
Abstract
Purpose
The aim of this review was to examine the efficacy of dance interventions for individuals with cerebral palsy (CP), measured at any level of the International Classification of Functioning, Disability and Health (ICF).
Methods
A systematic review and meta-analysis was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). A comprehensive search of peer-reviewed articles was performed using six electronic databases.
Results
Fourteen studies were included in this review, nine of which were also included in the meta-analysis. The meta-analyses yielded a large overall effect for cognitive, motor, and social-emotional function outcomes, with a high degree of heterogeneity between outcome effects, attributable to differences in study design.
Conclusion
Although recent studies provide support for the acceptance and efficacy of dance interventions for people with CP, the systematic review revealed significant limitations in study design (only 2 randomised control trials). High-quality research that measures outcomes across all dimensions of the ICF, and particularly at the level of participation, are needed to improve the level of empirical support for dance-based interventions.
Implications for Rehabilitation
Movement- and step-based dance practice for cerebral palsy have a positive impact on walking/gait, balance/postural control, and range of motion.
Dance programs should move beyond a traditional focus on body structure and function, placing participation at the forefront of the program.
Rehabilitation professionals should consider forming partnerships with stakeholders, addressing their goals, experiences, and challenges, with dance as a feasible and important option for participation-based practice.
Introduction
Cerebral palsy (CP) is one of the most common physical disabilities in childhood, with an overall birth prevalence of approximately 2 per 1,000 live births globally [Citation1], and a prevalence of 1 in 700 in Australia [Citation2]. The postural and motor dysfunction associated with CP are commonly accompanied by cognitive, sensory, and behavioural impairments [Citation3]. CP is caused by a non-progressive disturbance that occurs in the developing brain, during the pre/peri or post-neonatal period [Citation4,Citation5]. Although the brain lesion is non-progressive, over time, secondary implications of motor impairments together with cognitive and behavioural problems can lead to children with CP becoming increasingly sedentary with reduced engagement and participation in physical, social, recreational, and cultural activities [Citation6,Citation7]. Indeed, these children tend to have lower levels of participation in a narrower range of activities than typically developing children [Citation8], evident across a variety of settings, including at home, within the community, and at school [Citation7,Citation9].
Through the creation of safe and inclusive spaces, arts-based therapies like performing arts (drama, music, and dance), can play an important role in the lives and well-being of people with CP [Citation10]. Dance is a physical and art-based activity that has benefits across social, cultural, emotional, and physical domains [Citation11]. For people with a health condition such as CP, it also provides a unique opportunity for rehabilitation [Citation12]. Dance and movement to music require the performer to prepare and execute a sequence of functional movements, a form of perceptual-motor coordination that can excite motor neurons and train neuromuscular activation patterns for rehabilitative benefits [Citation13,Citation14]. Dance fosters neuroplasticity and provides insights into the neural systems responsible for integrating sensory and motor experiences [Citation13].
The American Dance Therapy Association recommends that dance should be used as a movement therapy for children and adults [Citation15]. Dance has been shown to enhance motor, cognitive and psychosocial functioning in a range of neurological conditions including Parkinson’s disease, intellectual disability, autism spectrum disorder, Down syndrome, and cerebral palsy [Citation11,Citation16,Citation17]. By incorporating physical, cognitive and social domains into a single activity, dance can positively influence neuromusculoskeletal, cardiorespiratory, and sensorimotor functions in people with CP, as well as memory and aesthetic expression [Citation18]. In addition, participation in community dance programs and public dance performances has been associated with the positive development of self-confidence, self-image, self-esteem, and self-worth, along with increased participation in physical and social activities among people with CP [Citation19,Citation20]. These therapeutic benefits of dance span different aspects of health and education by engaging the participant in the process of creating and learning the performance [Citation12,Citation21].
The International Classification of Functioning, Disability and Health (ICF) [Citation22] highlights the reciprocal relationships between the health condition (defined by its three core components of body structure and function, activity and participation), personal factors and environmental factors [Citation23]. Therefore, the framework is a multi-dimensional model that illustrates the bi-directional relationships among these different facets and how their interaction defines an individual’s level of functioning [Citation24,Citation25]. Through the lens of the ICF, many elements and attributes of the dance intervention have the potential to effect changes across all levels of the ICF [Citation23,Citation26]. For example, during the dance performance, people with CP are encouraged to take controlled risks by creating new movements, a process that supports: the development of motor control and fitness (body function); motor skill development and self-directed choreography (activity & participation); and participation in the dance performance itself (activity & participation) [Citation16,Citation27].
Recent systematic reviews of the dance intervention literature suggest dance has positive effects on changes in body functions, such as mobility and transfer [Citation3,Citation18]. However, there is an increasing awareness of the importance of participation in health and wellbeing and an increasing number of empirical studies demonstrating participation-focused interventions improved body structure and function [Citation28,Citation29]. To date, dance interventions have primarily focused on body structure and function [Citation3,Citation11,Citation18]. Although the ICF includes contextual factors that influence Body Structure and Function (BS&F), it fails to fully capture the construct of participation (which includes both attendance and involvement aspects), and associated person-related factors like self-concept, self-efficacy and self-determination [Citation3,Citation23]. To clearly understand the efficacy of dance interventions across all domains of the ICF particularly participation, the Family of Participation-Related Constructs (fPRC) framework will help to provide a broader understanding of participation and its related concepts, including, but not limited to activity competence, self-concept, self-efficacy, and social participation [Citation3,Citation28].
The fPRC is an ecological framework that extends the notion of participation and the intrinsic and extrinsic factors that influence the life outcomes of people with a disability [Citation25,Citation30]. In the fPRC, the two core components of participation are attendance, which can be defined as being present at the activity and measured as frequency, and involvement, which includes intrinsic elements such as the social connection, engagement and motivation of the individual, measured subjectively [Citation25,Citation31]. Indeed, to understand and measure the level of involvement, it is necessary to take into consideration the contextual element of the activity and the internal motivations of the individual [Citation32]. In the context of an intervention for someone with a disability like CP, participation in a community-based activity can be the means by which health and well-being outcomes are achieved (aka participation as a means). Alternately, interventions can also be designed and implemented in a more controlled clinical or educational setting but have as their objective an improvement in participation (aka participation as an end).
In an art context, participation as a means can be a community-based program that results in long-term benefits for self-efficacy and self-competence [Citation23]. Participation in artistic activities, like dance, can provide a motivating and inclusive environment, with ongoing opportunities for creative expression [Citation3]. For Schlebusch et al. [Citation31], participation can be investigated as an independent variable (as a process), or as an outcome (dependent variable). Therefore, to further understand the effects of dance interventions on participation, the authors grouped the activity outcomes (basic motor skill) in the motor function subgroup and used the fPRC framework to provide a more specific understanding of participation and its intrinsic and extrinsic factors.
