
Abstract
Purpose
The aim of this review was to synthesise qualitative literature on physical activity experiences of community-dwelling older adults with physical disabilities.
Methods
We conducted a scoping review of peer-reviewed, qualitative studies on physical activity with community-dwelling older adults with physical disabilities. We analysed eligible studies identified through electronic database searches (CINAHL Complete, MEDLINE, SPORTDiscus) and manual searches undertaken up to June 2023.
Results
Twenty-eight articles with 306 participants were included. As regard the experience of physical activity, although physical activity could elicit pleasure and enjoyment, many reported that physical activity sometimes produced pain. Various outcomes of physical activity were reported, with several physical, psychological, social, and lifestyle benefits prominent. Analyses of barriers and facilitators demonstrated how intrapersonal, interpersonal, environmental, and systems and programme factors influenced physical activity participation among older adults with physical disabilities.
Discussion
Our findings contribute to literature on physical activity in older adults with physical disabilities by synthesising qualitative research on physical activity experiences, outcomes, barriers, and facilitators in this population. Findings demonstrate the need for knowledgeable and supportive healthcare and exercise professionals, environments that support physical activity, and activities that promote pleasure and social connections.
Physical activity is perceived to have wide-ranging benefits for community-dwelling older adults with physical disabilities.
Various intrapersonal, interpersonal, environmental, and systems and programme barriers constrain physical activity in physically disabled people.
Knowledgeable and supportive healthcare and exercise professionals, accessible environments, and activities that promote pleasure and social connections could enhance engagement in physical activity.
Implications for Rehabilitation
Introduction
Engagement in physical activity can be beneficial for physical health and psychosocial wellbeing for disabled people [Citation1,Citation2]. Furthermore, physical activity can improve disabled peoples’ quality of life and functional independence [Citation3], expand social networks [Citation4], and promote positive affective states [Citation5]. Despite the well-documented benefits of physical activity, disabled people are less physically active than non-disabled people [Citation1,Citation6,Citation7]. Reasons for lower levels of physical activity among disabled people are complex, but barriers to physical activity can include intrapersonal (e.g., psychological factors), interpersonal (e.g., social support), environmental (e.g., facilities), and policy-level (e.g., health policies) factors [Citation8,Citation9]. Consequently, there is a need to address inequalities and inequities, and possible barriers, to increase physical activity and quality of life among disabled people.
The quantity of people with disabilities increases with age, and older people are represented disproportionately in disabled populations [Citation10]. In the United Kingdom, for example, the most recently reported assessment of household circumstances (2020/2021) indicated that at least one-third of older adults (≥ 65 years old) in various age groups (65–69 years old = 35%; 70–74 years old = 39%; 75–79 years old = 43%; 80+ years old = 59%) reported a disability, a figure that was considerably higher than younger adults (21%) and children (8%) [Citation11]. Furthermore, the United Nations [Citation12] estimate that more than 46% of older adults globally have a disability. Although a significant proportion of disabled people are insufficiently active across all age groups, the prevalence of those not meeting physical activity guidelines is greatest among older adults [Citation7]. With rapid growth expected in the numbers of disabled people [Citation13] and older adults [Citation14] in the global population in the coming decades, there is an urgent need for effective policies and practices that support engagement in physical activity. Ultimately, more effective strategies will increase the number of disabled older adults that can accrue the many physical and psychosocial benefits physical activity can offer.
Although significant attention has been directed towards quantifying physical activity in disabled people, in recent years there has been increased recognition of the need to consider the quality of disabled peoples’ participation experiences in physical activity [Citation15]. Within the context of physical disability, full participation in physical activity does not solely concern having access to relevant opportunities and programmes, it also entails having quality experiences [Citation16]. Following a systematic, configurative review of experiential characteristics of ‘participation’ (i.e., involvement in life situations) [Citation17], Martin Ginis et al. [Citation16] proposed six characteristics of quality participation experiences in disabled people: autonomy; belongingness; challenge; engagement; mastery; and meaning. Programme conditions that can facilitate such quality participation experiences include group-based programmes for people with similar disabilities, which can bring a sense of belonging and foster mastery, as well as exercise leaders that have strong physical activity and disability-specific knowledge [Citation18].
With increased attention being directed towards the quality of disabled peoples’ experiences in physical activity, further exploration of the experiences of disabled older adults in physical activity is warranted. To date, existing reviews of literature on aspects of disabled adults’ experiences in physical activity (e.g., barriers, facilitators, experiences) have combined middle-aged and older adult samples [Citation2,Citation18,Citation19]. Questions remain, however, about physical activity experiences specifically among older adults. Given that a broad range of factors influence physical activity engagement [Citation9] and differences exist in physical activity levels between middle-aged and older disabled adults [Citation7], it is important to direct further attention towards the participation experiences of older adults, as well as barriers and facilitators, which may vary across the lifespan.
The most prevalent disability reported among older adults is physical disability [Citation11]. Thus, interventions designed to promote physical activity among this group could have the potential for wide reach. To develop alternative and improved interventions to promote physical activity for older adults with physical disabilities, it would be valuable to explore current understanding of their lived experiences of engaging in physical activity and factors that influence participation. One way to achieve this is to systematically map and summarise the available qualitative literature on this topic through a scoping review [Citation20]. A scoping review of qualitative literature on the physical activity experiences of older adults with physical disabilities could make a valuable contribution to the literature as previous reviews of qualitative research have combined older adults with adults in early and middle adulthood [Citation2,Citation21]. Although such reviews can be valuable, by focusing specifically on qualitative research pertaining to older adults with physical disabilities, this could provide more granular insights into experiences of physical activity among this population and specific factors that influence engagement. In turn, this could provide a more robust platform to improve policy, practice, and interventions designed to promote physical activity among older adults with physical disabilities in future.
Purpose of the review
In this scoping review, we aimed to systematically map and summarise the available qualitative literature on physical activity experiences of community-dwelling older adults with physical disabilities. The overarching review question was: What is known from qualitative evidence about physical activity experiences in older adults with physical disabilities? In addressing our overarching research question, our specific objectives were to: (1) describe experiences in physical activity of community-dwelling older adults with physical disabilities; and (2) identify factors that influence participation in this population.
