RJK, Mason BS, Sporrel B, et al. Crank fore-aft position alters the distribution of work over the push and pull phase during synchronous recumbent handcycling of able-bodied participants. PLoS One. 2019;14:e0220943
- Stone B, Mason BS, Warner MB, et al. Horizontal crank position affects economy and upper limb kinematics of recumbent handcyclists. Med Sci Sport Exerc. 2019;51:2265–2273.
- Verellen J, Meyer C, Reynders S, et al. Consistency of within-cycle torque distribution pattern in hand cycling. J Rehabil Res Dev. 2008;45:1295–1302.
- Arnet U, van Drongelen S, van der Woude LH, et al. Shoulder load during handcycling at different incline and speed conditions. Clin Biomech (Bristol, Avon). 2012;27:1–6.
- Krämer C, Schneider G, Böhm H, et al. Effect of different handgrip angles on work distribution during hand cycling at submaximal power levels. Ergonomics. 2009;52:1276–1286.
- Quittmann OJ, Abel T, Albracht K, et al. Reliability of muscular activation patterns and their alterations during incremental handcycling in able-bodied participants. Sport Biomech. 2019.
- Arnet U, Drongelen S, Scheel-Sailer A, et al. Shoulder load during synchronous handcycling and handrim wheelchair propulsion in persons with paraplegia. J Rehabil Med. 2012;44:222–228.
- Van Drongelen S, Schlüssel M, Arnet U, et al. The influence of simulated rotator cuff tears on the risk for impingement in handbike and handrim wheelchair propulsion. Clin Biomech (Bristol, Avon). 2013;28:495–501.
- Praagman M, Stokdijk M, Veeger HEJ, et al. Predicting mechanical load of the glenohumeral joint, using net joint moments. Clin Biomech (Bristol, Avon). 2000;15:315–321.
- Nikooyan AA, Veeger HE, Chadwick EK, et al. Development of a comprehensive musculoskeletal model of the shoulder and elbow. Med Biol Eng Comput. 2011;49:1425–1435.
- Veeger HEJ, Rozendaal LA, Van der Helm FCT. Load on the shoulder in low intensity wheelchair propulsion. Clin Biomech (Bristol, Avon). 2002;17:211–218.
- Dallmeijer AJ, Zentgraaff IDB, Zijp NI, et al. Submaximal physical strain and peak performance in handcycling versus handrim wheelchair propulsion. Spinal Cord. 2004;42:91–98.
- Hettinga FJ, de Groot S, van Dijk F, et al. Physical strain of handcycling: an evaluation using training guidelines for a healthy lifestyle as defined by the American College of Sports Medicine. J Spinal Cord Med. 2013;36:376–382.
- Nash MS. Exercise as a health-promoting activity following spinal cord injury. J Neurol Phys Ther. 2005;29:87–106.
- Nooijen CF, Stam HJ, Bergen MP, et al.; Act-Active Research Group. A behavioural intervention increases physical activity in people with subacute spinal cord injury: a randomised trial. J Physiother. 2016;62:35–41.
- de Groot S, Post MW, Snoek GJ, et al. Longitudinal association between lifestyle and coronary heart disease risk factors among individuals with spinal cord injury. Spinal Cord. 2013;51:314–318.
- Hoekstra S, Valent L, Gobets D, et al. Effects of four-month handbike training under free-living conditions on physical fitness and health in wheelchair users. Disabil Rehabil. 2017;39:1581–1588.
- Martin Ginis KA, Van Der Scheer JW, Latimer-Cheung AE, et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018;56:308–321.
- Valent LJ, Dallmeijer AJ, Houdijk H, et al. Influence of hand cycling on physical capacity in the rehabilitation of persons with a spinal cord injury: a longitudinal cohort study. Arch Phys Med Rehabil. 2008;89:1016–1022.
- Knechtle B, Müller G, Knecht H. Optimal exercise intensities for fat metabolism in handbike cycling and cycling. Spinal Cord. 2004;42:564–572.
- Short KR, Teague AM, Klein JC, et al. The effect of handcycle ergometer exercise on glucose tolerance in ambulatory and non-ambulatory adolescents. Pediatr Exerc Sci. 2017;29:63–72.
- Nooijen CF, van den Brand IL, ter Horst P, et al. Feasibility of handcycle training during inpatient rehabilitation in persons with spinal cord injury. Arch Phys Med Rehabil. 2015;96:1654–1657.
