
Abstract
Purpose: To explore the experiences of involvement of adolescents living with cerebral palsy, and their parents, while participating in physical activity. Understanding involvement in physical activity may be used to guide future participation.
Methods: Eight adolescents (mean age 13 years 11 months, SD 1 year 6 months) with cerebral palsy participated in a New Zealand-based high-level mobility programme (HLMP) focused on running skills, twice per week for 12 weeks. The adolescents and 12 parents were interviewed before, after the 12 weeks and 9-months following the HLMP. Guided by interpretative description, 38 interviews were coded, analysed, and interpreted.
Results: Four themes were: “Turning up is not enough” (“There’s no point being there if you’re not involved”); “In it all the way”, “Changes on a dime”, and “What works for me.” Perceptions of involvement varied between adolescents and parents. Being “very involved” related to high levels of focus, concentration, effort; but not always enjoyment.
Conclusions: Focusing on enjoyment as the key experience of involvement understates the complexity and dynamic nature of involvement. “Being involved” is not always easy and may not mean the absence of discomfort or effort. Optimising the individuals’ involvement continuum during physical activity may be essential to promote lifelong participation.
Adolescents living with cerebral palsy and their parents have differing perspective of involvement and utilise different strategies to encourage being and staying active.
Teaching adolescents living with cerebral palsy about their involvement continuum and optimal level of involvement for each activity, context and environment could promote sustained participation.
To ensure adolescents are “being involved” in physical activity, opportunities for engagement, motivation and persistence are important; enjoyment is a possible, but not essential attribute of involvement.
Encouraging involvement in physical activity can be a source of family conflict from a young age therefore clinicians have a role as an essential supporter, motivator and educator.
IMPLICATIONS FOR REHABILITATION
Introduction
Participation in physical activity is the attendance and personal levels of involvement in meaningful life situations; in any context and environment [Citation1]. Attendance and involvement are the key constructs of participation in the Family of Participation Related Constructs (fPRC) framework [Citation1]. Attendance is defined as “being there” [Citation2] and can be understood as the frequency of attending and/or the range of different activities that the child takes part in. Attendance is commonly used as a participation outcome measure [Citation1] such as calling the roll and counting the activities completed. Involvement is the “experience of participation while attending” [Citation1], which may include elements of motivation, persistence, perhaps social connection (if others are present in the activity), affect, and engagement [Citation1]. Despite the importance of “being involved”, involvement is measured less frequently, is most often reported retrospectively by a third person, and is usually measured in terms of enjoyment [Citation3,Citation4]. However, enjoyment does not account for other potential affective experiences of involvement, such as sadness or frustration, or physical and cognitive experiences such as difficulty, or effort. In addition, proxy reporting of another person’s intrinsic experience is problematic [Citation5]. Only a child can fully know and express their personal level of involvement and their “in the moment” experiences. Therefore, the experience of involvement requires more in-depth consideration if we are to promote it and understand it effectively [Citation3,Citation6].
For optimal health and wellbeing physical activity should be sustained [Citation3]. Imms and colleagues propose that “being involved” may be key to ongoing participation in any activity [Citation1]. When a child is participating in physical activity, their attendance will not always reflect their personal experiences of involvement during the activity. Martin-Ginis et al. [Citation7] suggested that using only attendance to measure participation “ignores the meanings and satisfactions that a person derives from participating” [Citation7]. Whilst increased attendance is important and observable, the value and quality of the experience of participation may be crucial to sustaining participation in physical activity [Citation8]. Past and present experiences of involvement need to be considered when implementing a physical activity programme and may comprise more than enjoyment.
Despite the recognition that “being involved” is important when engaging in physical activity, there are gaps in understanding what involvement is and what it means to children when they are active. Tools to capture “in the moment” involvement have not been developed [Citation9]. The relationship of involvement to other constructs within the fPRC are hypothesised but not fully explored and research measuring involvement during and following a physical activity intervention is limited [Citation3]. For all children, including those with cerebral palsy, the experience of involvement may be essential to beginning, completing and continuing being active in physical activity. A recent systematic review revealed that only four of 13 studies measured involvement in children with cerebral palsy, but that three of those four studies failed to report outcomes at follow up, limiting our knowledge of sustained involvement outcomes [Citation3]. The fourth study in that review, reported improved involvement (measured as increased enjoyment) was sustained following a physical activity intervention but was only measured for the four-week follow up period [Citation10]. Thus, our knowledge is limited and a deeper interpretation is required.
Given that children with cerebral palsy are known to have very low levels of physical activity participation [Citation11,Citation12], a greater understanding of what influences involvement, what it looks like to be involved and what is needed to start and keep children with cerebral palsy involved in physical activity is needed. Asking the child about their experiences is crucial if we are to gain greater knowledge of the construct of involvement in real world, meaningful contexts and over the life course. In addition, asking parents about their experiences of their child’s involvement is also important. Although evidence suggests views of children and parents are likely to differ [Citation13], parents will bring a perspective that is important, and without parents to transport, pay and help them take part, children often cannot attend physical activity: a pre-requisite of involvement. Exploring experiences of involvement may contribute to a deeper understanding of the importance of involvement and may identify strategies to promote involvement in physical activity for long-term health and well-being.
Aims
The purpose of this study was to explore the perspectives of adolescents living with cerebral palsy and their parents about their, or their child’s, experiences of involvement, while participating in physical activity. The aim was to build knowledge about involvement to guide families’ and clinicians’ support of young people with cerebral palsy’s participation.
Research questions
What is the experience of involvement in physical activity of adolescents with cerebral palsy from the perspectives of the adolescent and their parent(s)?
What helps and hinders the experience of involvement from the perspectives of adolescents and their parents?