Furthermore, there is a lack of evidence supporting the potential suitability of dance as a therapeutic resource in relation to participation outcomes [Citation33]. Clinical trials and systematic reviews are needed to increase the understanding of the effects of dance intervention across the domains of the ICF and allow replication of the intervention in the heterogeneous clinical presentations of CP and diverse levels of GMFCS, MACS and CFCS [Citation34,Citation35]. The primary aim of the systematic review presented here was to examine the effectiveness of dance-related interventions reported in the literature for children and adults with cerebral palsy, measured at any level of the ICF, but with a focus on the core components of participation and person-related factors that influence participation.
Method
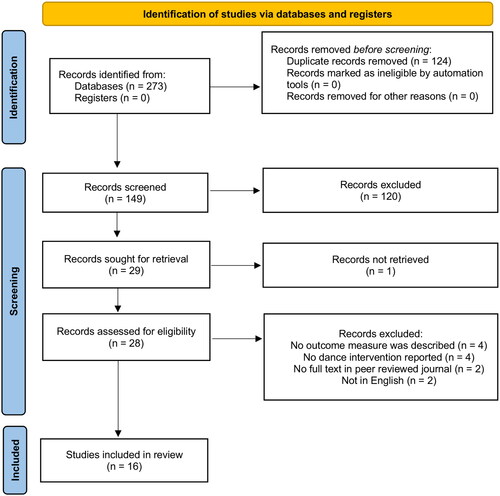
The protocol for this systematic review was developed a priori and registered with the International Prospective Register of Systematic Reviews – PROSPERO (Record ID: CRD42021246272). The review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines () [Citation36].
Figure 1. PRISMA flow diagram.
Search strategy
A systematic search of the literature was conducted on 18 January 2023, using the following databases: CINAHL; Embase; PubMed; PsycInfo; Scopus; and Web of Science. Search terms were (“Cerebral Palsy”) AND (Danc* OR “Art Therapy” OR “Music and Movement”). One member of the research team (ED) performed the initial database search for potentially relevant papers, with search terms cross-checked with other members of the authorship team. After the initial search, titles and abstracts of articles retrieved were exported to the Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia) [Citation37] to facilitate title/abstract and then full-text screening. The titles/abstracts and full texts were independently screened against the predefined inclusion and exclusion criteria by two reviewers: the lead author (ED) and one other member of the research team (PHW, MHC, LM, TBM). Any discrepancies related to the inclusion of studies were resolved through discussion, and if consensus was not reached, a third author provided adjudication. Full-text articles that met the criteria were retrieved and subjected to quality assessment and data extraction.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (1) full-text article, published in English, in a peer-reviewed journal; (2) any year of publication; (3) a dance intervention was evaluated; (4) participants had a formal diagnosis of CP, and were of any age or level of Gross Motor Function Classification System (GMFCS), symptom distribution (unilateral or bilateral) or motor subtype (spastic, dyskinetic or ataxic); (5) reported any outcome measures, including changes in body structure, body function, activities and participation, and psychosocial functioning for the people with CP participating in a dance intervention. Studies of dance interventions were excluded if no outcome measure was reported.
Quality appraisal
The methodological reporting quality of full-text papers was assessed by the primary author (ED) using a 16-item modified version of the Critical Appraisal Skills Programme (CASP) that captured case-control, cohort, and randomised controlled trials [Citation3]. The CASP checklists do not recommend a scoring system, therefore, the risk of bias for each of the 16 individual items was assessed on each quality as: (i) ‘Low’ indicating the item was clearly described; (ii) ‘High’ indicating the item was not clearly reported, and (iii) ‘Unclear’ if insufficient information was provided to determine the quality of the study [Citation3]. To allow for the inclusion of case studies, the Joanna Briggs Institute (JBI) Appraisal Checklist for Case Reports [Citation38] was used to assess the methodological quality of each of the eight items as (i) ‘Yes’ indicating that the item was described, (ii) ‘No’ when the item was not reported, and (iii) ‘Unclear’ if insufficient information was provided [Citation39]. Items that were not applicable to the study being appraised, were identified as “not applicable”.
Outcome measures and subgroups
For the meta-analysis outcome measures were entered into five subgroups: (i) cognitive function, (ii) motor function, (iii) social and emotional function, (iv) engagement, and (v) metabolism.
Cognitive functions subgroup concerns cognitive operations that are necessary to perform tasks of varying complexity [Citation11,Citation40], and include executive functions (working memory, inhibition and executive attention), as well as higher-order planning and organisation skills (rhythmic reproduction), sustained attention, and learning [Citation33,Citation41,Citation42].
The motor function subgroup captures changes in balance (i.e.., dynamic and static balance); postural control (e.g., deviations in centre of force (COF), limits of stability (LOS)); motor control; gait; strength; and range of motion (ROM) [Citation12,Citation20,Citation41–44]. Due to the limited number of studies and small sample sizes the activity outcomes (basic motor skill), such as mobility and transfer and self-care, were grouped in the motor function subgroup [Citation12,Citation33,Citation42]
The social and emotional function subgroup includes (i) body image (awareness of identity moderator); (ii) social/interpersonal factors (e.g., social problems; relationship issues); (ii) psychological factors (like anxiety, somatic complaints, and depression), and (iii) behavioural difficulties (e.g., aggression, internalizing problems, etc.) [Citation6,Citation12,Citation33].
Participation outcomes, as dependent variables, such as sport and physical activity outcomes, community activities, household responsibilities and day-to-day work/school, were listed under the subgroup and moderator “Engagement” [Citation6,Citation33,Citation41].
The metabolism subgroup clustered changes in body weight, aerobic fitness, haematological functions, and metabolic functions [Citation45,Citation46].
Data extraction
A customised data extraction tool using an Excel (MicroSoft Inc.) worksheet was designed for data extraction. Data were extracted by the first author (ED) and included: participant characteristics (age, CP subtype, and GMFCS level); details of the intervention (dance style, intervention protocol, number of training sessions, number of hours in intervention); type of outcome measured; measurement tools; and the study outcomes, when available, means, standard deviations (SD) and sample sizes were extracted, for pre- and post-interventions.
Furthermore, outcomes measured were mapped across the domains of ICF, by the first author (ED). The linking process involved assigning codes of the ICF domains of “Body Structure and Function” and “Activities and Participation”, and any discrepancies related to the coding were resolved through discussion with one other member of the research team (PHW, MHC, LM, TBM), if consensus was not reached, a third author provided adjudication.
Family of participation-related constructs
In addition to mapping outcomes across the domains of the ICF, to further understand participation in dance programs, the two core components of participation (attendance and involvement) were extracted together with the related person-related concepts of activity competence, sense of self, and preferences using the family of participation-related constructs (fPRC) framework [Citation25,Citation30].
Statistical analysis
Study analyses were conducted using R version 4.0.5 [Citation47]. Standard error (SE) values were converted to SD, where necessary [Citation48]. Hedges’ g effect sizes were used to quantify the magnitude of the difference between groups, calculated on the basis of pre-post changes in mean and SD using the ‘esc’ package [Citation48]. The pre-post changes in SD were imputed, with a correlation coefficient 0.5 used when this data was not reported [Citation49]. For studies where mean and SD were not reported, the effect size was estimated using the pre-post change p-value and sample size, calculated by the ‘compute.es’ package [Citation50]. Effect sizes were calculated such that positive values indicated better performance post-intervention.