Method
Review protocol
We used the 5-step framework for scoping reviews [Citation22] and suggestions for enhancing this framework [Citation23,Citation24] to address our objectives. Our review was reported in accordance with the PRISMA Extension for Scoping Reviews [Citation25] (PRISMA-ScR; see Supplementary File 1). The review protocol was deposited on the Open Science Framework website (https://osf.io/bdegr/) before the first database searches in June 2022. We updated the protocol in June 2023 to accommodate additional search terms.
Identifying relevant studies
To be included in the review, studies needed to be: (a) original, empirical studies containing qualitative data; and (b) present data on physical activity in community-dwelling older adults (defined as 65 years or over) with a physical disability or physical/mobility impairment. For studies that combined older adults with younger people, we included a study if the mean age for participants was ≥ 65 years old, or specific data pertaining to older adults could be identified and extracted (e.g., quotations). Physical activity was defined as any bodily movement produced by skeletal muscles that requires energy expenditure [Citation26]. Thus, studies focused on sports participation, physical activity, exercise, or any equivalent were included. Studies were excluded if: (a) they were not written in the English language; (b) recruited participants living in an acute or long-term care setting or a population with a specific condition (e.g., stroke, Parkinson’s disease) in which there was no explicit evidence of a physical/mobility impairment or disability; or (c) if they focused on rehabilitation (e.g., from a hip fracture) and did not make explicit reference to long-term physical/mobility impairment or disability. In studies with older adults with Parkinson’s disease, if the authors reported data classifying the symptoms of the disease based on Hoehn and Yahr’s [Citation27] scale, we included participants that were classified as being at stage 3 of the disease or higher, as this is indicative of at least “mild-to-moderate” (p. 433) impairment.
Study selection
The search strategy was developed by the first author, who had extensive experience of conducting database searching, in consultation with the other authors. The search terms were shaped by previous reviews of research with disabled people [Citation21] and pilot searches. The first author conducted systematic searches of three electronic databases (CINAHL Complete; MEDLINE; and SPORTDiscus) on three occasions (June 2022-June 2023), with the final search conducted on June 30th, 2023. Adopting principles from the SPIDER heuristic [Citation28], the search string included five blocks of Boolean search terms (see Supplementary File 2) related to the: Sample (physical disability and older adults); Phenomenon of Interest (physical activity); Research Design and Type (qualitative and mixed methods studies including qualitative research); and Evaluation (experience and other relevant terms). Where possible, additional subject terms (e.g., Medical Subject Headings [MeSh] in MEDLINE, Descriptors in PsycINFO) were also used (see Supplementary File 2 for full electronic database searches for each database). All searches were limited to records published in the English language. Additional records were identified through manual screening of the reference list of more than 10 past reviews focused on disability and physical activity (see Supplementary File 2), as well as screening titles of backward and forward citations (Google Scholar) for studies included in the review. All records identified through these search processes were exported to EndNote X9. We removed duplicates through the automatic de-duplication feature and manual screening. All members of the research team engaged in some stage of the screening process. Each record was screened independently by two of these authors at the title and abstract stage. Once the decisions reached by each author were compared, a meeting took place to resolve any discrepancies. The remaining records were checked for eligibility at full text by two authors independently. After completing this process, both authors met to discuss their decisions, resolve any discrepancies, and agree reasons for excluding articles at the full-text stage. In the event of any uncertainties, a third author was consulted and contributed to the decision making.
Data charting
We developed a data charting table collating information relevant to the review. The data charting table included information on the: authors; publication year; study objectives; study design; study characteristics; sample characteristics; physical activity protocol (e.g., type, dose, intensity, duration, setting, supervision); and theoretical framework/topic of interest. Data were extracted and cross-checked by two authors (PJ and GM).
Collating, summarising, and reporting results
We followed the 3-step process recommended by Levac et al. [Citation24] for collating, summarising, and reporting results of scoping reviews. First, the lead author led a content analysis [Citation29] to summarise all qualitative data (i.e., author interpretations, participant quotes, tables, figures) in the results or findings of included studies pertaining to experiences of older adults with physical disabilities in physical activity. The remaining authors, all of whom had different disciplinary expertise (e.g., public health, sociology, health and social care) and/or practical experience (e.g., as physical activity professionals), acted as ‘critical friends’ [Citation30] and provided additional and alternative perspectives on the first author’s interpretations through regular meetings of the research team. Second, findings generated from the included studies were organised and reported in accordance with our research questions. Finally, we considered the overall meaning of the results in relation to our research question and the implications of this for research and practice. This process was enhanced by discussing our findings with individuals with relevant lived experiences (e.g., older citizens, healthcare professionals) prior to submitting for peer review.
Results
In total, 5951 records were retrieved through our database and manual searches, with 28 articles meeting our eligibility criteria being included in the review (see Supplementary File 3 for full screening process outcomes). In the following sections, we first describe the included studies, before summarising the key findings. The synthesised charting form detailing contextual information for all studies is presented in .
Table 1. Extracted information on the included studies.
Description of included studies
Study design characteristics
The primary objective in most studies could be broadly classified as seeking to understand perceptions and experiences of physical activity (k = 19) or factors influencing participation in physical activity (e.g., barriers, enablers/facilitators/motivators) (k = 9). Seven studies reported a theoretical framework. Data were collected across the included studies via interviews (k = 21), focus groups (k = 5), or a combination of the two (k = 2). Data were most commonly analysed using thematic analysis (k = 11) and content analysis (k = 5).
Participant characteristics
Of the 306 eligible participants in the included studies, their gender or sex was reported as female (n = 160), woman (n = 41), male (n = 75), or man (n = 17). Only 13 of the 15 participants in the study by McKevitt et al. [Citation52] were eligible and while specific information on gender for these participants were not reported, 80% of the overall sample were female. The studies took place in 11 developed countries, with the highest number taking part in the United Kingdom (k = 8), New Zealand (k = 4), and Canada (k = 3). Most studies recruited participants with some form of arthritis (k = 17). Other participants were reported to have physical impairments due to Parkinson’s disease (k = 3) or had lower-limb amputations (k = 2).