Methods
Design
This study was embedded within a single subject research design (SSRD) intervention study investigating sustained participation in physical activity following a high-level mobility programme (HLMP) [Citation14]. The HLMP focused on running skills: targeted skills training and individualised, self-selected, physical activity goals. The HLMP was designed to support individuals to choose attendance, involvement and physical goals related to any physical activity that was important to them: goals did not need to be running based e.g., I play tennis with my family every week; I focus at least half of the time when I practise my throwing; I can run 2 km without stopping.
An interpretive description qualitative approach was chosen to address the research questions about involvement in physical activity, to inform practice and support change in practice [Citation15,Citation16]. Participants were aware of the phenomenon being investigated: involvement in physical activity. The process was inductive, with focus on the individuals (adolescent with cerebral palsy and their parent) and their experiences [Citation17]. The information gained was subjective but valued as an individual’s own perspective [Citation18]. The experiences and realities when “being involved” in physical activity helped to form subjective themes, while also demonstrating individual variations [Citation15]. Ethical approval for the conduct of the study was obtained from the Health and Disability Ethics Committee, New Zealand (19/STH/22). The research was registered with the Australian New Zealand Clinical Trials Registry (trial identification number ACTRN 12619000126112; universal trial number U1111-1226-8425) because it formed part of a single subject research design (SSRD) intervention study.
Child and parent characteristics
A convenience sample of children and adolescents were invited to participate in a HLMP intervention being tested in a SSRD with embedded qualitative exploration of their experiences. Participants were recruited using posters and online advertising at hospital, therapy services and community organisations that support children with disabilities in Christchurch, New Zealand. Children aged 7–18 years, with a diagnosis of cerebral palsy of any motor type, classified at GMFCS level I–II (Gross Motor Functional Classification System) [Citation19] were eligible to participate. Children were excluded if they had undergone single-event multi-level orthopaedic surgery within the past year or had a history of a medical event in the past 6 months that would limit or contraindicate their participation in a running programme. Children unable to complete interviews and express their experiences and ideas were excluded. A parent (chosen by the family) for each child was invited to participate in the qualitative component. Each parent and child needed to be able to communicate in English because translators were not funded. Informed, written consent was obtained for each child and parent.
Researchers’ characteristics
The lead researcher, GK, was an experienced trainer, coach, and physiotherapist, providing valuable, relevant insights about the phenomenon. The beliefs and expectations of GK during the interviews conducted and the process of analysis were managed by GK by placing herself in a “learner’s” role, by becoming the naïve listener and not the clinician [Citation20]. The broader research team included an occupational therapist with expertise in participation and qualitative methods (CI), a physiotherapist (BA) and an orthopaedic surgeon (NSS), each with expertise in cerebral palsy and physical activity, a biostatistician (MS), and a young woman with lived experience of cerebral palsy (AH). The diverse knowledge and perspectives of the research team were drawn on through design, analysis and interpretation of the findings.
Data collection
All data were collected as part of the larger SSRD study [Citation14]. The full SSRD data collection included: attendance and involvement measures using personalised physical activity diaries over 56–58 weeks, attendance, involvement and physical goal attainment measured fortnightly for the HLMP intervention period and the nine months of follow up, and four physical activity testing sessions. Specific to involvement, children rated each physical activity for the week as: not at all, somewhat or very involved level of involvement, in their personalised diaries e.g., biking was very involved and walking the dog somewhat. Findings from quantitative measures are reported elsewhere [Citation14].
In addition to the quantitative measures of involvement, three semi-structured interviews with the children and their parent(s) were conducted at SSRD baseline, following the 12-week HLMP intervention, and 9 months post-completion of the HLMP, using an inductive design. The baseline interview framework included gaining knowledge and sharing information about: participation (attendance and involvement), physical activity guidelines for children with cerebral palsy, the study aims and the HLMP. The baseline interview set the scene for involvement by supporting children to set involvement goals and develop their diaries to measure involvement. The involvement questions for the second and third interviews were initially planned and further developed based on the data collected at each prior stage.
Consistent language to ask about involvement was used throughout the study including interviews. The weekly diaries included the instruction: “think about how you felt, how much you were thinking about it and how hard you tried for each activity. Your involvement may change each day and there is no right or wrong answer.” During the first interview, words used by each participant for involvement were explored and then used when talking with that participant. New words were added as understanding and perspectives developed.
The interviews explored experiences and perceptions of the following questions: “what is involvement” in any type or form of physical activity; “what “being involved” and “not involved” “looked” like”; and “what was needed to stay involved now and in the future”. Children and their parents were asked to reflect on their HLMP and past physical activity experiences. All interviews were audio recorded. An audit trail, field notes recorded during and after the HLMP sessions, journaling of reflective thoughts, and peer discussions also informed the data analysis.
The interviews were conducted at a location, date, and time suitable for the families, with no time limits imposed. All interviews were conducted face-to-face in a community setting, except for one goal setting session that took place using video-conferencing technology at the child’s request. For each child, the same parent, preferably the one most involved in the HLMP, was encouraged to attend all three interviews. Each child and their parent could choose whether to attend each other’s interviews.
Data management
Voice recordings and transcriptions were stored securely as per ethical requirements. The interviews were transcribed verbatim using Otter (Otter.ai, Los Altos, CA, USA). The Excel (Microsoft Corporation, Redmond, WA, USA) software was used to tabulate text coding line by line and included the person speaking (de-identified), time code, the narrative, the meaningful statement, preliminary code, and preliminary concepts, patterns and themes (see for a coding example).
Table 1. Example of coding of an excerpt from the second interview for a participant.
Qualitative interpretive description analysis
Meaning statements were extracted at each interview phase to help develop future interview questions. All transcripts were re-read throughout the analysis by GK to immerse herself in each child’s and parent(s)’ story and to allow ideas to be reflected on and revisited. Full inductive analysis and interpretation occurred concurrently at the end of the third interviews using the codes developed over time to inform the analysis rather than pre-existing theory [Citation14]. Codes for all three interviews were then clustered to determine similarities and differences between the experiences of each child and their parent to enable “the whole story” to be brought together and establish preliminary patterns and themes. The five additional authors read and listened to two-three full transcripts, GK completed the coding and thematic analyses and all six researchers reviewed and discussed the developing themes. Interpretation of all sources of information helped confirm final themes. In addition, word clouds were developed, as a form of content analysis, using a repeated key word search of all preliminary codes to highlight the frequency of the experiences for the child and their parents, and any differences between them.
