
Abstract
eHealth applications are increasingly being used in services for people with intellectual disabilities (ID). DigiContact is an online support service that uses videoconferencing techniques to enable people with ID to contact a team of specially trained support workers 24/7. In this qualitative and participatory study we aimed to explore the experiences of independently living people with ID with what it is like to be supported online. Five online support users were each interviewed twice and the transcripts were analysed using a phenomenological hermeneutic method. Choice and control played a central role in their shared experiences, as well as the relationship with online support staff. The results indicate that the suitability of online support depends on the needs, capabilities and preferences of each individual support user. This underlines the importance of a personalised approach to the planning and delivery of online support.
In this research we interviewed five persons from the Netherlands about what it is like for them to be supported by the online service DigiContact.
They felt that DigiContact helped them to have access to sufficient professional support. Without DigiContact this would have been impossible, because of a reorganisation of the national long-term care system and cuts in care budgets.
They also felt that DigiContact gave them control over their support and stimulated them to take on an active role towards solving their problems.
Online support felt relatively impersonal, because they had contacts with different support workers.
We conclude that online support seems not to be equally suitable for everybody. Whether online support is suitable, and in what form, depends on someone’s personal needs, wishes and preferences in support. Service organisations should look carefully at each individual person when planning the use of online support.
Points of interest
Introduction
Technology is increasingly being used in the care for and support of people with disabilities. This is also the case within the professional care sector for people with intellectual disabilities (ID), where the generic term eHealth is often used for (health) services and information delivered or enhanced through the Internet and related technologies (Eysenbach Citation2001). Two review studies on the use of eHealth in the field of ID care (Oudshoorn et al. Citation2020; Vázquez et al. Citation2018) have shown that publications in this area focus on initiatives in either therapy and treatment or support for daily functioning. Regarding the latter category, eHealth is mostly used as an instrument to support the learning of specific daily living or vocational skills, and much less as a self-supportive tool or remote professional support (Oudshoorn et al. Citation2020; Vázquez et al. Citation2018). Although this indicates that studies regarding the use of remote support for daily functioning are still relatively scarce, the practice of offering remote online support has been expanding and is expected to continue doing so in the years to come (Friedman and Rizzolo Citation2017; Tassé, Wagner, and Kim Citation2020) .
In remote support, people with ID and their support staff typically use online devices such as (smart)phones, personal computers and tablets to get into contact with each other (Tassé, Wagner, and Kim Citation2020; Taber-Doughty et al. Citation2010). Although the use of remote support is surrounded by several ethical and safety concerns (e.g. Perry and Beyer Citation2012; Niemeijer et al. Citation2010), there are also several reasons that validate its use. For people with ID, a remote (online) delivery of support can have several advantages. First, it can increase the accessibility and flexibility of professional support (Zaagsma et al. Citation2019, Citation2020a). For example, during the current global COVID-19 virus online support could be continued and even scaled-up during periods of ‘lock-down’ and social distancing (EASPPD Citation2020; Zaagsma et al. Citation2020b). Second, remote support may increase the sense of independence, autonomy and privacy as the physical presence of support staff at home decreases (Brewer, Taber-Doughty, and Kubik Citation2010; Tassé, Wagner, and Kim Citation2020; Wennberg and Kjellberg Citation2010). Third, remote support has the potential to be more targeted, focused and specific, as it can be provided when needs arise rather than regardless of immediate needs (Perry, Beyer, and Holm Citation2009).
For service organisations it can also be beneficial to offer (part of their) services remotely, as it may help to increase their sustainability. Not only can technological innovations improve or enrich services, they can also help to differentiate one’s service offer from that of others and to enable a more efficient organisation of services (Brewer, Taber-Doughty, and Kubik Citation2010; Niemeijer et al. Citation2010). These aspects may be extra important for organisations in countries where socio-political shifts have led to social care reforms (e.g. resulting in decreasing care budgets and tightened eligibility criteria) and place the implementation of values like the participation, inclusion and self-direction of people with disabilities under pressure. Such shifts are likely to have various disadvantageous consequences for people with (intellectual) disabilities and their families (Goodley and Lawthom Citation2019; Goodley, Lawthom, and Runswick-Cole Citation2014; Malli et al. Citation2018) and many organisations search for ways to be able to continue their services to the people who need them. Technology, for example in the form of eHealth applications, can be used as a part of this strategy.