Physical activity characteristics
Most studies explored participants’ experiences of physical activity in general (k = 12) or in a specific exercise programme that involved strength, functional movement, or balance training (k = 12). Other studies included water-based programmes (k = 3) or dance (k = 1).
Narrative summary of findings
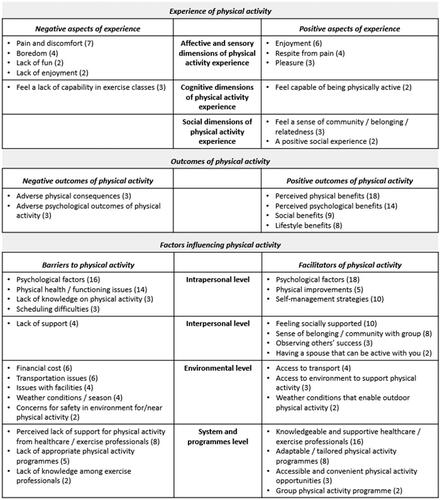
Based on our analysis of content reported within studies included in our review, we structured the main findings into four domains: experience of physical activity, which captured content interpreted as representing the experiences of participants during physical activity; outcomes of physical activity, which focused on perceived consequences of engaging in physical activity (i.e., after the activity); barriers to physical activity; and facilitators of physical activity. Drawing on social-ecological perspectives of health promotion [Citation56], we organised our analyses of barriers and facilitators to physical activity into four categories: intrapersonal factors; interpersonal factors; environmental factors; and system and programme factors. provides a visual representation of findings for which there was cross-study evidence (i.e., ≥ two studies). Sources for findings presented in the following sections are detailed in Supplementary File 4.
Figure 1. Summary of findings for each category in the scoping review. Note: The numbers indicate the total amount of sources for each finding.
Experience of physical activity
Content concerning the experience of physical activity was divided into negative and positive aspects of the physical activity experience. For each of these, we present evidence in relation to three categories (italicised in the text): (a) affective and sensory dimensions, (b) cognitive dimensions (i.e., how people think, including social cognition), and (c) social dimensions (i.e., interactions between individuals and groups) of the physical activity experience.
Positive aspects of the physical activity experience
Regarding the positive affective and sensory dimensions of the physical activity experience, four studies described how the experience of physical activity evoked pleasure. For some, this feeling of pleasure was attributed to exercising in a group [Citation35] or relaxation of the mind [Citation59], while aqua-based movement was also described as a pleasant form of physical activity for those with arthritis [Citation38,Citation42]. Participants across several studies reported that physical activity was enjoyable (k = 6) and that being physically active provided respite from pain (k = 4). For cognitive dimensions of the physical activity experience, two studies reported that participants felt capable of being physically active. Finally, positive social dimensions of the physical activity experience included that group physical activity was a positive social experience (k = 2) and that this type of physical activity fostered a sense of belonging and relatedness (k = 3).
Negative aspects of physical activity experience
Pain and discomfort were widely reported (k = 7) as unpleasant affective and sensory dimensions of the physical activity experience. Within this category, there was also cross-study evidence that physical activity could be boring/tedious (k = 4) or lacking in fun (k = 2) or enjoyment (k = 2). The most commonly-reported negative cognitive dimension of the physical activity experience was feeling a lack of capability in exercise classes (k = 3). This represented how participants felt less capable of performing certain exercises or how they struggled to “keep up” with the remainder of a group. Only one study reported negative social dimensions of the physical activity experience. Lange et al. [Citation46] reported that participants felt some individuals might not feel connected to others in a physical activity programme, but also outlined that some preferred exercising individually.
Outcomes of physical activity
Positive outcomes of physical activity
A range of positive outcomes of physical activity were reported across the included studies. Perceived physical benefits of physical activity were reported in 18 studies. Such physical benefits included perceived improvements in physical function/fitness (k = 11) and physical health (k = 5), as well as the soothing of pain, which was reported specifically in older adults with arthritis (k = 5). Psychological benefits of physical activity included that it contributed to improved perceptions of mental health and wellbeing (k = 10) and increased/maintained confidence (k = 6), primarily to be more active (k = 5). Other less-frequently identified psychological benefits were that physical activity can be a distraction from one’s condition (k = 2) and can elicit positive changes in attitude (k = 2). Social benefits of physical activity participation, reported across nine studies, included that group physical activity could be an opportunity for social interactions (k = 7) and could reduce feelings of isolation (k = 4). Eight studies also reported lifestyle benefits because of physical activity, with cross-study evidence that engaging in physical activity could make activities of daily living easier (k = 3).
Negative outcomes of physical activity
Although outcomes of physical activity were overwhelmingly positive, some negative consequences were reported. In terms of adverse psychological outcomes, for some, physical activity evoked unpleasant emotions (k = 3), such as feelings of guilt, due to not being active enough, and frustration, due to being given sub-optimal physical activity information and feeling physical activity was a chore. Some participants explained that a by-product of the process of partaking in physical activity was the stress of organising and waiting for transport [Citation35]. The most common adverse physical consequence was pain following physical activity (k = 2).
Barriers to physical activity
Intrapersonal factors
Psychological barriers to physical activity were reported across 16 studies. Widely-cited psychological barriers included lack of motivation (k = 7), fear of falling or concerns about safety (k = 6), and a perceived lack of capability/confidence (k = 5). In addition, there was evidence across multiple studies that poor mental health (k = 3), unpleasant past experiences in physical activity (k = 3), mental fatigue (k = 2), and fear of pain during/after physical activity (k = 2) represented barriers to physical activity. Physical health/functioning barriers, reported across 14 studies, most commonly encompassed reduced/ill health (k = 9), physical function limitations due to condition (k = 8), pain and injury (k = 7), and limited energy and fatigue (k = 4). Two studies also reported evidence that risk of medical complications/side effects of medication were barriers. Other intrapersonal issues of note included scheduling difficulties (k = 3) and lack of knowledge about physical activity (e.g., whether it is appropriate or not) (k = 3).