Strategies for enhancing rigour and trustworthiness
The potential biases of the researchers were acknowledged and managed by inclusion of interviews, journaling, an audit trail and frequent dialogue between all members of the team, as well as between GK and other professionals, to ensure the process was well-grounded, and to address rigour and reflexivity [Citation14]. Potential biases included GK knowledge of the children through previous physiotherapy consultation (at least two years prior) and AH involvement with some families through the Cerebral Palsy Society of New Zealand. Member checking occurred by presenting each participant and parent with the overall concepts and themes and seeking their critique and feedback [Citation17]. Two checklists, the Standard of Reporting Qualitative Research (SRQR) [Citation21] and the Consolidated Criteria for Reporting Qualitative Studies (COREQ) [Citation22], a 32-item checklist for interviews and focus groups, were used to support quality, completeness and transparency of reporting of the methods and findings to aid reader interpretation.
Results
Participants
Eight participants with cerebral palsy (mean age 13 years 11 months, SD 1 year 6 months) took part in the SSRD and the interpretive description study. The term adolescents will be used in reporting results, as it is more reflective of the included age range, than the words child or children [Citation23]. The adolescents’ mobility was classified at GMFCS level I-II (n = 5 GMFCS I, n = 3 GMFCS II) [Citation19], upper limb skills at Manual Ability Classification Scale I-III (MACS) [Citation24] and communication skills using the Communication Function Classification System (CFCS) at levels I-II [Citation25]. Six adolescents attended mainstream schooling and two were in supported learning units. The adolescents attended the community-based HLMP a median of 23/24 sessions.
Twelve parents (8 mothers, 4 fathers) participated in the interviews, with four adolescents having both parents attend at least one interview. The adolescent-parent dyad was self-selected based on those who attended the HLMP most frequently and remained consistent throughout. The semi-structured interview length varied between 15 min and 45 min. Additional follow-up information was provided via email, telephone, or text message from the participants. Three adolescents chose to be interviewed independent to their parents. Thirty-eight interviews were conducted with full data collection for seven dyads. One dyad did not complete the 9-month follow-up interview as they had left New Zealand. Adolescents are identified within the results with the letter A, and parents with the letter P; with quotes included from all participants.
Talking about involvement
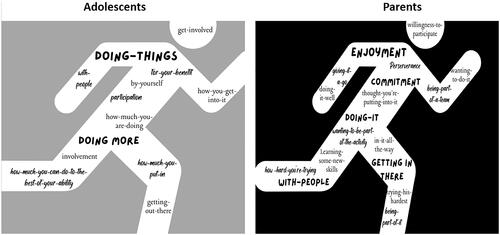
Thematic and content analysis identified the ways in which adolescents and parents talked about involvement. Adolescents and parents used phrases like “doing it”, “getting out there”, and “giving it a go”, either alone or with others (Supplement, Table 1). Words such as “perseverance”, “persistence”, “commitment”, and “enjoyment” and phrases such as “trying hard”, “how much you put into it”, “wanting to do it”, and “in it all the way” were also used to describe involvement. Involvement was identified as highly valued and essential to being active.
While there were similarities between adolescents and parents, there were also differences. shows parents were most likely to talk about enjoyment and commitment, being with others, when describing involvement, while their adolescents used the words “how much” to indicate what was needed to be involved.
Figure 1. A word map of “What is involvement in physical activity” from adolescents with cerebral palsy and their parents’ perspectives.
Themes
Thematic analysis across participants and over time, identified four main themes that described the experience of involvement in physical activity: “Turning up is not enough” (“There”s no point being there if you”re not involved”), “In it all the way” (being involved); “Changes on a dime” (shifting to being not involved), and “What works for me” (motivators and strategies) ().
Figure 2. A word map for “in it all the way” from adolescents with cerebral palsy and their parents perspective when “being involved.”
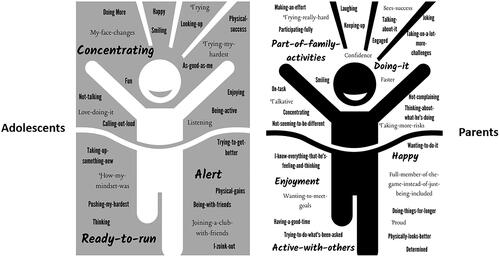
Figure 3. A word map for “Changes on a dime” from adolescents with cerebral palsy and their parents perspective when “not involved.”

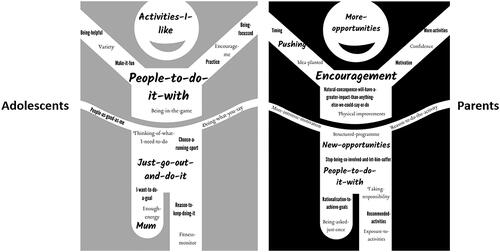
Figure 4. A word map of personal motivators and strategies of “What works for me” from adolescents with cerebral palsy and their parents perspective.
Turning up is not enough
Turning up to physical activity (attending) is not enough. Being involved required effort, focus and determination to make the physical activity experience worth attending “There’s no point being there if you’re not involved” (A). Being fully included fostered involvement “He feels like he’s part of the whole activity. He’s not off to the side and he’s fully involved” (P). Being involved was described as a positive and desired experience that required commitment and should be aimed for when participating in physical activity:
If you’re not 100% committed then you’re not involved, you’re not enjoying it. The flip side obviously if he is involved then he does tend to enjoy it (P).
If you’re gonna [sic] do it, stay committed to it! I’m quite bad at committing to things. It takes me a lot to do something (A).
