
Abstract
Purpose
Self-regulation refers to self-management and self-control, with or without disability. Outcomes of rehabilitation with respect to self-regulation are unclear. This study aims to identify elements of self-regulation that former patients consider important in the context of medical rehabilitation.
Materials and methods
Qualitative exploration based on focus group discussions (FGDs). Transcripts were analysed using thematic analysis as well as open coding. Forty individuals participated in seven diagnosis-related FGDs.
Results
Six subthemes were raised in the FGDs which could be merged into three main themes. Two main themes are conditional for regaining self-regulation: 1) having insight into one’s condition and abilities (i.e., insight into impairments. consequences of impairments. abilities); 2) to know how to cope with the consequences of the condition (be able to communicate limitations; have to trust in body and functioning). The subject of the last theme 3) is how to apply self-regulation in one’s own life (to make use of abilities and optimize functioning).
Conclusions
Three main themes of self-regulation in the context of medical rehabilitation were identified by former patients, partly relating to the ability to self-regulate and partly to the execution of self-regulation. This knowledge can be used to define specific rehabilitation goals and further develop rehabilitation outcome measurement.
Awareness of the fundamental subthemes of self-regulation in rehabilitation will positively contribute to theory building and improve clinical practice (e.g., goal setting).
Paying explicit attention to the six subthemes as standard elements of rehabilitation will help to provide a comprehensive view concerning self-regulation.
The conceptual model of self-regulation, based on patient perspectives, can contribute to the measurement of rehabilitation outcomes.
IMPLICATIONS FOR REHABILITATION
Introduction
In the Netherlands, about 200,000 adults make use of medical rehabilitation services annually, because of illness, an accident or congenital disease [Citation1]. Major diagnostic groups in rehabilitation are musculoskeletal disorders, stroke, traumatic brain injury, spinal cord injury, neurological and neuromuscular diseases, and chronic pain disorder. Rehabilitation treatment enables persons with chronic health conditions and disabilities to achieve and maintain optimal functioning when interacting with their environment [Citation2,Citation3], and thereby optimize their independence and autonomy [Citation4,Citation5]. Research has shown that effective rehabilitation consists of at least two types of interventions: 1) exercise, and 2) self-management and education [Citation6]. Self-management and education interventions include education about the condition and managing the symptoms, and psychosocial support to cope adequately with the emotional aspects of the illness [Citation6]. Rehabilitation goals are already often focused on optimizing participation and learning self-management. Self-management is often seen as an element of self-regulation; it ties in with the educational approach of rehabilitation [Citation7].
Self-regulation is a complex concept with diverging definitions and meanings [Citation8–11]. However, there appears to be a common understanding of self-regulation as a continuously active process of managing and changing the self. According to Bandura, self-regulation involves three components: 1) self-monitoring of own behaviour, emotional reactions, thought patterns and own successes and failures; 2) judgement of own behaviour according to own personal standards and broader contextual standards; and, 3) reactions to own behaviour [Citation12]. Self-regulation, according to all definitions, enables a person to make his/her own choices and to have self-control, thus positively contributing to participation in life and autonomy after rehabilitation [Citation13].
The term self-regulation is widely used throughout medical rehabilitation practice and in relation to chronic health conditions [Citation7,Citation11,Citation14,Citation15]. Also, specific self-regulation interventions have been described in the rehabilitation literature, all of which seem to influence self-regulation levels positively [Citation16,Citation17]. Nevertheless, unlike functional status, participation, or health-related quality of life, outcomes of rehabilitation with respect to self-regulation are not regularly measured and hence largely unknown. Consequently, it is not clear what rehabilitation can add to regaining self-regulation, nor how rehabilitation interventions can be made more effective. Furthermore, it is not clear which of the many instruments for measuring self-regulation [Citation10,Citation11], or related concepts such as self-insight [Citation12], self-efficacy [Citation13,Citation14], or self-awareness [Citation15–17], are most useful for this goal. To be able to identify an instrument that measures self-regulation outcomes of rehabilitation, it is important to know what is important or desirable about self-regulation in the context of medical rehabilitation, according to the rehabilitation patient. This study aims, therefore, to identify elements of self-regulation that former patients consider to be a requirement in the context of medical rehabilitation. A qualitative design was used as the goal of the study was to collect and explore patient perspectives.