Interpersonal factors
Four studies reported factors classified as interpersonal barriers to physical activity. The only interpersonal barrier for which there was cross-study evidence was a perceived lack of support (k = 4), which could be due to inadequate personal support networks or due to not having an exercise partner.
Environmental factors
Twelve studies reported environmental barriers to physical activity. Financial cost (k = 6) and transportation issues (k = 6) were the most widely-reported barriers. Environmental barriers also pertained to issues with facilities (e.g., lack of accessible, user-friendly facilities - k = 4) and weather conditions/season (k = 4), such that cold temperatures, poor weather, and darkness in winter constrained physical activity. Concerns for safety in the environment for physical activity or near a physical activity facility were also reported (k = 2).
System and programme-level factors
Eleven studies reported barriers to physical activity that could be classified as pertaining to systems and programmes (e.g., programme content and personnel). A consistent issue identified was a perceived lack of support for physical activity from healthcare/exercise professionals (k = 8). This sub-category was epitomised by a lack of advice/guidance, and sometimes conflicting messaging, from healthcare professionals about physical activity. Other barriers at the system and programme levels included a lack of appropriate physical activity programmes (k = 5) and limited disability-specific knowledge among exercise professionals (k = 2).
Facilitators to physical activity
Intrapersonal factors
A total of 21 studies reported intrapersonal facilitators for physical activity. Psychological factors were most commonly cited (k = 18), with prominent facilitators reported including a motive to preserve health and functional independence (k = 10), pleasure and enjoyment of physical activity (k = 6), and developing knowledge-capability and self-efficacy (k = 3). Participants also reported the benefits of self-management strategies (k = 10), with physical activity facilitated by being careful and taking precautions, and making physical activity part of one’s day and/or routine. Perceiving physical improvements (e.g., improved functioning, reduced pain) also supported physical activity (k = 5), with such improvements holding the potential to motivate participants.
Interpersonal factors
Eighteen studies reported interpersonal facilitators of physical activity. Feeling socially supported was a widely reported facilitator (k = 10), with such support stemming from friends, family, and peers (i.e., as part of a physical activity group). Similarly, the positive impact of feeling a sense of belonging/community within a physical activity group was reported across eight studies. A common thread within this sub-category was the perception among participants that being part of a homogenous group of people (e.g., people with similar impairments or conditions) enabled participants to feel as though they had similar capabilities to other participants and that this also provided an opportunity for them to benefit from mutual support due to their shared experiences. Participants also spoke of the benefits of observing others’ success (k = 3) and having a spouse that can be active with you (k = 2).
Environmental factors
Environmental facilitators to physical activity were reported in 11 studies. Four studies also reported that having access to transport was a facilitator of physical activity. There was cross-study evidence of the benefits of access to environments structured to support physical activity (k = 3) and weather conditions that enable outdoor physical activity (k = 2).
System and programme-level factors
A total of 20 studies reported factors that could facilitate physical activity and were categorised as being at system and programme levels. The importance of knowledgeable and supportive healthcare and exercise professionals to facilitate physical activity was widely reported (k = 16). Participants consistently acknowledged the importance of working with knowledgeable and trained professionals, who provided individualised support that accounted for the specific needs of participants, including through adapting activities. Moreover, a further facilitator of physical activity cited was adaptable/tailored physical activity programmes (k = 8). Multiple studies highlighted the importance of tailoring physical activity to the individual and implementing safe and effective guidelines specific to the person (i.e., age, condition). Other facilitators of physical activity included having accessible (e.g., indoors in winter) and convenient (i.e., time) physical activity options (k = 3) and/or those that involved group physical activity (k = 2).
Discussion
The aim of this review was to systematically map and summarise the available literature on physical activity experiences of community-dwelling older adults with physical disabilities. Our findings make a contribution to the corpus of literature on physical activity in older adults with physical disabilities by synthesising qualitative research on the experiences, outcomes, barriers, and facilitators to physical activity in this population. On the encouraging side, our review demonstrates a wide range of positive outcomes and experiential dimensions across the included studies, as well as a range of facilitators for physical activity. Less encouragingly, however, a range of barriers to physical activity were also reported, as well as negative outcomes and experiences of physical activity. Taken together, we identified intrapersonal-, interpersonal-, environmental-, and systems and programme-level factors that influence physical activity in community-dwelling older adults with physical disabilities. Similar to previous research [Citation60], it is important to note, however, that barriers and facilitators to physical activity were not homogenous to all participants, nor fixed; rather, these were individualized (e.g., transport was a facilitator for some, but a barrier for others) and context-dependent (e.g., weather could be a facilitator at certain times of year, but a barrier at others). Based on our findings, we suggest several potential implications for policy and practice related to promoting physical activity in this population.
First, findings across the included studies demonstrate the need for knowledgeable and supportive healthcare and exercise professionals to facilitate physical activity among older adults with physical disabilities. Healthcare professionals are considered important and credible sources of information about physical activity for disabled people [Citation61,Citation62]. Nevertheless, several studies included in our review highlighted a lack of support for engagement in physical activity among some healthcare professionals as a barrier to physical activity. This reinforces the importance of suitable education and training for healthcare professionals to encourage physical activity in older adults with physical disabilities. As social workers can also act as a key messenger group for physical activity in disabled people [Citation63], educating and training social workers who support older adults with physical disabilities could help to achieve greater impact [Citation64]. In addition, the review emphasises the need for tailored physical activity support for older adults with physical disabilities [Citation18], which can help participants to feel more competent and ameliorate potential negative consequences of physical activity when it is not individually tailored (e.g., lack of pleasure). Furthermore, exercise professionals should be equipped with the appropriate knowledge to ensure they can optimally support physical activity in this population.