Multi-level random-effects meta-analysis, which is preferred when multiple effect sizes are drawn from individual studies, was performed using the ‘metafor’ package [Citation51]. This approach allows the inclusion of each individual effect size in the calculation of aggregate measures while accounting for the non-independence of effect sizes [Citation52,Citation53]. The multi-level approach also provides estimates of heterogeneity within comparison effect sizes (i.e.., level 2), and between studies (i.e.., level 3) [Citation53]. Heterogeneity was evaluated with the I2 statistic, with greater than 75% representing considerable heterogeneity [Citation52,Citation54,Citation55]. The ‘dmetar’ package was used to calculate I2 [Citation56]. The Hartung-Knapp-Sidik-Jonkman method was applied to estimate the variance of pooled effects as it outperforms other methods when there are few studies or substantial heterogeneity [Citation57,Citation58].
To compare the effectiveness of the dance interventions on all outcomes, each outcome measure was entered as a moderator. A separate subgroup meta-analyses were run for cognitive/mental function, motor function, and social and emotional function. The magnitude of each combined estimate was interpreted according to Cohen [Citation59]. Furthermore, 95% confidence intervals (CI) were derived for all combined effect sizes to determine significance, which was indicated when the CI did not cross zero [Citation5,Citation52].
Moderator analysis
To explore high heterogeneity and to provide more detailed recommendations for dance programs, moderator analyses were run, including such factors as study design, study sample size, participant ability to ambulate, intervention dose, intervention intensity, and dance type.
The intervention dose was calculated as the total duration of dance interventions in minutes. Intervention intensity was calculated as the minutes of dance interventions per week. Dance types were based on two broader dance classifications: (1) Movement-based dance styles focused on spontaneous and self-willed movements impacting the exploration and transformation of the sense of self, and (2) Step-based dance including dance styles with specific pre-planned steps and techniques [Citation60–62].
Results
Search results
A total of 273 potentially relevant articles were identified from the search strategy. After duplicates (n = 124) were removed, the titles and abstracts of 149 articles were screened for eligibility. Of these articles, 29 met inclusion criteria based on title and abstract, one record could not be retrieved and 28 were retrieved for full-text review. Twelve articles were excluded for the following reasons: no outcome measure was described (n = 4); written in a language other than English (n = 2); the full text was not available in a peer-reviewed journal (n = 2); no dance intervention was included (n = 4). The search results and screening process are:
Characteristics of included studies
The included 16 studies were published between 1989 and 2022. Six studies were conducted in the USA [Citation15,Citation26,Citation35,Citation41,Citation43,Citation63], three in Brazil [Citation6,Citation33,Citation44], two in Japan [Citation45,Citation46] and Korea [Citation12,Citation20], and one each from Spain [Citation64], Ukraine [Citation65], and Canada [Citation42]. Study design varied and included 4 case studies [Citation15,Citation35,Citation63,Citation64], 7 pre- and post-intervention designs [Citation12,Citation20,Citation41,Citation42,Citation45,Citation46,Citation65], 3 pilot studies (of which two were clinical trials; one exploratory) [Citation6,Citation26,Citation43], and 2 RCTs [Citation33,Citation44].
Level and quality of evidence
The methodological quality scores of the articles reviewed are displayed in and . Of the 16 included studies, 12 were assessed using the modified CASP scale () and four used the JBI Appraisal Checklist for Case Reports (). Seven studies did not adequately control for confounding factors: three studies ensured random allocation of participants [Citation33, Citation44], however, one did not provide sufficient information to determine how random allocation occurred [Citation43]. Lakes, et al. [Citation41] used regression models, due to the lack of an available control group, and Cherriere, et al. [Citation42] considered the heterogeneity of the sample and the absence of a control group by using the tip pinch strength task as a control measure and a double baseline.
Figure 2. Methodological quality assessment of case-control, pilots, and randomised controlled trials on a dance intervention for people with CP using the Modified CASP scale.
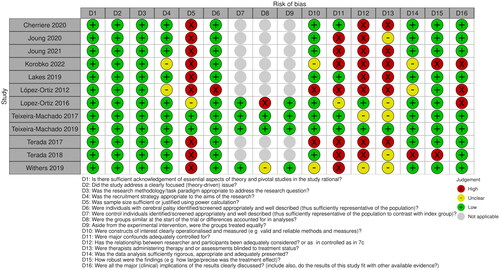
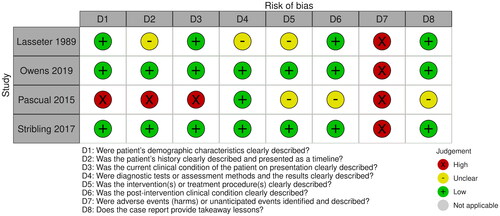
Figure 3. Methodological quality assessment of case studies on a dance intervention for people with CP using the JBI critical appraisal checklist for case reports.
The majority of the studies were shown to have weak methodological reporting quality. While many studies reported a small sample size as a weakness, only two studies clearly reported a power calculation [Citation33,Citation44]. The studies with the lowest risk of bias were the two conducted by Teixeira-Machado [Citation33,Citation44], which were both RCTs. However, only one of these studies reported assessor blinding [Citation44]. The studies by Lopez-Ortiz, et al. [Citation26] and Korobko, et al. [Citation65] presented the highest risk of bias, although those were exploratory and observational study designs, for Lopez-Ortiz, et al. [Citation26] the qualitative nature of the interview and the lack of follow up were weaknesses for the study. Group data analysis was presented in 10 studies, and was adequate for meta-analysis. Only one of the pilot studies did not report pre-post outcomes addressing the effect of the dance intervention [Citation26].
Four studies were case studies, assessed using the JBI Appraisal Checklist for Case Reports. All four studies did not identify possible adverse or unanticipated events for the dance intervention. Stribling and Christy [Citation15] and Owens and Silkwood–Sherer [Citation35] presented the lowest risk of bias. In contrast, the study by Morán Pascual, et al. [Citation64], presented the highest risk of bias among the case studies.
Participant characteristics
The demographics and levels of severity of the participants in each study are shown in . In total, 147 participants were included, ranging from 1 to 27 participants per study. Three studies included adults with CP, three included adolescents and adults, and nine included children and youths with CP. The age of the participants varied, with the mean age for the dance groups ranging from 12 years 9 months to 54 years old. Only one study did not report the age range of the participants [Citation26]. The level of motor function was assessed in participants using the GMFCS (ranging from I to V) in 81.25% of the studies, however, three did not report the GMFCS level for their participants [Citation41,Citation63,Citation64]. The participants’ motor subtypes also varied across studies and included spastic to ataxic and dyskinetic CP. Reported distributions included diplegia, hemiplegia to quadriplegia. The paper by Lopez-Ortiz, et al. [Citation26] reported 16 children with GMFCS levels ranging from I to V but did not detail the level of motor function of each participant. Eight studies only had participants that were able to walk (GMFCS Level I and II), and six studies included people with CP who were able to ambulate and people who needed a mobility device/wheelchair. Two studies only included participants transported in wheelchair in all settings (GMFCS Level V) [Citation45,Citation46].