- Mukherjee G, Bhowmik P, Samanta A. Physical fitness training for wheelchair ambulation by the arm crank propulsion technique. Clin Rehabil. 2001;15:125–132.
- Abel T, Kröner M, Rojas VS, et al. Energy expenditure in wheelchair racing and handbiking - a basis for prevention of cardiovascular diseases in those with disabilities. Eur J Cardiovasc Prev Rehabil. 2003;10:371–376.
- Babu Rajendra Kurup N, Puchinger M, Gföhler M. Forward dynamic optimization of handle path and muscle activity for handle based isokinetic wheelchair propulsion: a simulation study. Comput Methods Biomech Biomed Engin. 2019;22:55–63.
- Bresnahan JJ, Farkas GJ, Clasey JL, et al. Arm crank ergometry improves cardiovascular disease risk factors and community mobility independent of body composition in high motor complete spinal cord injury. J Spinal Cord Med. 2019;42:272–280.
- Brizuela G, Sinz S, Aranda R, et al. The effect of arm-crank exercise training on power output, spirometric and cardiac function and level of autonomy in persons with tetraplegia. Eur J Sport Sci. 2019.
- Valent LM, Dallmeijer AJ, Houdijk H, et al. Effects of hand cycle training on physical capacity in individuals with tetraplegia: a clinical trial. Phys Ther. 2009;89:1051–1060.
- Valent LJM. The effects of hand cycling on physical capacity in persons with spinal cord injury [dissertation]. Vrije Universiteit Amsterdam; 2009.
- Barton J, Pretty J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ Sci Technol. 2010;44:3947–3955.
- Pretty J, Peacock J, Sellens M, et al. The mental and physical health outcomes of green exercise. Int J Environ Health Res. 2005;15:319–337.
- Barton J, Griffin M, Pretty J. Exercise-, nature- and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect Public Health. 2012;132:89–96.
- Valent L, Dallmeijer A, Houdijk H, et al. Effects of hand cycle training on wheelchair capacity during clinical rehabilitation in persons with a spinal cord injury. Disabil Rehabil. 2010;32:2191–2200.
- Hettinga FJ, Hoogwerf M, van der Woude LV. Handcycling: training effects of a specific dose of upper body endurance training in females. Eur J Appl Physiol. 2016;116:1387–1394.
- de Groot S, Kouwijzer I, Baauw M, HandbikeBattle, et al. Effect of self-guided training for the HandbikeBattle on body composition in people with spinal cord injury. Spinal Cord Ser Cases. 2018;4:79.
- Abreu E. M d C, Alves R. d S, Borges ACL, et al. Autonomic cardiovascular control recovery in quadriplegics after handcycle training. J Phys Ther Sci. 2016;28:2063–2068.
- Schoenmakers P, Reed K, Van Der Woude L, et al. High intensity interval training in handcycling: the effects of a 7 week training intervention in able-bodied men. Front Physiol. 2016;7:638.
- Krops L, Albada T, Woude L, et al. Anaerobic exercise testing in rehabilitation: a systematic review of available tests and protocols. J Rehabil Med. 2017;49:289–303.
- Zeller S, Abel T, Smith PM, et al. Influence of noncircular chainring on male physiological parameters in hand cycling. J Rehabil Res Dev. 2015;52:211–220.
- Kouwijzer I, Nooijen C, Breukelen K, et al. Effects of push-off ability and handcycle type on handcycling performance in able-bodied participants. J Rehabil Med. 2018;50:563–568.
- Hutzler Y. Anaerobic fitness testing of wheelchair users. Sports Med. 1998;25:101–113.
- Balmer J, Davison RCR, Coleman DA, et al. The validity of power output recorded during exercise performance tests using a Kingcycle air-braked cycle ergometer when compared with an SRM powermeter. Int J Sport Med. 2000;21:195–199.
- Vogt S, Heinrich L, Schumacher YO, et al. Power output during stage racing in professional road cycling. Med Sci Sports Exerc. 2006;38:147–151.
- Sawka MN, Glaser RM, Laubach LL, et al. Wheelchair exercise performance of the young, middle-aged, and elderly . J Appl Physiol Respir Environ Exerc Physiol. 1981;50:824–828.