Second, our review demonstrates the need to assess and address environmental barriers to physical activity among older adults with physical disabilities. To open up opportunities for older adults with physical disabilities to be more physically active, cross-sectoral collaboration is needed to ensure that environmental planning (e.g., construction of facilities), transport (e.g., access to transport), and fiscal support (e.g., funding for physical activity programmes) is in place. There is a need, therefore, to ensure that agencies, organizations, groups, and individuals responsible for environmental planning and the construction of built environments are educated on how to create inclusive, accessible, and safe environments for physical activity and implement environmental and policy interventions to enable this. One of the most common concerns among older adults was fear of falling, of which physical impairments are a known risk-factor [Citation65]. Built environments should be constructed to reduce fearfulness and increase perceptions of safety among older adults with physical disabilities. Furthermore, the provision of accessible and convenient indoor physical activity opportunities could be valuable during winter, as cold temperatures, poor weather, and darkness were identified as barriers to physical activity. In addition, healthcare professionals and exercise professionals should strive to ensure that participants can feel safe when being physically active, for example, through the provision of appropriate advice on physical activity and ensuring that activities are suitable to each individual’s physical function capabilities. Close monitoring and adaptations to the participants’ needs could also help to build confidence.
Third, our findings underscore the importance of pleasant experiences for promoting physical activity engagement in older adults with physical disabilities. In recent years, there have been calls to embrace approaches that emphasise hedonic dimensions (e.g., pleasure, enjoyment) of physical activity [Citation66–68]. Furthermore, the importance of including hedonic dimensions in physical activity messaging is illustrated in co-produced infographics designed to communicate evidence-based guidelines for physical activity in disabled people in the United Kingdom [Citation69,Citation70] and South Africa [Citation71]. Despite the importance of pleasure and enjoyment, there was consistent cross-study evidence in our review of unpleasant experiential aspects of physical activity, including boredom, lack of fun and enjoyment, and pain and discomfort, with overly-strenuous activities being problematic for some. Pleasure during physical activity (rather than after) is related to long-term engagement in physical activity [Citation72] and pleasure and enjoyment were reported as facilitators of physical activity across multiple studies in our review. Therefore, physical activity programmes should be designed in a way that helps older adults with physical disabilities to maximise pleasure and minimise displeasure during physical activity, as such endeavours are more likely to elicit affective responses that forge associations that encourage future physical activity engagement [Citation66]. Furthermore, efforts to promote physical activity in this population should also embrace hedonic rather than purely biomedical perspectives, ensuring that the pleasures of physical activity are emphasised.
Finally, our review demonstrates the importance of considering how social connections can be harnessed to promote physical activity, as well as other health-related outcomes, in older adults with physical disabilities. Aligned with the “social cure” strand of research on social determinants of health [Citation73], our findings demonstrate that social relationships, social interactions, social support, and feeling a sense of belonging within a group were generally reported as benefits and facilitators of physical activity. Furthermore, the findings demonstrated that strongly identifying with a group (e.g., a physical activity group with people that have similar disabilities) appeared to hold multiple benefits, including that it provided an outlet for social interactions and an opportunity for peer support. In recent years, there is growing interest in the social identity approach to promoting physical activity in groups [Citation74], on the basis that identifying strongly with a group can influence one’s thoughts, feelings, and behaviours (e.g., physical activity), and provide scaffolding to access social-psychological resources from within groups (e.g., social support, sense of belonging) [Citation75]. Group membership in older adulthood is associated with better quality of life [Citation76] and greater physical activity [Citation77]. Furthermore, interventions that build social identities can reduce loneliness [Citation78], a problem that is more common among disabled people [Citation79] and thus more likely to lead to the negative physical and mental health consequences associated with loneliness in older adults [Citation80]. Based on our findings, group-based physical activity programmes should be designed to strengthen positive social identities among older adults with physical disabilities, with the identity leadership approach [Citation55] representing a promising strategy that could be utilised with this population in future. Nevertheless, it should be noted that some participants expressed a preference for engaging in physical activity on their own [Citation46,Citation55]. This emphasises the importance of considering barriers, facilitators, and experiences of physical activity as individualized and contextualized rather than as static and homogenous [see also Citation60].
Future research directions
Based on findings of our scoping review, we highlight several avenues for future research. First, our review demonstrated a general lack of methodological diversity, with studies generally using interviews or focus groups and forms of thematic or content analysis. Although such methods can, and have, been useful in contributing valuable understanding to date, expanding methodological horizons in this area could help to generate more diverse and innovative insights. For instance, researchers could consider the use of drawings [Citation81], go-along interviews [Citation82], photovoice [Citation83], or ethnographic approaches [Citation84]. Second, it was notable that none of the sampled populations were from developing countries. Physical inactivity levels are more prevalent in middle- and low-income countries [Citation85] and estimated levels of physical disability are high (>50%) in low- and middle-income countries [Citation86]. Further research is needed to better understand the physical activity experiences of older adults with physical disabilities in these regions. Third, studies in the review focus mainly on community-based physical activity (e.g., leisure centres, natural environments), but further research is also warranted to examine the feasibility, acceptability, efficacy, and safety of home-based physical activity interventions for older adults with physical disabilities. Furthermore, consideration should also be given to geographical factors (e.g., rural-urban, inland-coastal). Finally, we suggest that new opportunities to advance knowledge will also be opened up by working with older adults with physical disabilities to co-produce research [Citation87].
Review strengths and limitations
The review’s rigour was enhanced by: using established guidance for conducting and reporting scoping reviews; involving two authors in the screening and selection of articles; and sharing our research with individuals with relevant lived experiences prior to submitting for peer review. Despite our efforts to improve rigour, several limitations should be noted. Studies published in the English language were only included. Thus, the review could be susceptible to language bias. Our review only included participants with physical impairments and, therefore, excluded participants with only sensory impairments or intellectual disabilities, for example. Finally, we acknowledge that some relevant participants were excluded due to being in mixed samples with adults aged 18–64, but as data attributable to older adults were not identifiable in those studies, it was not possible to include them.
Conclusions
By systematically mapping and summarising the available qualitative literature on physical activity in community-dwelling older adults with physical disabilities, our scoping review offers an overview of what is known about physical activity in this population based on qualitative evidence. Our findings illustrate that while physical activity is perceived to have wide-ranging benefits for older adults with physical disabilities, a range of barriers to physical activity and negative experiential dimensions and outcomes were reported. Findings demonstrate the need for knowledgeable and supportive healthcare and exercise professionals, environments that support physical activity, and activities that promote pleasure and social connections to enhance the physical activity experiences of older adults with physical disabilities.