Material and methods
Design
Subjective concepts, such as self-regulation, cannot be directly observed [Citation18]. To translate the abstract concept of self-regulation into a measurable element, a concrete conceptual model should be devised that sufficiently reflects the perspectives of rehabilitation patients. As it was not known which elements would be mentioned as important by former patients, a qualitative approach was deemed appropriate. For this study, focus group discussions (FGDs) with former rehabilitation patients were organised. FGDs help in the understanding of individual perspectives, as well as of perceptions resulting from the interaction between participants [Citation19]. The FGDs were conducted with the aim of discovering former patients’ perspectives and priorities concerning self-regulation as an outcome of rehabilitation, using a structured procedure of interpretation. The “consolidated criteria for reporting qualitative research” (COREQ) were applied in the description of this qualitative research [Citation20].
Selection of participants for the FGDs
Purposive sampling was used. Individuals were included who had undergone a rehabilitation program between 2012 and 2017. The rehabilitation population was defined as persons who had a diagnosis covered by one of the main diagnostic groups in Dutch medical rehabilitation: 1) amputation, 2) neurological diseases (including neuromuscular diseases), 3) chronic pain disorder, 4) musculoskeletal disorder, 5) spinal cord injury, or 6) acquired brain injury [Citation1]. We added the diagnostic group on 7) oncology, due to the increasing number of rehabilitation patients within this population [Citation21]. In addition, they had to be at least 18 years old at the start of their rehabilitation trajectory. Individuals with insufficient knowledge of the Dutch language were excluded. Variation with respect to age, gender, educational background, marital status, ethnic background, and inpatient or outpatient trajectory was aimed for.
Procedure
Recruitment was carried out via patient organisations, social media and internal recruitment (via letters of invitation to former patients) among former patients of De Hoogstraat Rehabilitation center. Six large patient organizations were contacted, each representing a different diagnostic group in the Netherlands. Each organization was asked to distribute the invitation to their members, directly via e-mail or via their online newsletter. We called all individuals who indicated an interest in participating in the study by phone, to provide more information and assess their eligibility. No relationship with the participants was established prior to the FGDs and one pilot FGD was conducted. This pilot was organized to test the topic guide and to familiarize the moderator with the tasks. This did not lead to changes in the contents of the topic list. Seven FGDs were held between December 2019 and April 2020 at De Hoogstraat Rehabilitation center, due to its accessibility and a central location within the country. The number of seven FGDs was set a-priori, one for each diagnostic group. The aim was to include 49 participants (seven persons per diagnostic group). Each person could join the FGD once. They were conducted face-to-face in the Dutch language and audiotaped. All FGDs lasted 2 hours. They were moderated by the first author (female) and attended by an intern who kept track of the time and took field notes. One intern attended the first three FGDs; another the last four (both female). The last author (male) of this article attended the first two FGDs as a second moderator. Both moderators are experienced in qualitative data collection in the field of rehabilitation. All authors primarily involved in the content analysis are experienced in qualitative research as being from diverse backgrounds (nursing, health sciences, psychology).
Topic guide and element list
A topic guide containing the main questions was created by the authors and was used in all the FGDs to ensure the same format (Supplementary Appendix A). Questions were open and aimed at giving direction to the discussion of interest. Clarifications were asked when needed. Examples of questions were about respondents’ rehabilitation background, what the main impact was of rehabilitation on their lives, what the term self-regulation meant to them, and how they experienced self-regulation during rehabilitation. After a short break, we asked respondents to reflect on a list of 22 elements that could reflect self-regulation. The list was created by the researchers based on an exploratory literature search. This search used the term “self-regulation” and the related terms “self-determination,” “choice and control,” “autonomy,” and “self-insight.” Definitions and explanations of these keywords were unravelled by writing down all underlying elements mentioned in the publications retrieved. The researchers merged elements that were similar, and structured these into an understandable list, as shown in Supplementary Appendix B. Participants were asked to rate the importance of each element for self-regulation to facilitate the FGD. The study was bottom-up and themes of self-regulation were not pre-established.