All together, these reasons formed the incentive for the Dutch service provider Philadelphia Care Foundation to develop a remote, online support service named DigiContact for people with mild ID (IQ 50–69) or borderline intellectual functioning (IQ 70–85) who live independently in society. DigiContact offers 24/7 online support by using video conferencing techniques to enable communication between support users (people with ID) and a team of about 25 support workers who are especially trained to provide online support. Contact is also possible without video component by regular phone. DigiContact is offered as part of a broader range of services: it is generally combined with onsite support at home or at a community center, courses and/or onsite support regarding work (Vijfhuizen and Volkers Citation2016).
When evaluating a new support service like DigiContact, it is important to include the perspective of the people who use the service, in this case people with ID. A few studies have focused on the expectations, experiences and/or perceptions of people with ID regarding the use of eHealth in support of daily functioning: either in response to the use of eHealth in general (Frielink, Oudshoorn, and Embregts Citation2020) or in the form of remote support (e.g. Tassé, Wagner, and Kim Citation2020; de Wit et al. Citation2015; Zaagsma et al. Citation2019, Citation2020a). These studies give some insights into what people with ID regard as possible advantages and disadvantages of the use of eHealth, and remote support specifically. Perceived advantages were for example more independence and control over one’s life (Frielink, Oudshoorn, and Embregts Citation2020; Tassé, Wagner, and Kim Citation2020), a safe and secure feeling (Tassé, Wagner, and Kim Citation2020; Zaagsma et al. Citation2019, Citation2020a) and an increase in professional support accessibility (de Wit et al. Citation2015; Zaagsma et al. Citation2019, Citation2020a). Privacy concerns (Tassé, Wagner, and Kim Citation2020), the dangers that come with using the Internet (Frielink, Oudshoorn, and Embregts Citation2020), and the risk that eHealth applications will be implemented as a substitute for all onsite support (Frielink, Oudshoorn, and Embregts Citation2020; Zaagsma et al. Citation2020a) were some of the perceived disadvantages. Although these studies are important for understanding more about the potential value of remote, online support for people with ID, they do not provide an account of how online support is perceived by persons who use DigiContact. Knowing more about this is helpful for understanding why some persons have more positive experiences with online support than others. The current study was designed to give an in-depth account of the experiences of a small group of people who use the online support service DigiContact. The aim of this paper is to zoom in on the experiences of individuals and to describe in detail how they experience online support and give meaning to their experiences.
Method
This study used a qualitative research design, in which interviews with DigiContact support users were conducted and transcripts were analysed using a phenomenological hermeneutic method described by Lindseth and Norberg (Citation2004). Strongly inspired by the phenomenological hermeneutical interpretation theory developed by Ricoeur (Citation1976), this method aims to obtain knowledge of the essential meaning of lived experiences (Lindseth and Norberg Citation2004). The study was carried out by a duo of researchers and relied on a participatory research strategy in which an academically trained researcher (first author) and a co-researcher with ID (third author) worked together. The co-researcher was actively involved in identifying and clarifying the research topic, recruiting participants, data collection (construction of interview guide, planning and conducting interviews) and data analysis. Four senior researchers (second, fourth, fifth and sixth author) fulfilled advisory and coaching roles, mainly regarding qualitative and inclusive research methodology.
Participants
Participants were selected using a purposive sampling strategy (Patton Citation2005). We aimed to include individuals who used online support as their main form of professional support as this would guarantee the use of a sample with sufficient experience with online support. From the entire DigiContact case load, a senior support professional working for DigiContact was able to locate ten online support users for whom the service was either the only or the main source (as in: most intensively used) of professional support during at least the previous six months (December 2017 – May 2018). These ten support users were contacted through their case workers (senior support professionals who coordinate services), who were employed by the service organization that also offers DigiContact. Five of them did not want to participate in this study, for which they expressed different reasons: two felt uncomfortable about being interviewed, two had recently participated in an (unrelated) interview study and did not want to be interviewed again, and one opted out for reasons unknown. Five support users did agree to participate. In the following paragraphs, they are introduced through a short description of personal and professional support characteristics. Pseudonyms are used to protect participant anonymity.
Chris (35) lives alone in a semi-rural area and has a part-time job. He is single. He has a mild ID (IQ range 50–69) and has been receiving professional ID services for 21 years. Five years ago Chris started to use DigiContact. Recently, he put a hold to all professional support services except for DigiContact. Chris uses a tablet to contact the service on average twice a week (video connection).
Dave (46) lives alone in a semi-urban area and has a full-time job. He is single. Dave’s IQ level is unknown. He was registered for professional support about one year ago, after his long term relationship broke up. He was found eligible for online support from DigiContact only. Dave uses his landline phone to contact the service once a week (audio connection).