- Smith PM, McCrindle E, Doherty M, et al. Influence of crank rate on the slow component of pulmonary O2 uptake during heavy arm-crank exercise. Appl Physiol Nutr Metab. 2006;31:292–301.
- Abel T, Burkett B, Thees B, et al. Effect of three different grip angles on physiological parameters during laboratory handcycling test in able-bodied participants. Front Physiol. 2015;6:331.
- Sawka MN, Foley ME, Pimental NA, et al. Physiological factors affecting upper body aerobic exercise. Ergonomics. 1983;26:639–646.
- Talbot C, Kay TD, Walker N, et al. A comparison of two anaerobic test measurement systems using an upper body Wingate test. Res Sport Med. 2014;22:265–275.
- Wicks JR, Oldridge NB, Cameron BJ, et al. Arm cranking and wheelchair ergometry in elite spinal cord-injured athletes. Med Sci Sports Exerc. 1983;15:224–231.
- Meyer C, Weissland T, Watelain E, et al. Physiological responses in handcycling. Preliminary study. Ann Phys Rehabil Med. 2009;52:311–318.
- Jacobs PL, Mahoney ET, Johnson B. Reliability of arm Wingate anaerobic testing in persons with complete paraplegia. J Spinal Cord Med. 2003;26:141–144.
- van der Woude L, Bosmans I, Bervoets B, et al. Handcycling: different modes and gear ratios. J Med Eng Technol. 2000;24:242–249.
- VanSumeren A, Bye T, Kilgas M, et al. Influence of the lower body on seated arm cranking performance. Int J Sports Med. 2018;39:757–763.
- Miles DS, Sawka MN, Glaser RM, et al. Plasma volume shifts during progressive arm and leg exercise. J Appl Physiol Respir Environ Exerc Physiol. 1983;54:491–495.
- Balmer J, Bird SR, Davison RR, et al. Mechanically braked Wingate powers: agreement between SRM, corrected and conventional methods of measurement. J Sports Sci. 2004;22:661–667.
- de Groot S, Postma K, van Vliet L, et al. Mountain time trial in handcycling: exercise intensity and predictors of race time in people with spinal cord injury. Spinal Cord. 2014;52:455–461.
- Pitetti KH, Snell PG, Stray-Gundersen J. Maximal response of wheelchair-confined subjects to four types of arm exercise. Arch Phys Med Rehabil. 1987;68:10–13.
- Kouwijzer I, Valize M, Valent LJM, et al. The influence of protocol design on the identification of ventilatory thresholds and the attainment of peak physiological responses during synchronous arm crank ergometry in able-bodied participants. Eur J Appl Physiol. 2019;119:2275–2212.
- Leicht AS, Spinks WL. Effect of shoulder angle on physiological responses during incremental peak arm crank ergometry. J Sports Sci. 2007;25:443–452.
- Walker R, Powers S, Stuart MK. Peak oxygen uptake in arm ergometry: effects of testing protocol. Br J Sports Med. 1986;20:25–26.
- van der Woude L, Horstman A, Faas P, et al. Power output and metabolic cost of synchronous and asynchronous submaximal and peak level hand cycling on a motor driven treadmill in able-bodied male subjects. Med Eng Phys. 2008;30:574–580.
- Kouwijzer I, Valent L, Osterthun R, et al.; Group on behalf of the H. Peak power output in handcycling of individuals with a chronic spinal cord injury: predictive modeling, validation and reference values. Disabil Rehabil. 2020;42:400–409.
- Verellen J, Theisen D, Vanlandewijck Y. Influence of crank rate in hand cycling. Med Sci Sports Exerc. 2004;36:1826–1831.
- Anon. HandbikeBattle. Overwinnen! [cited 2018 Apr 4]. Available from: http://handbikebattle.nl/
- Van Leeuwen CMC, Verwer J, Van Koppenhagen CF, et al. Trainen voor de HandbikeBattle: mentale effecten; De eerste resultaten van de HandbikeBattle. Ned Tijdschr Revalidatiegeneeskd. 2014;36:104–107.
- Groot S, Hoekstra S, Comtesse P, et al. Relationships between internal and external handcycle training load in people with spinal cord injury training for the handbikebattle. J Rehabil Med. 2018;50:261–268.
- Bertucci W, Duc S, Villerius V, et al. Validity and reliability of the PowerTap Mobile Cycling Powermeter when compared with the SRM device. Int J Sports Med. 2005;26:868–873.