Data management and content analysis
All audiotapes were transcribed verbatim and anonymized. Data analyses were performed by two separate researchers, using MaxQDA software (Verbi Gmbh MaxQDA 2018.2). Thematic analysis, as well as open coding, were used for content analysis. Prior to coding, an initial coding tree was created based on the item list. The codes “important” (when the participant ranked the item with one or two), “neutral” (when the item was ranked with a three), and “not important” (when the item was ranked with a four or five) were added to classify quotes. Additional codes were created, evaluated, and refined for new elements emerging from the FGDs. Disagreements were discussed by the two researchers, and in some cases with a third researcher, until consensus was reached. Finally, all researchers attended a meeting to discuss the results in order to arrive at a final consensus.
Data quality assurance
The criteria used to determine the rigor of the study included the credibility, transferability, dependability, and conformability of the data [Citation22]. To ensure data credibility, the codes and themes that were used and the results that were obtained were discussed with four researchers, until consensus was reached. Furthermore, all results were discussed with an advisory board, consisting of rehabilitation researchers, managers, medical doctors, and representatives of patient organizations. They expressed the same understanding and interpretation of the results. Lastly, quotes of participants were used in the final report. Transferability was ensured by providing a transparent description of the study setting, including all main diagnostic groups and persons of different ages and backgrounds. To ensure data dependability, a study protocol was devised prior to embarking on the study. Furthermore, accurate documentation was provided of the research methods, of all changes and revisions, and of all the results. To maintain the conformability of the findings, probes were used to obtain detailed information on responses. We used a fixed structure for all FGDs. Field notes and audio recordings were collected for all FGDs to overcome biases.
Statement of ethics
The study protocol was reviewed by the ethics committee of the University Medical Center of Groningen; it was declared that this study did not require approval according to Dutch law (registration number 201800582). The board of De Hoogstraat Rehabilitation center provided approval for study execution. Written informed consent was obtained from all participants.
Results
Sixty-two former patients agreed to participate in the FGDs, 40 of whom participated in one of the seven FGDs. Due to personal reasons, fifteen former patients cancelled their participation a few days, up to a few hours, before the start of the FGD. Seven persons failed to show up. One participant was not able to join the FGD and agreed to participate in an additional one-to-one interview. Five partners who had accompanied the patient to the location, for any reason, attended the FGD. Partners were asked not to participate actively during the FGD. Characteristics of the participants can be found in . Participants from each of the seven diagnostic groups were included. Examples of health conditions included were chronic pain disorder: back pain (n = 1); neurology: Guillian barré (n = 3); musculoskeletal disorder: multi-trauma (n = 5); acquired brain injury: trauma (n = 4), and stroke (n = 2); oncology: breast cancer (n = 5); amputation: lower leg (n = 3); and spinal cord injury: paraplegia (n = 2).
Table 1. Sociodemographic characteristics of the study population.
Self-regulation conceptualized
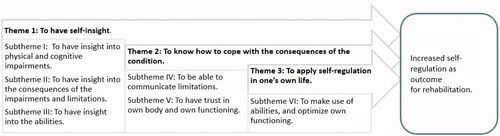
In addition to the 22 elements, the participants mentioned eleven new elements as being related to self-regulation. From this long list, the majority were coded as important. Those which were not considered important were omitted. Elements coded as important were combined when they were related to each other. Six subthemes stood out which could be merged into three main themes: 1) having self-insight into one’s condition and abilities; 2) to know how to cope with the consequences of the condition; 3) to apply self-regulation in one’s own life, as displayed in . Overall, participants stressed the importance of understanding themselves again. They emphasised that regaining their self-regulation after rehabilitation is an iterative process of self-reflection and trial and error. Although there were differences in age, stage of life, and degree of impairment, agreement was found throughout all FGDs concerning all subthemes.