Table 1. Summary of studies characteristics and proposed ICF codes.
Dance intervention and outcome measures
The range of dance interventions and protocol descriptions are also reported in . Although most studies involved interdisciplinary research teams, only six reported the dance intervention being carried out by people experienced in teaching dance intervention [Citation6,Citation12,Citation15,Citation20,Citation41,Citation42]. Nine studies conducted the dance intervention in community settings, four in dance studios [Citation15,Citation33,Citation41,Citation64], and five in community centres, school gymnasiums or halls [Citation6,Citation43,Citation45,Citation46]. The intervention frequency varied from at least 6 to 15 min twice weekly, to one 2-h session twice weekly [Citation12,Citation45,Citation46]. The minimal total dose of intervention reported was 720 min, and the maximal dose reported was 2880 min [Citation12,Citation43]. Five studies did not report the total dose of their intervention [Citation26,Citation45,Citation46,Citation64,Citation65]. Nine studies reported holding a dance performance or presentation following the intervention period [Citation6,Citation12,Citation20,Citation26, Citation42–44,Citation63,Citation65].
Creative dance (CD), ballet training, informal dance, and hip-hop were among the dance styles used for the interventions. Joung et al. [Citation12] described the CD intervention framework used for people with CP who were able to walk, with a detailed description of each stage (Play, Move and Dance), to support the replication of the intervention. Teixeira-Machado and DeSantana [Citation44] developed a dance protocol called Técnica Aplicada Lavinia Teixeira [TALT], based on Feldenkrais, Horton, Graham, and Laban/Bartenieff concepts. Their protocol followed four sets with eight repetitions for each procedure: (1) global range of motion; (2) motor coordination; (3) body image and environment; (4) skill and agility, however, the authors did not describe how the intervention would be implemented for participants who were ambulant versus those in a wheelchair. Both of the approaches above have similar characteristics, and incorporate self-awareness, self-control, body-awareness, and the active application of the will to the processes of growth, following the principles of movement-based practice [Citation12,Citation20,Citation33,Citation44,Citation60]. Lopez-Ortiz, et al. [Citation43] developed a dance protocol based on classical ballet, the Targeted Dance Class (TDC). Six studies described their dance intervention as including the following components: a warm-up, dance practice/choreography composition/rehearsal, and a cool-down [Citation6,Citation35,Citation41,Citation42,Citation63,Citation65]. Three studies did not report the dance protocol used [Citation45,Citation46,Citation64].
All reported outcomes were linked to ICF codes (). The most investigated outcomes were changes in mobility [Citation6,Citation12,Citation20,Citation33,Citation35,Citation41,Citation42,Citation65],followed by balance [Citation15,Citation20,Citation35,Citation42,Citation43], range of motion (ROM) [Citation12,Citation44,Citation64], and changes in metabolism (cardiovascular, haematological and metabolic) [Citation35,Citation41,Citation45,Citation46]. For Withers, et al. [Citation6] and Teixeira-Machado, et al. [Citation33] participants presented improved mobility. Joung, et al. [Citation12] reported statistically significant changes in spatiotemporal gait (p < 0.05), while Lakes, et al. [Citation41] reported a change in gait pattern between pre, post and follow-up assessments (p < 0.05). Statistically significant improvements in balance (p < 0.05) were reported in two studies using the Pediatric Balance Scale (PBS) [Citation42,Citation43] and one using the Berg Balance Scale (BBS) [Citation20]. Joung, et al. [Citation12] and Teixeira-Machado and DeSantana [Citation44] also observed positive changes in hip and ankle range of motion (ROM), p < 0.05. Only three studies addressed cognitive/mental function [Citation6,Citation33,Citation42], and emotional expression outcomes [Citation6,Citation12,Citation63]. Of those, Cherriere, et al. [Citation42] reported no statistically significant change for sustained and divided attention, and the case study by Lasseter, et al. [Citation63] presented no formal analyses for changes in self-concept and self-esteem.
Participation outcomes
Outcomes at the Body Functions and Structure level were measured in all 16 papers, while only five studies assessed participation in the community, social and civic life (e.g., engagement in sporting and physical activities, dance and art shows, and general community activities) [Citation6,Citation26,Citation33,Citation41,Citation65]. Teixeira-Machado, et al. [Citation33] reported improvement in the dance group joining community activities (p = 0.007), while Withers, et al. [Citation6] reported significant differences in the sporting domain, between the dance group and the control group post-intervention (p < 0.05). Mapping participation constructs to the fPRC framework enabled further consideration of the factors that influence participation [Citation9,Citation66]. reports participation components (attendance and involvement) and the intrinsic person-related concepts of participation (activity competence, sense of self, and preferences) assessed across all studies [Citation66].
Table 2. Studies mapped to the family of participation-related constructs (fPRC).
Table 3. Moderator analysis effect of dance type, dose, intensity, sample size and study design on outcomes effects size.
Seven studies reported attendance at dance classes, three reported attendance rates, which varied from 85% to 98.2% [Citation6,Citation12,Citation20,Citation35,Citation41,Citation42,Citation45], and one study reported participants’ attendance at dance performances [Citation65]. Eight studies reported participants’ involvement, but only three measured this domain [Citation6,Citation20,Citation26]. Only Withers, et al. [Citation6] assessed involvement while taking into consideration focus, confidence, aptitude, and participation. In this study, there was a strong correlation (r = 0.67, p = 0.05) between increased social competence and participation [Citation6]. The fPRC also defines factors at the individual level that influence participation, conceptualised as intrinsic person-related concepts [Citation25,Citation30]. Activity competence was assessed in all 16 studies, but most studies did not measure or mention a sense of self and preference. Only five studies assessed sense of self [Citation6,Citation12,Citation20,Citation63,Citation65] and two reported associated data [Citation15,Citation35]. Increased self-confidence was assessed in four studies, however, three studies did not report quantitative data [Citation20,Citation63,Citation65], and one study only reported an extremely strong correlation between the self-confidence and withdrawn/depression variables (r = −0.91, p = 0.001) and a very strong correlation between self-confidence and affective problems (r = −0.88, p = 0.001) [Citation6]. Body image was assessed in one study showing statistically significant pre- vs. post-improvement (p = 0.005) [Citation12]. Five studies measured preferences, with enhanced engagement in community and school activities highlighted by participants as they began to experience the same activities as their peers [Citation15,Citation20,Citation26,Citation63,Citation65]. Additionally, five studies reported changes in attitude after participation in dance performances with increased motivation and involvement in community activities and dance programs.
Meta-analysis of intervention studies
Ten studies were included in the multi-level meta-analysis, with a total of 157 effect sizes. presents the forest plots for the meta-analyses that included all outcomes and the five additional subgroups, cognitive/mental function, motor function, social and emotional function, engagement, and metabolism. The multi-level meta-analysis by outcomes yielded a large effect overall (g = 1.18, 95% CI = [0.19, 2.18]), with very high heterogeneity I2 = 90.7%. However, most of the heterogeneity came from the study level (I2 level-3 = 79.03%).