In it all the way
“In it all the way” highlights that being involved in physical activity required hard work but was rewarding and worth the effort (). Adolescents could clearly articulate what involvement felt like, looked like, and what was needed for them to be involved. Being involved was described as using physical, emotional, and mental processes to ensure they were “in it all the way”:
I would be trying my hardest. Me enjoying myself. Even if I’m struggling. Just doing it carefree (A).
He’s almost got a look of concentration on his face so he’s actually thinking about what he’s doing. He can physically probably hold himself better too (P).
Being “in it all the way” was situation specific. Involvement in cricket for one adolescent could vary from “boring” (if his team was winning or losing by large amounts) to “challenging, competitive, interesting and fun” (A), even within one session. Parents acknowledged the effort required to be involved varied between activities:
I think when he’s part of something, like Parafed or Scouts then it’s not an issue. Sometimes when it’s a bit more intrinsic, it’s got to come from within, that’s probably a little bit harder. Then he needs to concentrate. He’s got the determination to do it really (P).
I probably don’t give him enough credit for probably how tired he is after school. He tries really hard to be normal and to be involved. We just keep pushing him (P).
Some days I’m variable, but it depends if my foot is sore, or some part of my body is sore, then I won’t be as involved as I would be if my body was feeling fine. I just push through it, push through and get it done. My mind tells me to keep on going but my body’s like "too sore" (A)
Changes on a dime
A personal “involvement continuum” appeared to exist for each adolescent, with involvement levels varying from helpful to hindering, for each activity and within a session. The theme “changes on a dime” highlights the dynamic, “in the moment”, unpredictability of involvement from being highly involved and “in it all the way” to “being not involved.”
At the low end of the personal involvement continuum (hindering physical activity participation), adolescents talked about not paying attention and not wanting to be there, “I want to do something else” (A) when not involved. When “not involved” they felt down, bored and dispirited (). When not involved, one adolescent described:
I’m clumsing [sic] about, like swinging side to side not actually doing it. I’d be like phewwwww [sic] if I’m really tired, I just can’t help myself but not concentrate (A).
I liked doing activities by myself because some people get in the way and stuff. I want to concentrate and if people are in my way I just like disorientate [sic] and don’t know what’s going on. So, focus by myself and actually do it (A).
I feel a bit, concerned …, I’m not sure that sad is the right word for it either. It feels painful that you know that he’s not involved, for his sake. I don’t like it either (P).
It makes me exhausted and that kind of annoys me sometimes. Usually, I’m annoyed at the start [be]’cause I know that I get really tired but then at the end it’s not as tiring as I thought (A).
What works for me
The theme “what works for me” emphasised that the personal motivators and strategies for involvement in physical activity varied for each adolescent and were not always viewed in the same way as their parents (). Adolescents reported that key motivators included participating in “activities I like” and being motivated to “just go out and do it.” Parents felt a strong responsibility to encourage their adolescent to be involved but also felt they needed “pushing” or “forcing” at times, to get out the door (to attend). Most parents and adolescents described the strategy of having “people to do it with” were important to be, and keep being, involved. Key people could be a parent, friend or support person but was predominantly “Mum”. Adolescents and parents described the support and encouragement of friends and family increased motivation and confidence to attend and be involved:
So, I’ll have my father, my mother, my grandmother, slightly my sister, those sort of people and close friends. They can be coming and seeing me compete or giving me like good luck before the event or well done after the event. It makes me feel quite thankful that I’ve got a good close group of friends which I can actually trust, people I can trust (A).
A structured programme helps. He won’t do it otherwise because he’s not a physical person. If he’s doing something with friends, he’ll go along with them. I think it’d be great if my son realized that with effort, he could actually get better and get to a point where he could just about keep up with them as long as they weren’t doing anything major like sports (P).
I think if everyone’s going and you’ve got somewhere to go like you’re going to the park or looking for rocks. You know, it’s when he doesn’t think it’s exercise, when it’s actually to go and do something and it’s fun, as opposed to "Come on, we all need to get out and get some exercise in." (P)
She just doesn’t do anything. When she’s not involved, she’s just not participating. I think it upsets her. There’s activity she would love to do but she just doesn’t do it. I think nothing’s really helping with it. It’s just me pushing her to do it (P).
Interpretive description
The four themes highlight the experience of involvement in physical activity is personal, changeable and effortful; and relies on the desired context being supportive of ongoing participation. The onus cannot be placed solely on the adolescent or the parents. Strategies need to be developed and used to achieve personally optimal levels of involvement for each situation. With the help of key support people, adolescents living with cerebral palsy could (i) learn to understand and interpret their involvement continuum; and (ii) learn how to modify their personal levels of involvement to enhance their experience of physical activity. The roles of parents, health professionals, coaches, community organisations and supporters, could include being aware of variable involvement levels, what helps and hinders involvement, and the teaching of strategies and motivators that will foster helpful involvement levels for each adolescent.
Discussion
Rich accounts of the value and experience of being involved in physical activity were provided over the 13 months of the study. The detailed descriptions and interpretation of the experiences, and the diversity of past and present experiences reported by each adolescent and their parents confirmed the complex nature of involvement. The parents’ deep knowledge of their adolescents was clearly demonstrated as they could “see” involvement, however they often ascribed different meanings to what they saw in comparison to their adolescents’ interpretations.
For the eight adolescents living with cerebral palsy, being very involved was experienced when there was a high level of effort, concentration, readiness, and thought; highlighted by themes “Turning up is not enough” and “In it all the way.” Parents wanted their adolescents to be happy, to enjoy being active, and to participate with others. Enjoyment was less commonly reported by their children, as either experienced or as important. The theme, “Changes on a dime” (ranging from helpful to hindering levels of involvement) identified that finding optimal levels of involvement was challenging and despite encouragement, parents often had little influence. It was possible to be “too involved” resulting in a negative experience of frustration, exhaustion, and displeasure. Finding personal motivators and strategies “What works for me” to facilitate involvement were important to ensure ongoing participation in physical activity. Frequently described strategies to support involvement included choosing preferred activities, having more and new opportunities to try, having and using intrinsic motivation and having a key person, most often mum, actively encouraging participation.