Figure 1. The six subthemes which are considered to be required for self-regulation, displayed divided over three main themes.
Actually the process of rehabilitation was to rediscover who you are, what you can do, and how you want to use your energy what gives you energy. And then you can get on with your life again. That gave me hope for the future [Female, oncology, 45 years, outpatient].
Theme 1: to have self-insight
Elements on self-insight could be merged into three different subthemes which were labelled as self-insight in the impairment itself, self-insight in the consequences of the impairment, and insight into their abilities. Overall, participants described the significance of understanding what happened to them first, and what the consequences of their impairment were for their body and mind.
Yes, just practically. How does it work? Pain. You learn… the classical example they use is the burglar alarm that broke down. It is oversensitive and reacts too quickly and so you do not have to look for a burglar. The doctor could operate, but what you actually have to do is adjust the system, your brain. Having this insight is crucial [Female, chronic pain disorder, 32 years, outpatient].
Some participants stressed that the most important outcome of their rehabilitation trajectory was the process of learning about themselves. These insights enabled them to continue with their life after rehabilitation, in accordance with their own preferences.
Subtheme I. To have insight into their physical and cognitive impairments
Participants emphasized the importance of understanding their condition or disability. Also, the ability to recognize signs and symptoms in their own body was described as significant for their learning process during their rehabilitation trajectory. It was mentioned that a distorted view of their own impairments, if present, made it impossible to set realistic goals for the future, short- and long-term.
[…] but nobody ever told me that I would be disabled for the rest of my life [Female, spinal cord injury, 51 years, outpatient].
Participants mentioned they needed help to understand their functioning again, with their “new” body and mind. It was described as “retrieving a realistic view of your ‘new’ self.” Lastly, they raised the importance of creating insight into their own thoughts.
Subtheme II. To have insight into the consequences of the impairments and limitations
Having insight into ones’ own restrictions was mentioned in line with understanding the physical and cognitive limitations of their impairment.
You have to understand why you feel pain. Why you have to take it easy. Why you have to do things differently. [Female, chronic pain disorder, 30 years, outpatient].
Participants mentioned they lost the sense of their own abilities, physically and mentally. Realising their limitations was mentioned as being crucial for rehabilitation concerning self-regulation.
It was confronting, the realisation that there was quite a difference between the results of the neurological examination and how I experienced my impairments. That is also part of the rehabilitation trajectory [Male, acquired brain injury, 57 years, outpatient].
The importance of learning how to deal with these restrictions was emphasized as well as creating these insights. Participants mentioned that this insight was crucial to organizing their life in their own way. They meant the practical organisation of their lives, such as arranging medical devices or housing. However, their mental state and emotions were also vital: the ability to understand the consequences of their cognitive impairment. Realising what their impairment means for functioning in daily life was emphasised as being important for the process of regaining self-regulation. They also emphasized that it was important for them to learn their limitations regarding energy level, in order to create a realistic balance between their work and private life. For example, how much work can you cope with and still have enough energy for social activities?
I think setting my boundaries, in terms of having to realise that I couldn’t do what I used to be able to do. I did not have to learn how to walk again, but I certainly had to learn that I could no longer work nine or ten hours a day. I had to take breaks. That was where my limitations were [Female, MD, 39 years, outpatient].
Subtheme III. To have insight into their abilities
Participants emphasised the importance of not only focussing on their impairment, but also on what was still possible.
I can set my own goals, but are they realistic? [Female, neurology, 23 years, inpatient].
Knowledge about abilities was mentioned as being important to optimize participation in different themes of daily life. Participants stressed that their body and mind had changed, with the consequence that their thoughts were not always realistic. Toorganise their life in a proper way, they needed a realistic insight into their actual abilities.
What I also found really good, what I searched for in the beginning, I have this ‘new’ kind of destroyed body. I didn’t dare do much. So I had to find out what I still could do? [Female, oncology, 45 years, outpatient].