Carol (71) lives alone in an urban area and doesn’t have a job or any other fixed day-time occupation. She is divorced. Carol’s IQ level is unknown. She started receiving professional ID services four years ago, after she was diagnosed with cancer and underwent several surgical procedures. Since then Carol is supported at home by two different onsite support workers. Since two years, she also uses DigiContact support. She uses a tablet or mobile phone to contact the service about three times a day (audio or video connection).
Michael (56) lives alone in a semi-rural area and has a full-time job. He is a widower. Michael has borderline intellectual functioning (IQ range 70–85), and has been receiving professional ID services for 36 years. Currently, he is supported by an onsite support worker with whom he meets regularly at a community center. Five years ago Michael started using DigiContact support. He uses his tablet or mobile phone to contact the service about two or three times a week (audio or video connection).
Ben (39) lives alone in a semi-rural area and has a full-time job. He is single. Ben has borderline intellectual functioning and has been diagnosed as having ‘autism’. He has been receiving professional ID services for 25 years. Ben is supported by an onsite support worker with whom he meets at a community center. Five years ago, he also started using DigiContact support. He uses his tablet or mobile phone to contact the service about three times a week (audio or video connection).
Data collection and procedure
We used semi-structured interviews to collect data. An interview guide was developed, which included five main topic areas: (a) general information on the participants’ lives (to get to know each other); (b) use of support (an exploration of the availability and use of professional and natural supports); (c) the context and history of online support use (when, why and how DigiContact was introduced to them); (d) the experiences with online support in relation to support needs (views on if and how online support meets their needs); (e) evaluation of online support (how participants feel about being online supported). Each main topic started with an open-ended question, after which follow-up questions were based on the participant’s responses. Each participant was interviewed twice because including all main topics in one interview would be too much of a burden for the participants. This also allowed for more time to obtain the participants’ trust and increase the likelihood of them feeling at ease and expressing themselves freely. The first interview focused on topic areas a, b and c. The second interview focused on topic areas d and e.
The interviews were conducted by the two researchers together (first and third author). As the co-researcher did not have prior experience with interviewing, he received training in interview techniques before and during data collection. While the co-researcher observed and made field notes during the first few interviews, his role shifted over time towards him taking more and more the lead in asking questions. Participants were interviewed at home, during a four-month period (June – September 2018) and lasted between 42 and 67 min. The time between the two interviews varied from six to thirteen weeks. All interviews were audio-recorded with participant approval and transcribed verbatim. We included member validation as a validity check method (Green and Thorgood Citation2014): all participants received a typed summary of their interviews in accessible language to check for accuracy. They all felt that the summary represented their experiences well and no adjustments were made.
Data analysis
Analysis of the transcripts was based on the guidelines described by Lindseth and Norberg (Citation2004) and followed three steps: (1) the formulation of a naïve understanding; (2) structural analysis; and (3) the formulation of a comprehensive understanding. Throughout each step, the first author and co-researcher worked together and discussed their methods and findings by peer debriefing with two senior researchers (second and sixth author).
The first step started with listening to the interview recordings and reading all transcripts multiple times (first author only) to get an overall picture of the data and to grasp its meaning as a whole. The two researchers then came together to discuss and compare their first impressions and interpretations. Together they formulated a naïve understanding, which is a preliminary interpretation of the meaning of the data in its entirety. We attempted to interrelate the accounts of the participants, by undertaking a process of going back and forth between the transcripts and our interpretation. The naïve understanding was presented to and discussed with one participant, one online support worker and one onsite case worker. They all agreed with the naïve understanding and no adjustments were made.
The second step consisted of thematic structural analysis and was intended to validate the naïve understanding. Connections and patterns in the data were uncovered by dividing the data into meaning units, which are pieces of text (of any length) that convey one meaning. Each meaning unit was then condensed and expressed as concisely as possible in everyday words. The two researchers did this independently from each other and then again compared and discussed their meaning units and condensations until consensus was reached. Next, we reflected together on the condensed meaning units and, where relevant, abstracted them into subthemes and assembled them further into themes. To facilitate this process, we copied each meaning unit and its condensation on to a piece of paper, so we could (re)position them while assembling similar condensations.
The third step consisted of identifying relationships between themes and interpreting the findings in relation to the research question and the study context. The first author read all transcripts again, while taking into consideration the research question, the naïve understanding and the results of the structural analysis. Through thorough discussions, both with the co-researcher as well as with the senior researchers, a comprehensive understanding of the findings was formed and formulated. The comprehensive understanding was checked for its recognisability and relevance by four participants, as well as one online support worker and one onsite case worker. Although they all felt that the comprehensive understanding represented their feelings and experiences well, they also made some remarks that were used to add nuance to the comprehensive understanding.