Adolescents and their parents considered involvement as a critical factor when participating; involvement was key to being, and staying, active. Nyquist et al. also explored involvement using the fPRC to determine the experiences of 11 children with disabilities following a 3-week live-in adaptive physical activity programme [Citation26]. Consistent with our findings, being involved was valued beyond the physical gains (e.g., activity competence and skill mastery) and included increased motivation and sense-of-self attributes such as, confidence, self-efficacy, and relatedness [Citation26]. Children with disabilities involved in community and adaptive physical activity and sports programmes have reported similar positive experiences to those participating in the HLMP [Citation26–28]. Our qualitative findings support the construct of involvement as defined by Imms et al. [Citation1] and align well with the “quality participation elements” of “autonomy, belongingness, challenge, engagement, mastery, and meaning associated with participating” as identified by Martin Ginis [Citation7].
The “involvement continuum” suggests that it would be helpful for adolescents to learn what their personalised, optimal involvement levels are, to support their successful physical activity participation. Positive, helpful levels of involvement appeared to be an underlying requirement for ongoing participation; however, involvement could “change on a dime” because of “right now” or past experiences. Parents in this study reported that involvement in a physical activity may be high and have a positive effect when their adolescent was motivated, the activity involved a friend, was fun, and skills at the right challenge level were successfully achieved. However, the level of involvement may change within minutes while performing the same activity if it is too difficult or too easy, making the experience frustrating, causing the adolescent to lose focus and motivation, become disengaged, and no longer enjoy the experience. Understanding how much optimal involvement is enough to sustain participation is an important learning for each adolescent.
The rapidly changing experience of involvement highlights the importance of asking adolescents and parents frequently about their experiences of involvement within each activity and context and their involvement goal. It is important to consider that it is not possible to stay at high levels of involvement for long periods of time. The “flow state” has been well described as an optimal experience to achieve when active. The flow experience is one of total absorption and a sense of effortlessness. While there is often a desire to replicate the experience of flow it is not easy to achieve [Citation30]. McKenzie et al. also described a continuum of “finding the right balance” from “the right fit” through to “it’s all too hard” for adolescents and young people with childhood onset physical disability when describing exercise experiences [Citation31]. Social and environmental factors were found to have the strongest influence on participation in physical activity in those young people and adults. Providers of opportunities for physical activity should be mindful of such factors when adolescents are transitioning to adult activities and the importance of understanding the involvement continuum as unique to each person, context and environment.
Involvement is not just “having fun.” All the essential components of involvement should be considered when promoting participation in physical activity. Wiart [Citation32] stated “engagement in an enjoyable physical activity program is participation. If the physical activity is enjoyable and meaningful to the child and family, participation is an important outcome in itself”[Citation32]. In contrast, we found that involvement in physical activity was not always enjoyable for the adolescents with cerebral palsy in this study; yet participation was still desirable. For adolescents with cerebral palsy, a range of emotions might be experienced as part of involvement (e.g., satisfaction, joy, anger) as well as cognitive, affective, and behavioural aspects. Being involved required significant physical effort but also cognitive effort (e.g., thinking about skill execution, maintaining focus and concentration), trying to develop social connections, and being motivated while navigating the context and environment. The relationship between muscular endurance, physical capacity, and fatigue (general, cognitive, and total) is significant in adolescents with cerebral palsy and much greater than in their typically developing peers [Citation33]. The impact of fatigue and pain on involvement should not be underestimated, and is very common when living with cerebral palsy [Citation34]. Both cognitive and physical fatigue are likely to play a significant role in participation, and strategies to target both these aspects of fatigue should be addressed in combination [Citation35,Citation36].
The experiences of adolescents in this study supported the theorized bidirectional relationships of the fPRC of increased involvement when activities were preferred and competence was perceived as high [Citation1,Citation26]. However, the challenge for parents cannot be underestimated when non-attendance, low levels of effort, persistence and focus occurred to avoid being involved in non-preferred and difficult activities. As in the general population, exercise is of no interest to some children and adults with disabilities, and the prospect of participation in physical activity is associated with negative expectations, hindering involvement [Citation28,Citation37,Citation38]. A proportion of children and adults with disabilities describe themselves as “not being good enough” to participate in physical activity, which influences their likelihood of attendance and involvement [Citation29,Citation37].
Clinical implications
The findings of this study suggest that understanding the experiences and perspectives of adolescents and their parents of involvement may be important in clinical practice, as well as in community-based programmes. Consideration beyond the notion of enjoyment will need to be given to a broader range of elements and strategies to enhance ongoing involvement in physical activity. At an individual level, understanding involvement may be achieved by directly asking the adolescent (rather than, or as well as, their parent) about their experience of involvement, establishing their personal involvement continuum for each activity (including optimal level), and by setting specific involvement goals. In community and group settings, those supporting young people to participate in physical activity may need to pay more attention to ascertaining what constitutes optimal involvement for each adolescent during implementation of the programme and while attending. One adolescent may report “being optimally involved” occurs when with friends, the activity involves considerable effort, and when there is challenging competition. Another adolescent may prefer individual time, need external motivation and encouragement to get started and require high levels of focus to persist and achieve at their optimal involvement level.
Parents in this study felt a responsibility to find new and more opportunities for their adolescent while reporting a conflict between the need to encourage versus push participation in physical activity. The desire to promote participation while dealing with parental personal preferences and concerns (including inclusion, safety and suitability) appears to be a common challenge for parents of children with disabilities [Citation13,Citation39,Citation40]. Reducing factors that hinder and promoting factors that help involvement at an individual and family level, as well as at a system level have been recommended [Citation41,Citation42]. This may include provision of support, education and counselling from activity leaders (e.g., health professionals, coaches, trainers, teachers) directly to the parents/carers who are responsible for and encourage attendance and involvement of their young people [Citation43].