Theme 2: to know how to cope with the consequences of the condition
Participants mentioned that after the three steps of the creation of self-insight, coping became important. The coping process consisted, according to the participants, of two subthemes: to be able to communicate limitations, and to trust fully in yourself again, physically and mentally. Overall, participants highlighted the importance of the process of learning how to cope with, and communicate about, their own boundaries based on their new insights.
Subtheme IV. To be able to communicate limitations
Participants emphasised that it was important to learn to communicate their limits to their relatives and surroundings. First of all, not all impairments were visible, which meant they had to tell others about their impairments and limits. In addition, communicating these limits was mentioned as part of the process of learning how to deal with them themselves. Participants explained this as if their surroundings would know and understand their specific limitations; then they would not have to pretend they were able to do something, and push themselves too much.
Communication. I think that is really important to me. If you learn how to talk about everything, without bursting into tears, it will also become easier for those around you to talk to you about it [Female, oncology, 66 years, outpatient].
Subtheme V. To have trust in own body and own functioning
Participants emphasized the importance of being able to trust their own body and their own thoughts again. They described that their body and/or mind had been destroyed. They often lost who they were, and what they were able to do. They had to discover this again, but also to have trust in this “being.”
I think it is all important, especially to re-apply self-regulation in your life, and not just fulfil what a therapist expects of you. But to really have trust in your own body and yourself again, and that you make the right choices [Female, chronic pain disorder, 30 years, outpatient].
Participants described a difference between having insight and having trust. Even when their self-awareness and gained self-insights increased, they still experienced difficulty trusting their own body and mind again. It was important for them to regain this trust by feeling and experiencing what was still possible.
Theme 3: to apply self-regulation in one’s own life
The last step to regain self-regulation was explained by one subtheme, according to participants: to make use of abilities, and to optimize own functioning.
Subtheme VI. To make use of abilities, and optimize own functioning
Participants mentioned that having self-insight and knowing how to deal with these insights were significant for self-regulation, but that in the end, it would be about how to apply this knowledge in daily life. This is what they mentioned as being the last step in their learning process during rehabilitation concerning self-regulation.
I went straight to the sports consultant to find out about sport options in my neighborhood. This was the most important thing for me [Female, amputation, 76 years, inpatient].
Participants mentioned that it was important that they could do what was important for them personally. They stressed that the focus was on decision-making and explained that it was important for them to make realistic decisions so that they would get the most benefit from their abilities. In some cases, participants mentioned they were no longer able to work, but that they adjusted their expectations and focused on other important areas of life such as family. Participants added that even though their personal learning process would continue for the rest of their lives, the first steps taken during rehabilitation to regain self-regulation were crucial in understanding how to apply self-regulation in their daily life.
Well, just being able to cook again… [Male, neurology, 72 years, inpatient].
Discussion
The main findings of this study include a conceptual model of self-regulation based on three main themes and six subthemes. Two of these themes are conditional for regaining self-regulation: 1) having self-insight into one’s condition and abilities (insight in impairments; in consequences of impairments; in abilities); 2) to know how to cope with the consequences of the condition (be able to communicate limitations; have trust in body and functioning). The last theme, 3) concerns how to apply self-regulation in one’s own life (to make use of abilities and optimize functioning). This conceptual model can be used as eligible content for outcome measurement, for developing a theory on the concept of self-regulation, and to improve clinical practice and goal setting [Citation7].