Supplemental Material
Download PDF (469 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Martin Ginis KA, van der Ploeg HP, Foster C, et al. Participation of people living with disabilities in physical activity: a global perspective. Lancet. 2021;398(10298):443–455. doi:10.1016/S0140-6736(21)01164-8.
- Williams TL, Smith B, Papathomas A. The barriers, benefits and facilitators of leisure time physical activity among people with spinal cord injury: a meta-synthesis of qualitative findings. Health Psychol Rev. 2014;8(4):404–425. doi:10.1080/17437199.2014.898406.
- Sweet SN, Martin Ginis KA, Tomasone JR. Investigating intermediary variables in the physical activity and quality of life relationship in persons with spinal cord injury. Health Psychol. 2013;32(8):877–885. doi:10.1037/a0032383.
- Hall DL, Allen-Collinson J, Jackman PC. The agenda is to have fun’: Exploring experiences of guided running in visually impaired and guide runners. Qual Res Sport, Exer Health. 2023;15(1):89–103. doi:10.1080/2159676X.2022.2092200.
- Aitchison B, Rushton AB, Martin P, et al. The experiences and perceived health benefits of individuals with a disability participating in sport: a systematic review and narrative synthesis. Disabil Health J. 2022;15(1):101164. doi:10.1016/j.dhjo.2021.101164.
- de Hollander EL, Proper KI. Physical activity levels of adults with various physical disabilities. Prev Med Rep. 2018;10:370–376. doi:10.1016/j.pmedr.2018.04.017.
- Kamil-Rosenberg S, Greaney ML, Hochman T, et al. How do physical activity and health vary among younger, Middle-Aged, and older adults with and without disability? J Aging Phys Act. 2019;27(2):234–241. doi:10.1123/japa.2017-0215.
- Shields N, Synnot AJ, Barr M. Perceived barriers and facilitators to physical activity for children with disability: a systematic review. Br J Sports Med. 2012;46(14):989–997. doi:10.1136/bjsports-2011-090236.
- Martin Ginis KA, Ma JK, Latimer-Cheung AE, et al. A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol Rev. 2016;10(4):478–494. doi:10.1080/17437199.2016.1198240.
- World Health Organisation. World report on disability. 2011. https://www.who.int/disabilities/world_report/2011/report.pdf.
- Department for Work and Pensions. Family Resources Survey: financial year 2020 to 2021. 2022. Available online: https://www.gov.uk/government/statistics/family-resources-survey-financial-year-2020-to-2021.
- United Nations. Ageing and disability. 2023. https://www.un.org/development/desa/disabilities/disability-and-ageing.html.
- World Health Organisation. Disability and health. 2021. https://www.who.int/news7 room/fact-sheets/detail/disability-and-health.
- United Nations. Factsheet on Persons with Disabilities. 2022. https://www.un.org/development/desa/disabilities/resources/factsheet-on-persons-with-disabilities.html.
- Jackson J, Williams TL, McEachern BM, et al. Fostering quality experiences: qualitative perspectives from program members and providers in a community-based exercise program for adults with physical disabilities. Disabil Health J. 2019;12(2):296–301. doi:10.1016/j.dhjo.2018.11.008.
- Martin Ginis KA, Evans MB, Mortenson WB, et al. Broadening the conceptualization of participation of persons with physical disabilities: a configurative review and recommendations. Arch Phys Med Rehabil. 2017;98(2):395–402. doi:10.1016/j.apmr.2016.04.017.
- World Health Organization. The world health report 2001: mental health: new understanding, new hope. Geneva, Switzerland: World Health Organisation; 2001.
- Shirazipour CH, Evans MB, Leo J, et al. Program conditions that foster quality physical activity participation experiences for people with a physical disability: a systematic review. Disabil Rehabil. 2020;42(2):147–155. doi:10.1080/09638288.2018.1494215.
- Ma JK, Martin Ginis KA. A meta-analysis of physical activity interventions in people with physical disabilities: content, characteristics, and effects on behaviour. Psychol Sport Exerc. 2018;37:262–273. doi:10.1016/j.psychsport.2018.01.006.
- Munn Z, Peters MD, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. doi:10.1186/s12874-018-0611-x.
- Williams TL, Ma JK, Martin Ginis KA. Participant experiences and perceptions of physical activity-enhancing interventions for people with physical impairments and mobility limitations: a meta-synthesis of qualitative research evidence. Health Psychol Rev. 2017;11(2):179–196. doi:10.1080/17437199.2017.1299027.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616.
- Daudt HM, van Mossel C, Scott SJ. Enhancing the scoping study methodology: a large, inter-professional team’s experience with arksey and o’Malley’s framework. BMC Med Res Methodol. 2013;13(1):48. doi:10.1186/1471-2288-13-48.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850.
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131.
- Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17(5):427–442. doi:10.1212/wnl.17.5.427.
- Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435–1443. Available from: doi:10.1177/1049732312452938.
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x.
- Smith B, McGannon KR. Developing rigor in qualitative research: problems and opportunities within sport and exercise psychology. Int Rev Sport Exerc Psychol. 2018;11(1):101–121. doi:10.1080/1750984X.2017.1317357.
- Bearne LM, Manning VL, Choy E, et al. Participants’ experiences of an education, self-management and upper extremity eXercise training for people with rheumatoid arthritis programme (EXTRA). Physiother. 2017;103(4):430–438. doi:10.1016/j.physio.2016.12.002.
- Bennett HB, Walter CS, Oholendt CK, et al. Views of in‐person and virtual group exercise before and during the pandemic in people with parkinson disease. Pm R. 2023;15(6):772–779. doi:10.1002/pmrj.12848.
- Bergland A, Fougner M, Lund A, et al. Ageing and exercise: building body capital in old age. Eur Rev Aging Phys Act. 2018;15(1):7. doi:10.1186/s11556-018-0195-9.
- Crowley L, Kennedy N. Barriers to exercise in rheumatoid arthritis – a focus group study. Physiother Pract Res. 2009;30(2):27–33. doi:10.3233/PPR-2009-30207.