- Gardner AS, Stephens S, Martin DT, et al. Accuracy of SRM and power tap power monitoring systems for bicycling. Med Sci Sports Exerc. 2004;36:1252–1258.
- Bertucci W, Grappe F, Girard A, et al. Effects on the crank torque profile when changing pedalling cadence in level ground and uphill road cycling. J Biomech. 2005;38:1003–1010.
- Abel T, Burkett B, Schneider S, et al. The exercise profile of an ultra-long handcycling race: the Styrkeprøven experience. Spinal Cord. 2010;48:894–898.
- Nimmerichter A, Eston RG, Bachl N, et al. Longitudinal monitoring of power output and heart rate profiles in elite cyclists. J Sports Sci. 2011;29:831–840.
- Rice I, Hettinga FJ, Laterrier J, et al. Biomechanics. In: Vanlandewijck Y, Thompson W, editors. The Paralympic athlete. Chichester (UK): Wiley-Blackwell; 2011. p. 33–50.
- Kauzlarich J. Wheelchair rolling resistance and tire design. In: van der Woude L, Hopman M, van Kemenda C, editors. Biomedical aspects of manual wheelchair propulsion: the state of the art III. Assistive technology research series. Amsterdam (The Netherlands): IOS press; 1999. p. 158–172.
- van der Woude L, Geurts C, Winkelman H, et al. Measurement of wheelchair rolling resistance with a handle bar push technique. J Med Eng Technol. 2003;27:249–258.
- Frank T, Abel E. Drag forces in wheelchairs. In: van der Woude L, Meijs P, Van der Grinten B, De Boer Y, editors. Ergonomics of manual wheelchair propulsion; state of the art. Concerned action “mobility restoration for paralyzed persons”. Amsterdam (The Netherlands): IOS press; 1993. pp 255–267.
- Wilson DG, Papadopoulos J, Whitt FR. Bicycling science. 3rd ed. Cambridge (MA): MIT Press; 2004.
- de Groot S, Zuidgeest M, van der Woude LV. Standardization of measuring power output during wheelchair propulsion on a treadmill Pitfalls in a multi-center study. Med Eng Phys. 2006;28:604–612.
- de Groot G, Sargeant A, Geysel J. Air friction and rolling resistance during cycling. Med Sci Sports Exerc. 1995;27:1090–1095.
- Mannion P, Toparlar Y, Hajdukiewicz M, et al. Aerodynamics analysis of wheel configurations in Paralympic hand-cycling: a computational study. Eur J Mech - B/Fluids. 2019;76:50–65.
- Mannion P, Toparlar Y, Blocken B, et al. Analysis of crosswind aerodynamics for competitive hand-cycling. J Wind Eng Ind Aerodyn. 2018;180:182–190.
- Mannion P, Toparlar Y, Clifford E, et al. The impact of arm-crank position on the drag of a paralympic hand-cyclist. Comput Methods Biomech Biomed Engin. 2019;22:386–395.
- Belloli M, Cheli F, Bayati I, et al. Handbike aerodynamics: wind tunnel versus track tests. Proc Eng. 2014;72:750–755.
- Gaesser G, Brooks GA. Muscular efficiency during steady-rate exercise: effects of speed and work rate. J Appl Physiol. 1975;38:1132–1139.
- Powers SK, Beadle RE, Mangum M. Exercise efficiency during arm ergometry: effects of speed and work rate. J Appl Physiol Respir Environ Exerc Physiol. 1984;56:495–499.
- van Drongelen S, Maas JC, Scheel-Sailer A, et al. Submaximal arm crank ergometry: effects of crank axis positioning on mechanical efficiency, physiological strain and perceived discomfort. J Med Eng Technol. 2009;33:151–157.
- Romkes J, Groen BE, Koning JJ. Mechanical efficiency in arm cranking exercise. In: Van der Woude L, Hopman M, Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: the state of the art II. Vol. 5. Amsterdam (The Netherlands): IOS press; 1999. p 172–175.
- Lovell D, Shields D, Beck B, et al. The aerobic performance of trained and untrained handcyclists with spinal cord injury. Eur J Appl Physiol. 2012;112:3431–3437.