Ethical procedure
The Medical Ethics Review Committee of VU University Medical Center (FWA00017598) confirmed that official approval was not required as the Dutch Medical Research Involving Human Subjects Act (WMO) did not apply. We followed the Disability Studies in the Netherlands Code of Practice in Research (DSIN Citation2017). Written informed consent was obtained from all participants. Audio-recordings were made after the participants gave their approval and the audio files were destroyed after analysis had been completed. All data were anonymized and subsequently handled and stored with care and respect for privacy.
Findings
Naïve understanding
The participants’ accounts showed that having 24/7 access to online support was perceived to be valuable, but that there were also some negative evaluations. Being able to initiate and control their online support contacts (timing them whenever and as often as needed) appeared to enhance the experience of self-direction in support. Online support seemed to have a positive impact on emotional well-being, as its continuous availability gave participants a secure feeling and the opportunity to clear their mind from frustrations and worries immediately. Also, DigiContact was seen as an additional social contact and alleviated feelings of isolation and loneliness. At the same time, participants needed time to get used to online support because it was felt to be different from regular onsite support. Participants struggled with not having an assigned online professional to talk to, which made the support feel less personal. It seemed that their use of online support was not only influenced by their own experiences and expectations, but also by their case worker and informal caregivers, who often stimulated participants to use online support.
Structural analysis
The structural analysis resulted in three themes that reflected the meaning of being supported online: (1) Using online support as a solution; (2) Helping oneself through being in control; and (3) Being in a relationship with a service, not a person. In the following sections the three themes are described and illustrated with quotes from the interviews.
Using online support as a solution
A common experience identified through the analysis consisted of using online support to create a better match between available professional supports on the one hand and support needs and/or preferences on the other hand. Getting the needed or wanted professional support was perceived to be an ongoing struggle. For some participants this was about having access to professional support, for others it concerned getting enough support and/or preferring a different type of support.
For most participants online support was a way to ensure themselves of (sufficient) professional support within a context of care reforms, austerity measures and strict support eligibility. Participants who had been receiving services for quite some years had experienced the impact of the long-term health care reforms. Their recollections indicate that this had been a stressful period during which they became aware of their vulnerability because of the uncertainty as to whether and how professional support would be continued. As DigiContact was introduced during that period, the participants linked its introduction to the reformations, reinforcing their perception that this new service was (at least partially) there to replace onsite support. Although negative feelings and opposition prevailed at first, participants soon realized that the service offered them the possibility to maintain more or less the same intensity of support they were used to:
Instead of every week you get it [onsite support at home] just once a month or once every three months. If you want more you have to call DigiContact when something is bothering you. In fact, I get just as much support. It still is three times a week. But now I call DigiContact twice a week and once a week I go to the meeting place. (Ben)
Of course, I can phone A or C [onsite support workers], but they cannot always come to me, because they are busy themselves. That is why I am so happy with them [DigiContact]. And I keep repeating it: when I need them, I call them and they will make time for me. I can’t do that with A and C, when they are not there.
Unlike the others, Chris did not use online support to ensure himself of sufficient professional support. Instead, he felt that online support matched his personal support preferences better than onsite support. After a long history of receiving professional services, he had been unhappy with his onsite support. When DigiContact was introduced, he immediately felt that this would improve services for him. For him, being in control of the timing and frequency of his support contacts was a big advantage (see also theme ‘Helping oneself through being in control’). As support workers no longer entered his home, he felt that online support workers respected his privacy more and interfered less with his business:
When it comes to support, the real life support I had, they played mother knows best to me. They did not give me much room to learn or to discover. […] I say that [DigiContact] means progress. I knew it right away, to me it is the invention of the century.