The adolescents reported getting started and staying involved in physical activity could be challenging. If clinicians, coaches and parent/carers can provide increased opportunities for positive experiences of optimal involvement and assist adolescents to recognise the components that are most important for themselves, participation may be more valued, with an increased likelihood of sustained involvement. Addressing “turning up” and “keeping up” before the known decline in physical activity participation in adolescents with cerebral palsy appear to be important starting points [Citation43–46].
Strengths and limitations
Analysis of multiple sources of information from interviews, audit trails, and journaling of qualitative findings provided breadth and depth of insight into during the analysis and interpretation of the data. The high rate of data collection and longitudinal collection was a strength. Four of the 12 parents who contributed to the involvement findings were fathers which provided more diversity of experiences than is commonly seen in research with parents. This depth of engagement resulted in detailed descriptions and interpretation of the experiences of both adolescents and parents.
The voice of adolescents with cerebral palsy was limited to those aged 11–16 who are ambulant (GMFCS I-II) and who could verbally communicate their experiences (CFCS I-II). Only one female adolescent participated, limiting the transferability of findings. Being the only female may also have influenced her HLMP experiences, and she subsequently only attended 2/24 sessions. Reduced recreational, skill based and active physical participation in female adolescents with disabilities [Citation48,Citation49] highlights the need to understand and further explore the experiences of involvement in physical activity for this group. A targeted approach such as a female only multi-sport camp, with a social focus, may be one option [Citation50].
Transferability
The study was directed at understanding involvement in physical activity across any setting for adolescents with cerebral palsy. The transferability of the themes to different contexts and environments should be considered in light of the context of this study. The experiences of involvement are likely to vary dependent on the task, for example, doing homework compared to playing a game of basketball, and dependent on the place e.g., school compared to home. Determining effective strategies to promote and measure involvement in all contexts, environments and for individuals with cerebral palsy who are not adolescents, and those who require assistance with mobility and communication, requires further research. The findings may have also differed if the research questions were framed using the fPRC with a different starting point: for example, “How do preferences influence involvement in physical activity now and into the future?”
Future research
The new knowledge gleaned by this research may be a useful starting point for further research addressing “in the moment” outcome measures and strategies generated by both adolescents and their parents to enhance involvement. Measures of real-world, self-report experiences need to be developed [Citation6,Citation9,Citation51]. Measures need to consider the complexity of involvement to tap cognitive, affective and behavioural aspects of the experience as it pertains to an individuals’ context and what is meaningful involvement for them: that is, we need to be able to capture their personalised involvement continuum. Measurement ideas to consider include an adolescent reviewing themselves in action (from video footage) or commentating “live” when active on their involvement experience. These personalised approaches would ensure involvement was person-centred and person-driven. Self-report of involvement has been used successfully with children who have autism spectrum disorder [Citation52], and disengaged high school students in physical education classes [Citation53]. In the moment measurement of involvement may negate the need for proxy reporting with long recall periods and would expand reporting beyond enjoyment [Citation3].
Future research may also focus on assisting young people to learn self-awareness, self-regulation and self-management strategies to help with changeable involvement levels i.e., to move from hindering to helpful levels of involvement. This is important if an individual’s in-the-moment responses are detrimental to being and staying active over the life course.
The influence of environment on physical activity involvement outcomes should also be addressed [Citation42]. There is growing evidence supporting environmental approaches to increasing participation [Citation54,Citation55], but direct measures of involvement are not always included in the studies to date.
Inclusion of a more diverse sample of people (ages, gender and ability levels) would enhance our current understanding of the role of involvement in physical activity, in different contexts and environments. A life course approach using a longitudinal study design to explore past and present involvement experiences is recommended.
Conclusion
“Being involved” in physical activity was experienced as complex and dynamic by the adolescents with cerebral palsy and their parents in this study. Four key themes were identified: “Turning up is not enough” (“There’s no point being there if you’re not involved”); “In it all the way”, “Changes on a dime”, and “What works for me.” Focusing on enjoyment as the only valid experience of involvement undermines the effort, focus and concentration required to achieve the optimal level of involvement for each activity. Perceptions of involvement varied between adolescents and parents, making finding effective motivators and strategies challenging. Lifelong participation in physical activity may be enhanced by learning to regulate the personal involvement continuum.
Authors contributions
GK delivered the high-level mobility intervention, conducted the interviews, coded, compared and interpreted the data for analysis, developed themes and wrote the paper. CI, SS, BA, MS and AH were involved in the design of the research, interpreting the data, drafting, and review of the paper.
Supplemental Material
Download PDF (175.5 KB)Acknowledgements
The authors would like to acknowledge the eight adolescents and their families for their commitment to this research over a 13 month period including a three month period of COVID lockdown in New Zealand. Thank you to Jacky Lipson for assisting with the involvement graphics. GK would like to acknowledge the contribution of the Australian Commonwealth Government for support through an Australian Government Research Training Program Scholarship during her PhD at the Australian Catholic University and the University of Melbourne.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Imms C, Granlund M, Wilson PH, et al. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. 2017;59(1):16–25. doi: 10.1111/dmcn.13237.
- Imms C, Adair B, Keen D, et al. Participation’: a systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev Med Child Neurol. 2016;58(1):29–38. doi: 10.1111/dmcn.12932.
- Kilgour G, Adair B, Stott NS, et al. Do physical activity interventions influence subsequent attendance and involvement in physical activities for children with cerebral palsy: a systematic review. Disabil Rehabil. 2022;44(9):1682–1698. doi: 10.1080/09638288.2021.1909151.
- Quartermaine JR, Rose TA, Auld ML, et al. Participation measures that evaluate attendance and involvement for young people aged 15 to 25 years with cerebral palsy: a systematic review. Disabil Rehabil. 2023;2023:1–17. doi: 10.1080/09638288.2023.2207042.