Figure 4. Forest plots for the meta-analyses on all outcomes, with each outcome measure, entered as a moderator and as additional subgroups, including cognitive/mental function, motor function, social and emotional, and other outcome categories.
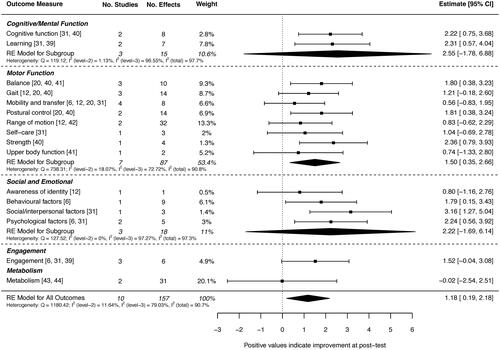
Cognitive/mental function outcomes showed a very large but non-significant effect size, overall, but with wide confidence intervals (g = 2.55, 95% CI = [−1.78, 6.88]), and considerable heterogeneity at the study level I2 (level-3) = 96.55%. The "Learning” outcome returned a large effect size, with a wide confidence interval (g = 2.31, 95% CI = [0.57, 4.04]), contributing to 7.8% of the overall estimated effect size of all outcomes. Motor function outcomes weighted most heavily (53.4%) to the overall effect size. Analysis showed a large effect (g = 1.50, 95% CI = [0.35, 2.66]), with strength, postural control, and balance all yielding significant effects of high magnitude (effect sizes >1.5). Social and emotional function outcomes revealed a large but non-significant effect size, with a wide confidence interval (g = 2.22, 95% CI = [−1.69, 6.14]) and considerable heterogeneity between studies (level 3) I2 = 97.27%. Social/interpersonal factors (e.g., social problems and relationships); and Psychosocial factors (like anxiety, somatic complaints, and depression) outcomes yielded significant effect sizes (g = 3.16, 95% CI = [1.27, 5.04]; and g = 2.24, 95% CI = [0.56, 3.92]). Behavioural factors also contributed to a large effect size (g = 1.79 CI = [0.15, 3.43]) and weighted more than half of the social and emotional function outcomes subgroup (6.1%). Despite the large effect, the engagement moderator was non-significant (g = 1.52, 95% CI = [–0.04, 3.08]).
Moderator analyses revealed that the two RCT studies [Citation33,Citation44] had significantly larger effects than non-RCT studies (p < 0.001), with the RCT studies having the highest estimate among all moderators (g = 4.08, 95% CI = [3.61, 4.54] (). Outcomes were significantly improved for those with the ability to ambulate compared with those who could not (p = 0.024), and for movement-based dance types compared with step-based (p = 0.040). On the other hand, the intensity (minutes/week) and dose (total minutes) of the dance intervention did not significantly moderate outcomes [Citation12,Citation20,Citation33,Citation44].
Discussion
This combined systematic review and meta-analysis evaluated 16 studies that investigated the effects of dance intervention for people with CP, measured across levels of the ICF. Ten of these studies had not been previously reviewed systematically [Citation3,Citation18]. Our review showed most studies were of low methodological reporting quality and had small sample sizes. Only two studies were RCTs [Citation33,Citation44] and dance protocols were often poorly described, with only two clearly detailing the content and pedagogy of the dance intervention [Citation12,Citation20]. Outcomes related to body structure and function were most reported across studies. Meta-analysis of these outcomes suggested that dance interventions are an effective means of improving motor function outcomes, but there was heterogeneity in the profile of effect sizes within performance categories. Few studies reported the effects of dance interventions across the participation constructs. The pattern of results within each of the major categories of function is discussed below. The discussion will also address the need to move toward participation-focused dance interventions in future studies.
Body structure and functions
Neuromusculoskeletal and movement-related functions
The most frequently reported outcomes were walking/gait, balance/postural control, and range of motion (ROM), with the meta-analysis showing large, significant improvements in postural control and balance (g values > 1.81). Measures of balance were varied, while two studies used the Pediatric Balance Scale (PBS) [Citation42,Citation43]. The results for balance outcomes were consistent with earlier work on the effects of dance in children with disabilities by May and colleagues (2021). The results of their research yielded a significant pooled effect for balance in response to the intervention (g = 1.028, 95% CI = [0.575, 1.481] p < 0.001) [Citation11]. Many aspects of dance interventions incorporate gross motor training such as sequential movements around the room while responding to music and beats of different tempos, challenging their limits of stability and spatial awareness [Citation12,Citation20]. By comparison, recent studies show moderate evidence to support the use of exercise-based (gross-motor) training to improve postural control in ambulant children with CP; this training involves repetition of simple functional exercises involving balance, walking and standing activities [Citation67].
Basic mobility for ambulant participants with CP (walking/gait) was measured in six studies [Citation6,Citation12,Citation33,Citation35,Citation41,Citation42], however, seven different outcome measures were used, highlighting the need for greater consistency in measurement when determining efficacy across several studies with small sample sizes. In their scoping review of dance interventions for CP, Cherriere and colleagues also identified that researchers fail to adopt standardised tools and validated outcome measures [Citation18]. This issue was further highlighted in our review, which limits conclusions about the effects of dance intervention for people with CP [Citation68].
The overall effect of dance on lower-limb range of motion was moderate (but non-significant), g = 0.57 [95% CI −1.13, 2.26], while the specific effect reported in the RCT by Teixeira-Machado and DeSantana [Citation44] was significant. Indeed, consistent with earlier reviews, there are promising findings on the effect of dance intervention on the amplitude of movement [Citation69]. However, additional data is needed to address the determinants of change, related to such factors as training intensity and schedule (Teixeira-Machado and DeSantana [Citation44]).
Mental functions
Cognitive/Mental Function was explored in only three studies of dance interventions, despite the fact that cognitive function is often impaired in children with CP, with this review yielding a large effect size g = 2.55 (95% CI = [−1.78, 6.88]) [Citation11]. The earlier meta-analysis of Koch, et al. [Citation40] also showed that dance intervention can benefit cognitive skills. Similarly, however, the limited number of studies and the wide confidence intervals do not allow us to dissect the specific effects on different aspects of cognition including working memory, executive attention, sustained attention, and processing speed [Citation11,Citation18].
Similarly, few studies explored the benefits of dance on the psychological well-being of people with CP. Mental health problems such as depression and anxiety were only measured by Withers, et al. [Citation6]. And, the RCT by Teixeira-Machado, et al. [Citation33] showed improved psychosocial, interpersonal, and behavioural factors after the dance intervention. The systematic review and meta-analysis by May, et al. [Citation11] also highlighted this gap in research and encouraged studies that evaluate the use of dance to develop the social skills of children with disability. Our review did show that the two studies measuring psychosocial functions had statistically significant and positive gains [Citation6,Citation33], consistent with the earlier meta-analysis of Koch showing benefits for quality of life and interpersonal skills [Citation40].