- Goosey-Tolfrey VL, Alfano H, Fowler N. The influence of crank length and cadence on mechanical efficiency in hand cycling. Eur J Appl Physiol. 2007;102:189–194.
- Goosey-Tolfrey VL, Sindall P. The effects of arm crank strategy on physiological responses and mechanical efficiency during submaximal exercise. J Sports Sci. 2007;25:453–460.
- Arnet U, Marchetto P, van der Woude LV, et al. Propulsion style and mechanical efficiency during handcycling at different power outputs. In: Arnet U, editor. Handcycling: a biophysical analysis. Wageningen (The Netherlands): Ponsen & Looijen B. V.; 2012. p. 88–99.
- Arnet U, van Drongelen S, Schlussel M, et al. The effect of crank position and backrest inclination on shoulder load and mechanical efficiency during handcycling. Scand J Med Sci Sports. 2014;24:386–394.
- Glaser RM, Sawka MN, Brune MF, et al. Physiological responses to maximal effort wheelchair and arm crank ergometry. J Appl Physiol Respir Environ Exerc Physiol. 1980;48:1060–1064.
- Glaser RM, Sawka MN, Durbin RJ, et al. Exercise program for wheelchair activity. Am J Phys Med. 1981;60:67–75.
- Smith PA, Glaser RM, Petrofsky JS, et al. Arm crank vs handrim wheelchair propulsion: metabolic and cardiopulmonary responses. Arch Phys Med Rehabil. 1983;64:249–254.
- Sawka MN, Gonzalez RR, Drolet LL, et al. Heat exchange during upper- and lower-body exercise. J Appl Physiol Respir Environ Exerc Physiol. 1984;57:1050–1054.
- Sawka MN, Pimental NA, Pandolf KB. Thermoregulatory responses to upper body exercise. Eur J Appl Physiol Occup Physiol. 1984;52:230–234.
- Sawka MN, Miles DS, Petrofsky JS, Wilde SW, et al. Ventilation and acid-base equilibrium for upper-body and lower-body exercise. Aviat Sp Environ Med. 1982;53:354–359.
- Sawka MN, Glaser RM, Wilde SW, et al. Metabolic and circulatory responses to wheelchair and arm crank exercise. J Appl Physiol Respir Environ Exerc Physiol. 1980;49:784–788.
- Sawka MN, Foley ME, Pimental NA, et al. Determination of maximal aerobic power during upper-body exercise. J Appl Physiol Respir Environ Exerc Physiol. 1983;54:113–117.
- Sawka MN. Physiology of upper body exercise. Exerc Sport Sci Rev. 1986;14:175–211.
- Franklin BA. Exercise testing, training and arm ergometry. Sports Med. 1985;2:100–119.
- Franklin BA, Scherf J, Pamatmat A, et al. Arm exercise testing and training. Pract Cardiol. 1982;8:43–70.
- Pandolf KB. Local and central factor contribution in the perception of effort during physical exercise. In: Borg G, Ottoson D, editors. The perception of exertion in physical work. London (UK): Palgrave Macmillan; 1986.
- Pandolf KB, Billings DS, Drolet LL, et al. Differential ratings of perceived exertion and various physiological responses during prolonged upper and lower body exercise. Eur J Appl Physiol Occup Physiol. 1984;53:5–11.
- Hjeltnes N, Stanghelle JK, Skyberg D. Pulmonary function and oxygen uptake during exercise in 16 year old boys with cystic fibrosis. Acta Paediatr Scand. 1984;73:548–553.
- Hjeltnes N. Cardiorespiratory capacity in tetra- and paraplegia shortly after injury. Scand J Rehabil Med. 1986;18:65–70.
- Hjeltnes N. Capacity for physical work and training after spinal injuries and strokes. Scand J Soc Med Suppl. 1982;29:245–251.
- Hjeltnes N, Vokac Z. Circulatory strain in everyday life of paraplegics. Scand J Rehabil Med. 1979;11:67–73.
- Hjeltnes N. [Physical work capacity and training after spinal cord injuries and cerebrovascular accidents]. Tidsskr. Nor. Laegeforen. 1980;100:862–866.
- Hjeltnes N. Oxygen uptake and cardiac output in graded arm exercise in paraplegics with low level spinal lesions. Scand J Rehabil Med. 1977;9:107–113.