- Liao Y-T, Hwang A-W, Liao H-F, et al. Understanding the participation in home, school, and community activities reported by children with disabilities and their parents: a pilot study. Int J Environ Res Public Health. 2019;16(12):2217. doi: 10.3390/ijerph16122217.
- Adair B, Ullenhag A, Rosenbaum P, et al. Measures used to quantify participation in childhood disability and their alignment with the family of participation-related constructs: a systematic review. Dev Med Child Neurol. 2018;60(11):1101–1116. doi: 10.1111/dmcn.13959.
- Martin Ginis KA, Evans MB, Mortenson WB, et al. Broadening the conceptualization of participation of persons with physical disabilities: a configurative review and recommendations. Arch Phys Med Rehabil. 2017;98(2):395–402. doi: 10.1016/j.apmr.2016.04.017.
- Shirazipour CH, Evans MB, Leo J, et al. Program conditions that foster quality physical activity participation experiences for people with a physical disability: a systematic review. Disabil Rehabil. 2020;42(2):147–155. doi: 10.1080/09638288.2018.1494215.
- Resch C, Van Kruijsbergen M, Ketelaar M, et al. Assessing participation of children with acquired brain injury and cerebral palsy: a systematic review of measurement properties. Dev Med Child Neurol. 2020;62(4):434–444. doi: 10.1111/dmcn.14465.
- Gates PE, Banks D, Johnston TE, et al. Randomized controlled trial assessing participation and quality of life in a supported speed treadmill training exercise program vs. a strengthening program for children with cerebral palsy. J Pediatr Rehabil Med. 2012;5(2):75–88. doi: 10.3233/PRM-2012-0199.
- Reedman SE, Johnson E, Sakzewski L, et al. Sedentary behavior in children with cerebral palsy between 1.5 and 12 years: a longitudinal study. Pediatr Phys Ther. 2020;32(4):367–373. doi: 10.1097/PEP.0000000000000740.
- Verschuren O, Peterson MD, Balemans AC, et al. Exercise and physical activity recommendations for people with cerebral palsy. Dev Med Child Neurol. 2016;58(8):798–808. doi: 10.1111/dmcn.13053.
- Schiariti V, Sauve K, Klassen AF, et al. ‘He does not see himself as being different’: the perspectives of children and caregivers on relevant areas of functioning in cerebral palsy. Dev Med Child Neurol. 2014;56(9):853–861. doi: 10.1111/dmcn.12472.
- Kilgour G, Stott NS, Steele M, et al. Effects of a 12-week community-based high-level mobility program on sustained participation in physical activity by adolescents with cerebral palsy: A single subject research design study. Disabil Rehabil. 2023. doi: 10.1080/09638288.2023.2256225.
- Thompson Burdine J, Thorne S, Sandhu G. Interpretive description: a flexible qualitative methodology for medical education research. Med Educ. 2021;55(3):336–343. doi: 10.1111/medu.14380.
- Thorne S. What can qualitative studies offer in a world where evidence drives decisions? Asia Pac J Oncol Nurs. 2018;5(1):43–45. doi: 10.4103/apjon.apjon_51_17.
- Thorne S, Kirkham SR, MacDonald-Emes J. Interpretive description: a noncategorical qualitative alternative for developing nursing knowledge. Res Nurs Health. 1997;20(2):169–177. doi: 10.1002/(SICI)1098-240X(199704)20:2<169::AID-NUR9>3.0.CO;2-I.
- Brewer KM, Harwood ML, McCann CM, et al. The use of interpretive description within kaupapa māori research. Qual Health Res. 2014;24(9):1287–1297. doi: 10.1177/1049732314546002.
- Palisano RJ, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214–223. doi: 10.1111/j.1469-8749.1997.tb07414.x.
- Archibald MM, Caine V, Ali S, et al. What is left unsaid: an interpretive description of the information needs of parents of children with asthma. Res Nurs Health. 2015;38(1):19–28. doi: 10.1002/nur.21635.
- O’Brien BC, Harris IB, Beckman TJ, et al. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi: 10.1097/ACM.0000000000000388.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi: 10.1093/intqhc/mzm042.
- Guthold R, Stevens GA, Riley LM, et al. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1· 6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35. doi: 10.1016/S2352-4642(19)30323-2.
- Eliasson AC, Krumlinde-Sundholm L, Rösblad B, et al. The manual ability classification system (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol. 2006;48(7):549–554. doi: 10.1017/S0012162206001162.
- Hidecker MJC, Paneth N, Rosenbaum PL, et al. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. 2011;53(8):704–710. doi: 10.1111/j.1469-8749.2011.03996.x.
- Nyquist A, Jahnsen RB, Moser T, et al. The coolest I know–a qualitative study exploring the participation experiences of children with disabilities in an adapted physical activities program. Disabil Rehabil. 2020;42(17):2501–2509. doi: 10.1080/09638288.2019.1573937.
- Bragg E, Spencer NLI, Phelan SK, et al. Player and parent experiences with child and adolescent power soccer sport participation. Phys Occup Ther Pediatr. 2020;40(6):637–650. doi: 10.1080/01942638.2020.1746946.
- Downs M, MacDermid J, Connelly D, et al. Current experiences and future expectations for physical activity participation: perspectives of young people with physical disabilities and their rehabilitation clinicians. Dev Neurorehabil. 2021;24(2):73–84. doi: 10.1080/17518423.2020.1771787.
- Lauruschkus K, Nordmark E, Hallström I. “It’s fun, but…” children with cerebral palsy and their experiences of participation in physical activities. Disabil Rehabil. 2015;37(4):283–289. doi: 10.3109/09638288.2014.915348.
- Nakamura J, Csikszentmihalyi M. The concept of flow. Flow and the foundations of positive psychology. Chicago: Springer; 2014. p. 239–263.