Participation and the family of participation-related constructs
Participation outcomes were the key point of interest for this review; however, only three studies measured participation as an outcome and very few measured the intrinsic and extrinsic components of participation. Artistic and creative experiences, such as dance, allow a playful approach that fosters participation, however, studies of dance maintain a focus on physical outcomes at the body structure and function level [Citation23,Citation70,Citation71]. A necessary shift from impairment-focused to participation-focussed interventions is needed to improve outcomes across all levels of the ICF for people with CP [Citation29,Citation72], using participation as an entry point to physical, recreational, and social activities, may help to develop body structure and function, and further participation [Citation9,Citation23].
According to the family of participation related constructs (fPRC), the two core components of participation are attendance (measured commonly as frequency) and involvement (measured subjectively and including elements like social connection, engagement, and motivation) [Citation25,Citation31]. While eight studies measured participants’ attendance at dance classes and performances, only three assessed involvement [Citation6,Citation20,Citation26]. Schlebusch et al. [Citation31] identified that most studies investigated participation as “being there” (adherence/attendance), which aligns with our findings.
Interestingly, attendance was frequently construed as being related to personal or inter-personal factors, but supporting data was not provided. Teixeira-Machado and DeSantana [Citation44] reported that adherence was due to participants’ sense of belonging. Similarly, Joung et al. [Citation12] reported a high level of satisfaction due to the high level of attendance (98%), while Cherriere, et al. [Citation42] also reported a high participation rate (85%) and noted that participants and families were highly motivated and enjoyed the intervention. Notwithstanding this, not one of the three studies just mentioned measured involvement. According to the fPRC model, participation is more than the individual’s physical presence at an activity [Citation23]. The participants’ involvement is their subjective experience while engaged in the activity, with aspects that are frequently overlooked in research including motivation, persistence, and social connection [Citation7].
A strong link has been suggested between participation in dance and improved psychosocial functioning [Citation33]. Teixeira–Machado et al. [Citation33] reported a correlation between improved participation outcomes (r = 0.97, p = 0.01) and psychosocial adjustment (r = 0.83, p = 0.005). Similarly, Withers, et al. [Citation6] reported a strong correlation between increased social abilities and participation in dance intervention (r = 0.67, p < 0.05). Dance as a means of positive participation experience has the potential to develop preferences for further participation in physical activities [Citation16,Citation73]. For example, Lopez-Ortiz, et al. [Citation26] reported that children with CP who are involved in classical ballet training expressed the desire to have more dance classes, participate in a school group, and develop a new interest in attending art and dance shows. However, the findings from Lopez–Ortiz, et al. [Citation26], should be interpreted with some caution as no follow-up evaluation was conducted to confirm if there were changes in participation in community-based creative activities over time.
All five studies that provided the opportunity for participants to present a dance performance to an audience, reported a positive change in attitude. Indeed, for Teixeira-Machado and DeSantana [Citation44], the dance performance was an awakening moment for people with CP, providing an opportunity to be a (positive) centre of attention, on stage and receive standing applause (see also Joung, et al. [Citation12]). For Withers, et al. [Citation6] the dance performance motivated children with the lower aptitude to develop better individual performance. In the post-performance interview used by Joung, et al. [Citation20] participants reported a feeling of joy when presenting their achievements to the public and receiving applause from the audience. In a similar vein, a study on dance clasperformancesses and public performance for perception of wellbeing in people with Parkinson’s disease shows that public dance performances may contribute to a magnified experience of wellbeing [Citation74].
Taken together, this review shows that the ICF Body Function and Structure, and Activity domains were commonly measured outcomes, but only few studies measured participation as an outcome, and even fewer measured the participation in dance intervention as a process, even though understanding engagement and involvement is an important part of the biosocial framework of the ICF [Citation32]. As well, it remains unclear whether dance interventions impact the children’s interests and preferences into the future. This review reenforces the growing need for dance interventions that focus on participation outcomes, placing participation at the forefront dance program [Citation33,Citation72]. However, to integrate participation in practice, a dialogue between researchers and the stakeholders is needed to form a genuine partnership [Citation72]. To be participation-focused practice, collaborative tools should be used to address stakeholders’ perspectives and goals [Citation72,Citation75].
Strengths and limitations
This review is the first to include a meta-analysis on the effects of dance intervention for people with CP. One of the main limitations of our study was data extraction across such varied methodologies and the small number of studies—the net effect was a meta-analysis that showed wide confidence intervals on combined estimates of effect size and high heterogeneity. This placed some limits on the conclusions that could be drawn about the effects of dance on different aspects of functioning and performance in people with CP [Citation40]. To better understand the characteristics of studies that moderated outcomes, a range of factors were considered. Effects were significantly larger for the two RCT studies than other study designs. With the small number of studies, other moderator outcomes are likely to be heavily influenced by the results of the two RCT studies, and therefore results should be interpreted with caution. Nevertheless, we provide potential insight to practitioners on a range of moderating factors, and results should be used to guide consistency in future work.
The broad definition of participation in the ICF does not adequately capture the complexity of outcomes and, as such, we adopted the fPRC framework to fully describe the aspects of participation considering the intrinsic and extrinsic factors that influence the life of people with a disability [Citation25,Citation30,Citation31]. Unfortunately, the literature base is still limited, and did not provide a sufficient body of work for a robust analysis of participation outcomes.
Future research
This review highlights the need for greater detail regarding the content and pedagogy of dance interventions to allow replication across the heterogeneous clinical presentation of CP. A detailed description of interventions will provide an understanding of the elements of dance that contribute to increased effectiveness [Citation34]. Our meta-analyses also suggested a high degree of heterogeneity between outcome effects, due to differences in study design and measurement. To advance the literature, a more programmatic approach is needed, with improved study designs and greater consistency in the choice of (validated) outcome measures, supporting quantitative reviews of treatment efficacy [Citation10].
Participation-focused research should use collaborative tools to reach decisions together with consumers [Citation72], however, to date no studies were co-designed with consumers, considering the perspectives of people with CP. To close this gap, an interactive process of knowledge exchange should be implemented between those who carry out the research, those implementing the research in real life and most importantly, those whom the research impacts, that is people with CP and their families [Citation76,Citation77].
Conclusion
The number of studies supporting the use of dance interventions for people with CP has increased in recent years. Although, this systematic review revealed significant limitations in the design of recent studies (with only 2 RCTs), and high heterogeneity in population and outcomes measure; this review suggested that movement-based and step-based dance practice have a positive impact on walking/gait, balance/postural control, and range of motion (ROM). More broadly, the range of the study’s designs, and the nature of the outcome measures presented in this review are appropriate for the early stage of the field [Citation10]. Nevertheless, findings should be interpreted with caution and may be used as a starting point to guide clinical practice and enable implementation fidelity of the dance intervention in the real world.
Future research measuring outcomes across all dimensions of the ICF is needed to improve the level of empirical support for dance-based interventions. Furthermore, interventions should move beyond the traditional model of practice focusing on body structure and function, towards a participation focussed model with goals that are meaningful for the participants and their families [Citation29]. In addition, participation-based research should consider information gathered about the child’s desired participation and priorities, to have a positive effect on addressing their needs [Citation31,Citation32].