- Frauendorf H, Kobryn U, Gelbrich W, et al. Changes of the EMG and its relationship to the cardiopulmonary parameters during two-arm cranking of disabled men. Biomed Biochim Acta. 1989;48:S521–S524.
- Frauendorf H, Kobryn U, Hoffmann B, et al. Sex- and age-related behaviour of the integrated EMG during one-arm cranking. Biomed Biochim Acta. 1986;45:85–87.
- Frauendorf H, Gelbrich W, Kobryn U. [Reactions of the cardiopulmonary and the motor system in work with medium-sized muscles]. Z Gesamte Hyg. 1990;36:357–360.
- Goosey-Tolfrey V. Wheelchair sport: a complete guide for athletes, coaches, and teachers. Chaimpaign (IL): Human Kinetics; 2010.
- Abel T, Vanlandewijck Y, Verellen J. Handcyling. In: Goosey-Tolfrey VL, editor. Wheelchair sport, a complete guide for athletes, coaches, and teachers. Chaimpaign (IL): Human Kinetics; 2010. pp 187–197.
- Abel T, Vega SR, Bleicher I, et al. Handbiking: physiological responses to synchronous and asynchronous crank montage. Eur J Sport Sci. 2003;3:1–9.
- Dallmeijer AJ, Ottjes L, de Waardt E, et al. A physiological comparison of synchronous and asynchronous hand cycling. Int J Sports Med. 2004;25:622–626.
- Faupin A, Gorce P, Campillo P, et al. Kinematic analysis of handbike propulsion in various gear ratios: implications for joint pain. Clin Biomech (Bristol, Avon). 2006;21:560–566.
- Faupin A, Gorce P, Meyer C, et al. Effects of backrest positioning and gear ratio on nondisabled subjects’ handcycling sprinting performance and kinematics. JRRD. 2008;45:109–116.
- Faupin A, Gorce P, Meyer C. Effects of type and mode of propulsion on hand-cycling biomechanics in nondisabled subjects. JRRD. 2011;48:1049–1060.
- Krämer C, Hilker L, Böhm H. Influence of crank length and crank width on maximal hand cycling power and cadence. Eur J Appl Physiol. 2009;106:749–757.
- Litzenberger S, Mally F, Sabo A. Biomechanics of elite recumbent handcycling: a case study. Sports Eng. 2016;19:201–211.
- Weissland T, Pelayo P, Vanvelcenaher J, et al. Physiological effects of variations in spontaneously chosen crank rate during incremental upper-body exercise. Eur J Appl Physiol Occup Physiol. 1997;76:428–433.
- Hopman MTE, van Teeffelen WM, Brouwer J, et al. Physiological responses to asynchronous and synchronous arm-cranking exercise. Eur J Appl Physiol Occup Physiol. 1995;72:111–114.
- Mossberg K, Willman C, Topor M, et al. Comparison of asynchronous versus synchronous arm crank ergometry. Spinal Cord. 1999;37:569–574.
- Smith PM, Chapman ML, Hazlehurst KE, et al. The influence of crank configuration on muscle activity and torque production during arm crank ergometry. J Electromyogr Kinesiol. 2008;18:598–605.
- Foss Ø, Hallén J. The most economical cadence increases with increasing workload. Eur J Appl Physiol. 2004;92:443–451.
- Litzenberger S, Mally F, Sabo A. Influence of different seating and crank positions on muscular activity in elite handcycling – a case study. Procedia Eng. 2015;112:355–360.
- Faupin A, Gorce P. The effects of crank adjustments on handbike propulsion: a kinematic model approach. Int J Ind Ergon. 2008;38:577–583.
- Union Cycliste Internationale. UCI Cycling Regulations. 2016. p. 1–81.
- Zipfel E, Olson J, Puhlman J, et al. Design of a custom racing hand-cycle: review and analysis. Disabil Rehabil Assist Technol. 2009;4:119–128.
- Krämer DC. Ergonomische Optimierung des Handbike-Antriebes [dissertation]. 2012.
- Smith P, Doherty M, Price M. The effect of crank rate on physiological responses and exercise efficiency using a range of submaximal workloads during arm crank ergometry. Int J Sports Med. 2005;27:199–204.
- Chaikhot D, Taylor MJD, Hettinga FJ. Sex differences in wheelchair propulsion biomechanics and mechanical efficiency in novice young able-bodied adults. Eur J Sport Sci. 2018;18:650–658.