- McKenzie G, Willis C, Shields N. Barriers and facilitators of physical activity participation for young people and adults with childhood-onset physical disability: a mixed methods systematic review. Develop Med Child Neuro. 2021;63(8):914–924. doi: 10.1111/dmcn.14830.
- Wiart L. How do we ensure sustainable physical activity options for people with disabilities? Dev Med Child Neurol. 2016;58(8):788–788. doi: 10.1111/dmcn.13100.
- Eken MM, Houdijk H, Doorenbosch CAM, et al. Relations between muscle endurance and subjectively reported fatigue, walking capacity, and participation in mildly affected adolescents with cerebral palsy. Dev Med Child Neurol. 2016;58(8):814–821. doi: 10.1111/dmcn.13083.
- Lindsay S. Child and youth experiences and perspectives of cerebral palsy: a qualitative systematic review. Child Care Health Dev. 2016;42(2):153–175. doi: 10.1111/cch.12309.
- Kumar R, Smith M. The effect of muscle endurance and fatigue on participation in adolescents with cerebral palsy. Dev Med Child Neurol. 2016;58(8):789–789. doi: 10.1111/dmcn.13142.
- Dutia I, Eres R, Sawyer SM, et al. Fatigue experienced by people with cerebral palsy: a systematic review of assessment tools and decision tree. Disabil Rehabil. 2023;2023:1–9. doi: 10.1080/09638288.2023.2205175.
- Ives B, Clayton B, Brittain I, et al. I’ll always find a perfectly justified reason for not doing it’: challenges for disability sport and physical activity in the United Kingdom. Sport Soc. 2019;2019:19.
- Wright A, Roberts R, Bowman G, et al. Barriers and facilitators to physical activity participation for children with physical disability: comparing and contrasting the views of children, young people, and their clinicians. Disabil Rehabil. 2019;41(13):1499–1507. doi: 10.1080/09638288.2018.1432702.
- Lauruschkus K, Nordmark E, Hallström I. Parents’ experiences of participation in physical activities for children with cerebral palsy – protecting and pushing towards independence. Disabil Rehabil. 2017;39(8):771–778. doi: 10.3109/09638288.2016.1161841.
- Atchison B-J, Goodwin DL. “My child may be ready, but I am not”: parents’ experiences of their children’s transition to inclusive fitness settings. Adapt Phys Activ Q. 2019;36(2):282–301. doi: 10.1123/apaq.2018-0101.
- Martin Ginis KA, Ma JK, Latimer-Cheung AE, et al. A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol Rev. 2016;10(4):478–494. doi: 10.1080/17437199.2016.1198240.
- Quartermaine JR, Rose TA, Auld ML, et al. Factors impacting positive and negative participation of young people with cerebral palsy: a Delphi study of consumers and health professionals. Disabil Rehabil. 2023;2023:1– 9. doi: 10.1080/09638288.2023.2194062.
- Arakelyan S, Maciver D, Rush R, et al. Family factors associated with participation of children with disabilities: a systematic review. Dev Med Child Neurol. 2019;61(5):514–522. doi: 10.1111/dmcn.14133.
- Baksjoberget PE, Nyquist A, Moser T, et al. Having fun and staying active! Children with disabilities and participation in physical activity: a follow-up study. Phys Occup Ther Pediatr. 2017;37(4):347–358. doi: 10.1080/01942638.2017.1281369.
- Imms C, Froude E, Adair B, et al. A descriptive study of the participation of children and adolescents in activities outside school. BMC Pediatr. 2016;16(1):84. doi: 10.1186/s12887-016-0623-9.
- Shikako-Thomas K, Shevell M, Lach L, et al. Are you doing what you want to do? Leisure preferences of adolescents with cerebral palsy. Dev Neurorehabil. 2015;18(4):234–240. doi: 10.3109/17518423.2013.794166.
- Shimmell LJ, Gorter JW, Jackson D, et al. It’s the participation that motivates him: physical activity experiences of youth with cerebral palsy and their parents. Phys Occup Ther Pediatr. 2013;33(4):405–420. doi: 10.3109/01942638.2013.791916.
- Imms C, Adair B. Participation trajectories: impact of school transitions on children and adolescents with cerebral palsy. Dev Med Child Neurol. 2017;59(2):174–182. doi: 10.1111/dmcn.13229.
- King G, McDougall J, Dewit D, et al. Predictors of change over time in the activity participation of children and youth with physical disabilities. Child Health Care. 2009;38(4):321–351. doi: 10.1080/02739610903237352.
- Guest L, Balogh R, Dogra S, et al. Examining the impact of a multi-sport camp for girls ages 8–11 with autism spectrum disorder. Ther Recreat J. 2017;51(2):109–126. doi: 10.18666/TRJ-2017-V51-I2-7383.
- Aubert S, Brazo-Sayavera J, González SA, et al. Global prevalence of physical activity for children and adolescents; inconsistencies, research gaps, and recommendations: a narrative review. Int J Behav Nutr Phys Act. 2021;18(1):2. doi: 10.1186/s12966-021-01155-2.
- Simpson K, Imms C, Keen D. The experience of participation: eliciting the views of children on the autism spectrum. Disabil Rehabil. 2022;44(9):1700–1708. doi: 10.1080/09638288.2021.1903100.
- Casey A, Jones B. Using digital technology to enhance student engagement in physical education. Asia-Pac J Health, Sport Phys Educat. 2011;2(2):51–66. doi: 10.1080/18377122.2011.9730351.
- Anaby D, Avery L, Gorter JW, et al. Improving body functions through participation in community activities among young people with physical disabilities. Dev Med Child Neurol. 2020;62(5):640–646. doi: 10.1111/dmcn.14382.
- Anaby DR, Law M, Feldman D, et al. The effectiveness of the pathways and resources for engagement and participation (PREP) intervention: improving participation of adolescents with physical disabilities. Dev Med Child Neurol. 2018;60(5):513–519. doi: 10.1111/dmcn.13682.