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Stavsky M, Mor O, Mastrolia SA, et al. Cerebral palsy-trends in epidemiology and recent development in prenatal mechanisms of disease, treatment, and prevention. Front Pediatr. 2017;5:21.
- Australian Cerebral Palsy Register Bulletin, Birth years 1995–2014. In: register ACP, editor. Sydney (AU): CP Register October 2020.
- Lopez-Ortiz C, Gaebler-Spira DJ, McKeeman SN, et al. Dance and rehabilitation in cerebral palsy: a systematic search and review. Dev Med Child Neurol. 2019;61(4):393–398. Apr
- Galea C, Mcintyre S, Smithers-Sheedy H, et al. Cerebral palsy trends in Australia (1995–2009): a population-based observational study. Dev Med Child Neurol. 2019;61(2):186–193.
- Martins E, Cordovil R, Oliveira R, et al. Efficacy of suit therapy on functioning in children and adolescents with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2016;58(4):348–360.
- Withers JW, Muzzolon SB, Zonta MB. Influence of adapted hip-hop dancing on quality of life and social participation among children/adolescents with cerebral palsy. Arq Neuropsiquiatr. 2019;77(10):712–722.
- Resch C, Van Kruijsbergen M, Ketelaar M, et al. Assessing participation of children with acquired brain injury and cerebral palsy: a systematic review of measurement properties. Dev Med Child Neurol. 2020;62(4):434–444.
- Arakelyan S, Maciver D, Rush R, et al. Family factors associated with participation of children with disabilities: a systematic review. Dev Med Child Neurol. 2019;61(5):514–522.
- Kilgour G, Adair B, Stott NS, et al. Do physical activity interventions influence subsequent attendance and involvement in physical activities for children with cerebral palsy: a systematic review. Disabil Rehabil. 2021;7:1–17.
- Edwards BM, Smart E, King G, et al. Performance and visual arts-based programs for children with disabilities: a scoping review focusing on psychosocial outcomes. Disabil Rehabil. 2020;42(4):574–585.
- May T, Chan ES, Lindor E, et al. Physical, cognitive, psychological and social effects of dance in children with disabilities: systematic review and meta-analysis. Disabil Rehabil. 2021;43(1):13–26.
- Joung HJ, Park J, Ahn J, et al. Effects of creative dance-based exercise on gait performance in adolescents with cerebral palsy. J Exerc Rehabil. 2020;16(4):332–343.
- Teixeira-Machado L, Arida RM, de Jesus Mari J. Dance for neuroplasticity: a descriptive systematic review. Neurosci Biobehav Rev. 2019;96:232–240.
- Pitale JT, Bolte J. Efficacy of dance-based paradigms, wearable sensors, and auditory feedback for gait retraining in children: a feasibility study. J Bodyw Mov Ther. 2020; Apr24(2):57–62.
- Stribling K, Christy J. Creative dance practice improves postural control in a child with cerebral palsy. Pediatr Phys Ther. 2017; 29(4):365–369.
- Prieto LA, Haegele JA, Columna L. Dance programs for school-age individuals with disabilities: a systematic review. Adapt Phys Activ Q. 2020;37(3):349–376.
- Patterson KK, Wong JS, Prout EC, et al. Dance for the rehabilitation of balance and gait in adults with neurological conditions other than parkinson’s disease: a systematic review. Heliyon. 2018;4(3):e00584.
- Cherriere C, Robert M, Fung K, et al. Is there evidence of benefits associated with dancing in children and adults with cerebral palsy? A scoping review. Disabil Rehabil. 2020;42(23):3395–3402.
- Swaine B, Poncet F, Lachance B, et al. The effectiveness of dance therapy as an adjunct to rehabilitation of adults with a physical disability. Front Psychol. 2020;11:1963.
- Joung HJ, Yang HK, Lee Y. Effect of dance on balance, mobility, and activities of daily living in adults with cerebral palsy: a pilot study. Front Neurol. 2021;12:663060.
- Menezes DeJesus B, Teixeira-Machado L. The role of dance in the functioning and socialization of people with cerebral palsy: a pilot clinical trial. Electron Physician. 2020;12(4):7784–7790.
- WHO. International classification of functioning, disability, and health: children & youth version: ICF-CY. Geneva: World Health Organization; 2007.
- Duckworth J, Hullick J, Mochizuki S, et al. editorsInteractive arts and disability: a conceptual model toward understanding participation. 2020. Cham: Springer International Publishing; (Interactivity, game creation, design, learning, and innovation.
- Noten S, Troenosemito LAA, Limsakul C, et al. Development of an ICF core set for adults with cerebral palsy: capturing their perspective on functioning. Dev Med Child Neurol. 2021;63(7):846–852.
- Imms C, Granlund M, Wilson PH, et al. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. 2017;59(1):16–25.
- Lopez-Ortiz C, Gladden K, Deon L, et al. Dance program for physical rehabilitation and participation in children with cerebral palsy. Arts Health. 2012;4(1):39–54.
- McGuire M, Long J, Esbensen AJ, et al. Adapted dance improves motor abilities and participation in children with down syndrome: a pilot study. Pediatr Phys Ther. 2019;31(1):76–82.
- Nyquist A, Jahnsen RB, Moser T, et al. The coolest I know–a qualitative study exploring the participation experiences of children with disabilities in an adapted physical activities program. Disabil Rehabil. 2020;42(17):2501–2509.
- Reedman SE, Jayan L, Boyd RN, et al. Descriptive contents analysis of ParticiPAte CP: a participation-focused intervention to promote physical activity participation in children with cerebral palsy. Disabil Rehabil. 2021;8:1–11.
- Adair B, Ullenhag A, Keen D, et al. The effect of interventions aimed at improving participation outcomes for children with disabilities: a systematic review. Dev Med Child Neurol. 2015;57(12):1093–1104. Dec
- Schlebusch L, Huus K, Samuels A, et al. Participation of young people with disabilities and/or chronic conditions in low- and middle-income countries: a scoping review. Dev Med Child Neurol. 2020;62(11):1259–1265. Nov
- Kaelin VC, Bosak DL, Villegas VC, et al. Participation-focused strategy use among caregivers of children receiving early intervention. Am J Occup Ther. 2021;75(1):7501205090p1–7501205090p11. Jan-Feb
- Teixeira-Machado L, Azevedo-Santos I, Desantana JM. Dance improves functionality and psychosocial adjustment in cerebral palsy: a randomized controlled clinical trial. Am J Phys Med Rehabil. 2017;96(6):424–429.
- Beaudry L, Fortin S, Rochette A. Adapted-dance intervention for subacute rehabilitation post-stroke: ‘what’ and ‘how. Research in Dance Education. 2019;20(3):279–296.
- Owens M, Silkwood-Sherer D. Informal dance intervention improves BMI and functional gait in an adolescent with cerebral palsy: a case report. Pediatr Phys Ther. 2019; Oct31(4):E26–E31.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
- Babineau J. Product review: covidence (systematic review software). J Can Health Libr Assoc. 2014;35(2):68–71. 08/01
- Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. Joanna Briggs Institute Reviewer’s Manual the Joanna Briggs Institute. 2017. Available from: https://synthesismanual.jbi.global
- Hickey L, Kuyucak O, Clausen L, et al. Mapping the focus of research conducted with adults with cerebral palsy: an overview of systematic reviews. Disabil Rehabil. 2022;3:1–24.