In our study, we used a bottom-up approach to search for elements of self-regulation that former rehabilitation patients considered important. These patients shared the knowledge and competencies they viewed as conditional for regaining self-regulation. In his model, Bandura [Citation12] described three components of self-regulation: self-monitoring, self-judgement, and reaction. Interestingly, these three components largely relate to our third theme on the application of self-regulation in daily life. Other commonly used definitions of self-regulation also focus on how self-regulation is applied in daily life [Citation8,Citation10,Citation23]. We found one related qualitative study which conceptualised exercising self-regulation in a cancer population. It revealed four important factors including value-based goals, unplanned activity, influence from previous goal attempts, and self-reward [Citation24]. Again, the four factors identified in that study are largely in agreement with the third theme of our study, which is focused on applying self-regulation. The results of our study reveal that self-regulation not only includes the application of self-regulation, but also includes aspects that are conditional to executing self-regulation, such as having insight into one’s limitations and abilities and being able to communicate about limitations. These aspects are not new in the rehabilitation literature; examples of instruments measuring one or more of these aspects are available. For example, the Awareness Questionnaire [Citation25] measures the understanding of the health condition, and the University of Washington Self-Efficacy Scale (UW-SES) [Citation26] measures self-efficacy in a health condition. Nevertheless, we believe our model to be useful because a more comprehensive approach to self-regulation is needed in rehabilitation research, in clinical practice, and for the identification of self-regulation measures in rehabilitation.
Clinical relevance
Medical rehabilitation aims to optimize self-regulation as one of the core outcomes for patients [Citation27]. Knowledge and skills are necessary to ensure the active application of self-regulation [Citation15]. If applicable, these requirements or skills should be addressed as part of rehabilitation after the onset of disability. The themes identified in this study can be used to encourage rehabilitation health care workers to pay specific attention to self-regulation. Specifically, the first theme of creating insights can be translated into practice by rehabilitation health care workers sharing their knowledge about the condition and impairments with patients. Also, helping patients experience their possibilities as well as their restrictions in daily life by, for example, practicing daily activities together. The second theme is focused on communication and regaining trust in one’s self. This can be implemented in rehabilitation care by asking patients to practise communicating, for example by letting them explain their condition or impairments or by writing a letter about them. Lastly, to help patients regain trust in themselves, it is important to set realistic goals. Professionals can help set these goals, provide positive feedback and celebrate successes when goals are achieved. In general, the three themes can provide guidance in goal-setting, as these can function as a basis for defining rehabilitation goals.
Future research
A recommendation for future research is to validate the three main themes in different populations, for instance in other countries or cultures. The identified themes help translate self-regulation as a concept into measurable elements in the context of rehabilitation. With regard to outcome measurement, the recommendation is to review the literature systematically for measures for self-regulation in a rehabilitation population, and screen these for content based on the conceptual model developed in the present study. If none of the existing measures fits the three themes from the model, a reliable and valid measure should be developed to gauge self-regulation as an outcome of rehabilitation.
Study limitations
This study included participants with different diagnoses, most of whom were selected via patient organisations. The procedure, which might have induced selection bias, was based on convenience. To overcome this limitation, the additional selection was carried out via a rehabilitation center and social media. An attempt was made to recruit persons from different cultural backgrounds, living in the Netherlands, but the requirement for adequate levels of speaking and understanding Dutch meant that only two of the participants were of non-Dutch origin.
Conclusion
Shared views on the conceptualisation of self-regulation in a rehabilitation setting prevailed in this study. A total of six subthemes were identified, which were merged into three main themes. Two of the main themes of self-regulation are conditional for regaining self-regulation during rehabilitation. The last theme focuses on the application of self-regulation in daily life. These themes may contribute to theory building, improvement of clinical practice and directions for goal-setting, and content for measurement of self-regulation as a rehabilitation outcome.
Appendix_B.docx
Download MS Word (17.8 KB)Appendix_A.docx
Download MS Word (14.7 KB)Acknowledgments
We would like to thank all participants and all patient organisations for contributing to this study and for sharing their experiences.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Revalidatie Nederland. Brancherapport revalidatie. Utrecht (The Netherlands): Revalidatie Nederland; 2018.
- Stucki G, Cieza A, Melvin J. The international classification of functioning, disability and Health (ICF): a unifying model for the conceptual description of the rehabilitation strategy. J Rehabil Med. 2007;39(4):279–285.
- Stucki G, Bickenbach J, Gutenbrunner C, et al. Rehabilitation: the health strategy of the 21st century. J Rehabil Med. 2018;50(4):309–316.