- de Groot GCL, Fagerström L. Older adults’ motivating factors and barriers to exercise to prevent falls. Scand J Occup Ther. 2011;18(2):153–160. doi:10.3109/11038128.2010.487113.
- Dohrn IM, Ståhle A, Roaldsen KS. “You have to keep moving, be active”: perceptions and experiences of habitual physical activity in older women with osteoporosis. Phys Ther. 2016;96(3):361–370. doi:10.2522/ptj.20150131.
- Evans N, Connelly DM, Hay ME. The process of commitment to exercise among stroke survivors in Canada. Health Soc Care Community. 2022;30(3):e706–e716.
- Fisken AL, Waters DL, Hing WA, et al. Perceptions towards aqua-based exercise among older adults with osteoarthritis who have discontinued participation in this exercise mode: osteoarthritis, aqua-based exercise. Australas J Ageing. 2016;35(1):12–17. doi:10.1111/ajag.12167.
- Gay C, Eschalier B, Levyckyj C, et al. Motivators for and barriers to physical activity in people with knee osteoarthritis: a qualitative study. Joint Bone Spine. 2018;85(4):481–486. doi:10.1016/j.jbspin.2017.07.007.
- Hammer NM, Bieler T, Beyer N, et al. The impact of self-efficacy on physical activity maintenance in patients with hip osteoarthritis - a mixed methods study. Disabil Rehabil. 2016;38(17):1691–1704. doi:10.3109/09638288.2015.1107642.
- Hendry M, Williams NH, Markland D, et al. Why should we exercise when our knees hurt? A qualitative study of primary care patients with osteoarthritis of the knee. Fam Pract. 2006;23(5):558–567. doi:10.1093/fampra/cml022.
- Hunt ER, Papathomas A. Being physically active through chronic illness: life experiences of people with arthritis. Qual Res Sport Exerc Health. 2020;12(2):242–255. doi:10.1080/2159676X.2019.1601637.
- Jayakaran P, Perry M, Kondov M, et al. Attitudes and beliefs towards physical activity participation in individuals with below-knee amputation. N Z. J Physiother. 2019;47(2):1063–1070.
- Kanavaki AM, Rushton A, Hale E, et al. Physical activity, sedentary behaviour and well-being: experiences of people with knee and hip osteoarthritis. Psychol Health. 2022;:1–19. Advance online publication. doi:10.1080/08870446.2022.2126473.
- Kunkel D, Robison J, Fitton C, et al. It takes two: the influence of dance partners on the perceived enjoyment and benefits during participation in partnered ballroom dance classes for people with parkinson’s. Disabil Rehabil. 2018;40(16):1933–1942. doi:10.1080/09638288.2017.1323029.
- Lange E, Palstam A, Gjertsson I, et al. Aspects of exercise with person-centred guidance influencing the transition to independent exercise: a qualitative interview study among older adults with rheumatoid arthritis. Eur Rev Aging Phys Act. 2019;16(1):4. doi:10.1186/s11556-019-0211-8.
- Larmer P, Kersten K, Dangan J. Patient reported benefits of hydrotherapy for arthritis. N Z. J Physiother. 2014;42(2):89–93.
- Law RJ, Breslin A, Oliver EJ, et al. Perceptions of the effects of exercise on joint health in rheumatoid arthritis patients. Rheumatology (Oxford). 2010;49(12):2444–2451. doi:10.1093/rheumatology/keq299.
- Lee FKI, Lee TFD, So WKW. Effects of a tailor-made exercise program on exercise adherence and health outcomes in patients with knee osteoarthritis: a mixed-methods pilot study. Clin Interv Aging. 2016;11:1391–1402. doi:10.2147/CIA.S111002.
- Lee LS, Hitzig SL, Mayo A, et al. Factors influencing physical activity among individuals with lower limb amputations: a qualitative study. Disabil Rehabil. 2022; 45(9):1461–1470.
- Maiers M, Salsbury SA. “Like peanut butter and jelly”: a qualitative study of chiropractic care and home exercise among older adults with spinal disability. Arthritis Care Res (Hoboken). 2022;74(11):1933–1941. doi:10.1002/acr.24636.
- McKevitt S, Jinks C, Healey EL, et al. The attitudes towards, and beliefs about, physical activity in people with osteoarthritis and comorbidity: a qualitative investigation. Musculoskeletal Care. 2022;20(1):167–179. doi:10.1002/msc.1579.
- Moody J, Hale L, Waters D. Perceptions of a water-based exercise programme to improve physical function and falls risk in older adults with lower extremity osteoarthritis: barriers, motivators and sustainability. N Z. J Physiother. 2012;40(2):64–70.
- O’Brien M, Dodd KJ, Bilney B. A qualitative analysis of a progressive resistance exercise programme for people with parkinson’s disease. Disabil Rehabil. 2008;30(18):1350–1357. doi:10.1080/09638280701614546.
- Petursdottir U, Arnadottir SA, Halldorsdottir S. Facilitators and barriers to exercising among people with osteoarthritis: a phenomenological study. Phys Ther. 2010;90(7):1014–1025. doi:10.2522/ptj.20090217.
- McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspective on health promotion programs. Health Educ Q. 1988; Winter15(4):351–377. doi:10.1177/109019818801500401.
- Stone RC, Baker J. Painful choices: a qualitative exploration of facilitators and barriers to active lifestyles among adults with osteoarthritis. J Appl Gerontol. 2017;36(9):1091–1116. doi:10.1177/0733464815602114.
- Thomas R, Hewlett S, Swales C, et al. Keeping physically active with rheumatoid arthritis: semi-structured interviews to explore patient perspectives, experiences and strategies. Physiother. 2019;105(3):378–384. doi:10.1016/j.physio.2018.09.001.
- Stødle IV, Debesay J, Pajalic Z, et al. The experience of motivation and adherence to group-based exercise of norwegians aged 80 and more: a qualitative study. Arch Public Health. 2019;77(1):26. doi:10.1186/s13690-019-0354-0.
- Monforte J, Smith M, Smith B. Designing a programme to train social workers on how to promote physical activity for disabled people: a delphi study in the UK. Health Soc Care Community. 2022;30(5):e2805–17.