- Koch SC, Riege RFF, Tisborn K, et al. Effects of dance movement therapy and dance on health-related psychological outcomes. A meta-analysis update. Front Psychol. 2019;10:1806.
- Lakes KD, Sharp K, Grant-Beuttler M, et al. A six week therapeutic ballet intervention improved gait and inhibitory control in children with cerebral Palsy-A pilot study. Front Public Health. 2019;7:137.
- Cherriere C, Martel M, Sarrasin A, et al. Benefits of a dance intervention on balance in adolescents with cerebral palsy. Phys Occup Ther Pediatr. 2020;40(5):518–533.
- Lopez-Ortiz C, Egan T, Gaebler-Spira DJ. Pilot study of a targeted dance class for physical rehabilitation in children with cerebral palsy. SAGE Open Med. 2016;4:2050312116670926.
- Teixeira-Machado L, DeSantana JM. Effect of dance on lower-limb range of motion in young people with cerebral palsy: a blinded randomized controlled clinical trial. Adolesc Health Med Ther. 2019;10:21–28.
- Terada K, Satonaka A, Terada Y, et al. Training effects of wheelchair dance on aerobic fitness in bedridden individuals with severe athetospastic cerebral palsy rated to GMFCS level V. Eur J Phys Rehabil Med. 2017;53(5):744–750. Oct
- Terada K, Satonaka A, Wada M, et al. Nutritional aspects of a year-long wheelchair dance intervention in bedridden individuals with severe athetospastic cerebral palsy rated to GMFCS level V. Gazz Med Ital - Arch Sci Med. 2018;177(7-8):360–366.
- Team RC. R: a Language and Environment for Statistical Computing. 2021.
- Lüdecke D. Esc : Effect size computation for meta analysis (Version 0.5. 1). 2019.
- Higgins JP, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions. Chichester (UK): John Wiley & Sons; 2019.
- Del Re A. Computees: compute effect sizes. R package version 0.2-2. 2013.
- Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Soft. 2010;36(3):1–48. 08/05
- Subara-Zukic E, Cole MH, McGuckian TB, et al. Behavioral and neuroimaging research on developmental coordination disorder (DCD): a combined systematic review and meta-analysis of recent findings. Front Psychol. 2022. DOI: 10.3389/fpsyg.2022.809455
- Baker JM, Reiss AL. A meta-analysis of math performance in Turner syndrome. Dev Med Child Neurol. 2016;58(2):123–130.
- Downs J, Blackmore AM, Epstein A, et al. The prevalence of mental health disorders and symptoms in children and adolescents with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2018;60(1):30–38.
- van Houdt CA, Oosterlaan J, van Wassenaer-Leemhuis AG, et al. Executive function deficits in children born preterm or at low birthweight: a meta-analysis. Dev Med Child Neurol. 2019;61(9):1015–1024.
- Harrer M, Cuijpers P, Ebert D. Doing meta-analysis in R: a hands-on guide. New York (US): CRC press; 2021.
- IntHout J, Ioannidis JP, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. 2014; 14:25.
- Hartung J, Knapp G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat Med. 2001; 20(12):1771–1782.
- Cohen J. Statistical power analysis for the behavioral sciences. Cambridge (MA): Academic Press; 2013.
- Schmalzl L, Crane-Godreau MA, Payne P. Movement-based embodied contemplative practices: definitions and paradigms. Front Hum Neurosci. 2014;8:205.
- Gibbons E. Teaching dance: the spectrum of styles. Bloomington (IN): Author House; 2007.
- Valverde-Guijarro E, Alguacil-Diego IM, Vela-Desojo L, et al. Effects of contemporary dance and physiotherapy intervention on balance and postural control in Parkinson’s disease. Disabil Rehabil. 2022;44(12):2632–2639.
- Lasseter J, Privette G, Brown CC, et al. Dance as a treatment approach with a multidisabled child: Implications for school counseling. The School Counselor. 1989;36(4):310–315.
- Morán Pascual P, Mortes Roselló E, Domingo Jacinto A, et al. On the use of dance as a rehabilitation approach for children with cerebral palsy: a single case study. Stud Health Technol Inform. 2015;217:923–928.
- Korobko LR, Nahorna OB, Prymachok LL, et al. Dance and motor therapy in the physical rehabilitation program of teenagers with childhood cerebral palsy. Acta Balneol. 2022;64(2):138–144.
- Adair B, Ullenhag A, Rosenbaum P, et al. Measures used to quantify participation in childhood disability and their alignment with the family of participation-related constructs: a systematic review. Dev Med Child Neurol. 2018;60(11):1101–1116.
- Dewar R, Love S, Johnston LM. Exercise interventions improve postural control in children with cerebral palsy: a systematic review. Dev Med Child Neurol. 2015; 57(6):504–520.
- Booth ATC, Buizer AI, Meyns P, et al. The efficacy of functional gait training in children and young adults with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2018;60(9):866–883.
- Chang M, Halaki M, Adams R, et al. An exploration of the perception of dance and its relation to biomechanical motion: a systematic review and narrative synthesis. J Dance Med Sci. 2016;20(3):127–136.
- Machado ED, Mendes MDM, Simoni MF, et al. Projeto dança em cadeira de rodas e mobilidade de crianças e adolescentes com deficiência física: série de casos. Cad Edu Saude e Fis. 2021. DOI: 10.18310/2358-8306.v8n16.a10
- Millard O, Lindor E, Papadopoulos N, et al. AllPlay dance: two pilot dance projects for children with disability, developed and assessed with a dance studies approach. Front Psychol. 2021;12:567055.
- Anaby D, Khetani M, Piskur B, et al. Towards a paradigm shift in pediatric rehabilitation: accelerating the uptake of evidence on participation into routine clinical practice. Disabil Rehabil. 2022; 44(9):1746–1757.
- Cameron KL, Allison K, McGinley JL, et al. Feasibility of a dance participation intervention for extremely preterm children with motor impairment at preschool age (dance PREEMIE). Early Hum Dev. 2021;163:105482.
- Carroll SJ, Dale MJ, Bail K. “Out and proud…. in all your shaking glory” the wellbeing impact of a dance program with public dance performance for people with Parkinson’s disease: a qualitative study. Disab Rehab. 2022. DOI: 10.1080/09638288.2022.2122598
- Nguyen T, Palisano RJ, Graham I. Perspectives and experiences with engaging youth and families in research. Phys Occup Ther Pediatr. 2019;39(3):310–323.
- Jull J, Giles A, Graham ID. Community-based participatory research and integrated knowledge translation: advancing the co-creation of knowledge. Implement Sci. 2017; 12(1):150.
- Nguyen T, Graham ID, Mrklas KJ, et al. How does integrated knowledge translation (IKT) compare to other collaborative research approaches to generating and translating knowledge? Learning from experts in the field. Health Res Policy Syst. 2020;18(1):35.