- McClure J, Leah C. Is independence enough? Rehabilitation should include autonomy and social engagement to achieve quality of life. Clin Rehabil. 2021;35(1):3–12.
- Wade DT. Defining rehabilitation: an exploration of why it is attempted, and why it will always fail. Clin Rehabil. 2021;35(12):1650–1656.
- Wade DT. What is rehabilitation? An empirical investigation leading to an evidence-based description. Clin Rehabil. 2020;34(5):571–583.
- Siegert RJ, McPherson KM, Taylor WJ. Toward a cognitive-affective model of goal-setting in rehabilitation: is self-regulation theory a key step? Disabil Rehabil. 2004;26(20):1175–1183.
- Zimmerman BJ. Attaining self-regulation. In: Boekaerts M, Paul MZ, Pintrich R, eds. Handbook of self-regulation. Amsterdam (The Netherlands): Elsevier; 2005, p. 13–40.
- Toering T, Elferink-Gemser MT, Jonker L, et al. Measuring self-regulation in a learning context: reliability and validity of the Self- Regulation of Learning Self-Report Scale (SRL-SRS). Int J Sport Exerc Psychol. 2012;10(1):24–38.
- Baumeister RF, Vonasch AJ. Uses of self-regulation to facilitate and restrain addictive behavior. Addict Behav. 2015;44:3–8.
- Martini R, Cramm H, Egan M, et al. Scoping review of self-regulation: what are occupational therapists talking about? Am J Occup Ther. 2016;70:1–15.
- Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Process. 1991;50(2):248–287.
- Ezekiel L, Collett J, Mayo NE, et al. Factors associated with participation in life situations for adults with stroke: a systematic review. Arch Phys Med Rehabil. 2019;100(5):945–955.
- Tougas ME, Hayden JA, McGrath PJ, et al. A systematic review exploring the social cognitive theory of self-regulation as a framework for chronic health condition interventions. PLoS One. 2015;10(8):e0134977.
- Maes S, Karoly P. Self-regulation assessment and intervention in physical health and illness: a review. Appl Psychol. 2005;54(2):267–299.
- Kuo CC, Lin CC, Lin SY, et al. Effects of self-regulation protocol on physiological and psychological measures in patients with chronic obstructive pulmonary disease. J Clin Nurs. 2013;22(19–20):2800–2811.
- Toglia J, Johnston MV, Goverover Y, et al. A multicontext approach to promoting transfer of strategy use and self regulation after brain injury: an exploratory study. Brain Inj. 2010;24(4):664–677.
- Krabbe PFM. Thurstone scaling as a measurement method to quantify subjective health outcomes. Med Care. 2008;46(4):357–365.
- Wong L. Focus group discussion: a tool for health and medical research. Singapore Med J. 2008;49(3):256–260.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Heal Care. 2007;19(6):349–357.
- Veld D. Oncologische revalidatie geen luxe. Medische Oncologie. 2018;7:44–47.
- Lincoln YS, Guba EG. Establishing dependability and confirmability in naturalistic inquiry through an audit. Am Educ Res Assoc Annu Meet. 1982;1-7.
- Clark NM, Zimmerman BJ. A social cognitive view of Self-Regulated learning about health*. Health Educ Behav. 2014;41(5):485–491.
- Basen-Engquist K. Survivors: a qualitative study. Psychooncology. 2019;27:563–568.
- Sherer M, Bergloff P, Boake C, et al. The awareness questionnaire: factor structure and internal consistency. Brain Inj. 1998;12(1):63–68.
- Amtmann D, Bamer AM, Cook KF, et al. University of Washington Self-Efficacy Scale: a new self-efficacy scale for people with disabilities. Arch Phys Med Rehabil. 2012;93(10):1757–1765.
- Nedelandse vereniging van revalidatieartsen. Position paper medical rehabilitation. Utrecht (The Netherlands): Nedelandse vereniging van revalidatieartsen; 2015.