- Faulkner G, Gorczynski P, Arbour KP, et al. Messengers and methods of disseminating health information among individuals with spinal cord injury. In: Berkovsky TC, editor. Handbook of spinal cord injuries. Hauppauge (NY): Nova Science Publishers; 2010. p. 349–374.
- Letts L, Martin Ginis KA, Faulkner G, et al. Preferred methods and messengers for delivering physical activity information to people with spinal cord injury: a focus group study. Rehabil Psychol. 2011;56(2):128–137. doi:10.1037/a0023624.
- Smith B, Wightman L. Promoting physical activity to disabled people: messengers, messages, guidelines and communication formats. Disabil Rehabil. 2021;43(24):3427–3431. doi:10.1080/09638288.2019.1679896.
- Denkinger MD, Lukas A, Nikolaus T, et al. Factors associated with fear of falling and associated activity restriction in community-dwelling older adults: a systematic review. Am J Geriatr Psychiatry. 2015;23(1):72–86. doi:10.1016/j.jagp.2014.03.002.
- Whipple MO, Hamel AV, Talley KMC. Fear of falling among community-dwelling older adults: a scoping review to identify effective evidence-based interventions. Geriatr Nurs. 2018;39(2):170–177. doi:10.1016/j.gerinurse.2017.08.005.
- Brand R, Ekkekakis P. Affective–reflective theory of physical inactivity and exercise: foundations and preliminary evidence. Ger J Exerc Sport Res. 2018;48(1):48–58. doi:10.1007/s12662-017-0477-9.
- Phoenix C, Orr N. Pleasure: a forgotten dimension of physical activity in older age. Soc Sci Med. 2014;115:94–102. doi:10.1016/j.socscimed.2014.06.013.
- Williams DM, B LC. Motivation for exercise: reflective desire versus hedonic dread. In: MH Anshel, SJ Petruzzello, EE Labbé, editors. APA handbook of sport and exercise psychology, vol 2 exercise psychology. American Psychological Association; 2019. p. 363–385.
- Smith B, Kirby N, Skinner B, et al. Infographic. Physical activity for disabled adults. Br J Sports Med. 2019;53(6):335–336. doi:10.1136/bjsports-2018-100158.
- Smith B, Netherway J, Jachyra P, et al. Infographic. Communicate physical activity guidelines for disabled children and disabled young people. Br J Sports Med. 2022;56(10):588–589. doi:10.1136/bjsports-2022-105411.
- Naidoo R, Smith B, Foster C, et al. Physical activity for adults with disabilities: designing a South African infographic to communicate guidelines. Br J Sports Med. 2022;56(10):537–538. doi:10.1136/bjsports-2021-104855.
- Rhodes RE, Kates A. Can the affective response to exercise predict future motives and physical activity behavior? A systematic review of published evidence. Ann Behav Med. 2015;49(5):715–731. doi:10.1007/s12160-015-9704-5.
- Haslam SA, McMahon C, Cruwys T, et al. Social cure, what social cure? The propensity to underestimate the importance of social factors for health. Soc Sci Med. 2018;198:14–21. doi:10.1016/j.socscimed.2017.12.020.
- Haslam SA, Fransen K, Boen F, editors. The new psychology of sport and exercise the new psychology of sport and exercise: the social identity approach. London, England: SAGE Publications; 2020.
- Fransen K, Cruwys T, Haslam C, et al. Leading the way together: a cluster randomised controlled trial of the 5R shared leadership program in older adult walking groups. Int J Behav Nutr Phys Act. 2022;19(1):63. doi:10.1186/s12966-022-01297-x.
- Steffens NK, Jetten J, Haslam C, et al. Multiple social identities enhance health post-retirement because they are a basis for giving social support. Front Psychol. 2016;7:1519. doi:10.3389/fpsyg.2016.01519.
- Stevens M, Lieschke J, Cruwys T, et al. Better together: how group-based physical activity protects against depression. Soc Sci Med. 2021;286(114337):114337. doi:10.1016/j.socscimed.2021.114337.
- Haslam C, Cruwys T, Chang MXL, et al. GROUPS 4 HEALTH reduces loneliness and social anxiety in adults with psychological distress: findings from a randomized controlled trial. J Consult Clin Psychol. 2019;87(9):787–801. doi:10.1037/ccp0000427.
- Emerson E, Fortune N, Llewellyn G, et al. Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: cross-sectional study. Disabil Health J. 2021;14(1):100965. doi:10.1016/j.dhjo.2020.100965.
- Ong AD, Uchino BN, Wethington E. Loneliness and health in older adults: a mini-review and synthesis. Gerontology. 2016;62(4):443–449. doi:10.1159/000441651.
- Guillemin M. Understanding illness: using drawings as a research method. Qual Health Res. 2004;14(2):272–289. doi:10.1177/1049732303260445.
- Carpiano RM. Come take a walk with me: the “go-along” interview as a novel method for studying the implications of place for health and well-being. Health Place. 2009;15(1):263–272. doi:10.1016/j.healthplace.2008.05.003.
- Morgan DL, Ataie J, Carder P, et al. Introducing dyadic interviews as a method for collecting qualitative data. Qual Health Res. 2013;23(9):1276–1284. doi:10.1177/1049732313501889.
- Phillipson L, Hammond A. More than talking: a scoping review of innovative approaches to qualitative research involving people with dementia. Int J Qual Methods. 2018;17(1):160940691878278. doi:10.1177/1609406918782784.
- Guthold R, Stevens GA, Riley LM, et al. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–86–e1086. doi:10.1016/S2214-109X(18)30357-7.
- Salinas-Rodríguez A, Rivera-Almaraz A, Scott A, et al. Severity levels of disability among older adults in low- and Middle-income countries: results from the study on global AGEing and adult health (SAGE). Front Med (Lausanne). 2020;7:562963. doi:10.3389/fmed.2020.562963.
- Smith B, Williams O, Bone L, Collective, T. M. S. W. C. P., et al. Co-production: a resource to guide co-producing research in the sport, exercise, and health sciences. Qual Res Sport Exerc Health. 2023;15(2):159–187., doi:10.1080/2159676X.2022.2052946.