Helping oneself through being in control
The continuous availability of online support combined with being able to decide when contact was needed, played a central role in the participants’ experiences. Deciding when and how often support was needed, seemed to contribute to a sense of control and ownership over their support. Participants could time their contacts according to their need(s) as well as convenience. This contrasted with their onsite support experiences, where they generally felt to have a limited say in when and how often they had access to their onsite support worker:
Yes, they [his two onsite support workers] just did not want to adjust their agendas. Their appointments were fixed and when I wanted to make an appointment, it was not possible. […] They are difficult. Difficult. Well, now you no longer are dependent on them. You don’t even need to be at home or make an appointment when you need support. It is when I want and when it’s a good time for me and when I feel like it. (Chris)
I use DigiContact as an outlet, so to speak. When I have had a terrible day or when I don’t feel well in my head. Or when something is bothering me, I think about things a lot. Then I [with an emphasis on ‘I’] can call them to clear my head. (Chris)
They can see that too often I keep worrying about certain issues. They tell me I should call them. They want me to take the initiative to call and get rid of my frustrations. I didn’t do that at first, but I do now more and more often. I think this is something I have to learn. (Michael)
Yes, I mean, then I don’t have an appointment, so I can’t just… At least, that is what I think at such moments. That I can’t just say like well, I will call them now. However, they say I can, so maybe… Unless something extreme happens, that is different, but normally…no. (Dave)
They told me I can always call them whenever something is worrying me or when my head is spinning. Then I can call them every day, but also every evening and every night. That makes me feel relaxed, like yes, yes, yes, because I can get things off my chest, even when I lay tossing and turning in my bed. (Ben)
Look, it is possible that if there is a problem, your support worker [onsite] will come two or three days later. But now, you can just call and tell them like ‘Hey, I got a problem’ and get rid of it immediately. (Chris)
Being in a support relationship with a service, not a person
Another distinctive feature of the online support service that played an important role in the participants’ experiences, was the fact that support users do not have contacts with a fixed online support worker. After all, when someone contacts DigiContact, he or she talks to the support worker who happens to be on duty at that particular moment. This had consequences for the way participants experienced their relationship with the online support staff. The support contacts were perceived to be relatively impersonal as both parties did not know each other (well).
There were two sides to the experience of not knowing each other. One side was about the support user not knowing the online support staff, which resulted in some participants not feeling confident and secure enough to open up: ‘DigiContact is certainly helpful, but sometimes I find it difficult to explain certain things. I, for me, I do not find it very direct’ (Michael). A feeling of trust and security did improve over time, as participants got to know the online support workers a little better and as a result felt more at ease about confiding in them. A certain level of reciprocity in exchanging personal information was felt to be helpful, as were annual meet-and-greet sessions where participants could meet staff members in person. Nonetheless, for some participants a situation was created over time in which some of the online support workers were trusted and others not: ‘Because you build up a bit of trust with the person you are talking to, and well, with the person you get the next time, you don’t know what it will be like’ (Dave). In addition to the difficulty of knowing and trusting an entire team of support workers, the experience of feeling a connection with a support worker was important. Participants described that they felt more at ease with some support workers than with others and this could endanger getting good support: ‘There are at least two [online support workers] I don’t have a connection with. […] To get the right kind of help, you’ve got to have a connection. If that is missing, it doesn’t feel right to me’ (Ben).
The other side of the experience of not knowing each other, was that participants sometimes felt that online support workers did not know them well enough. This could be annoying because they had to introduce themselves and share their story repeatedly. Some participants stressed that not being known well, entailed the risk that support was not tailored to their personal needs. Ben talked about how this used to be a problem for him, but that over time the staff has gotten to know him well enough:
It does not bother me any longer that I talk to someone else every time, as everybody knows me by now. They all know what’s bothering me, so they all know about my autism and that I followed an assertiveness training.
Comprehensive understanding
The structural analysis validated the naïve understanding to a large extent but at the same time clarified some aspects, such as how the participants saw their online support experiences as embedded within the context of their broader, individual lives and circumstances. First, care reforms and accompanying changes in (the availability of) services reinforced a situation in which participants were searching for ways to get the support they needed and wanted. DigiContact was seen and used as a way to shape professional supports towards better alignment with their needs and preferences. Second, the participants were often stimulated by their case worker and close relatives to use online support. Third, the participants’ support history also played an important role, as their experiences with onsite support served as a benchmark for interpreting online support experiences. This comparison resulted in online support being experienced as a very different way to be supported.
This perception of online support as a different way of being supported was grounded in the experiences with four unique online support characteristics: (1) the 24/7 availability; (2) support users can initiate contact; (3) support is provided by a team of support workers; and (4) the online support staff are stationed in one location. These characteristics had certain implications for the way support contacts were realized as well as for the nature of the relationship with support staff. The 24/7 availability and being able to initiate contact not only meant that participants had continuous and immediate access to professional support, but also that they could determine the timing and frequency of their support. The fact that online support was provided by a team of support workers situated at one location implied that participants were not supported by a fixed support worker and that support was delivered from a distance. is a visual representation of how the four online support characteristics and their implications relate to the participants’ experiences and the meanings given to the experiences.
Figure 1. Visual representation of how DigiContact characteristics (inner circle) and their implications (middle circle) relate to user experiences (outer circle).
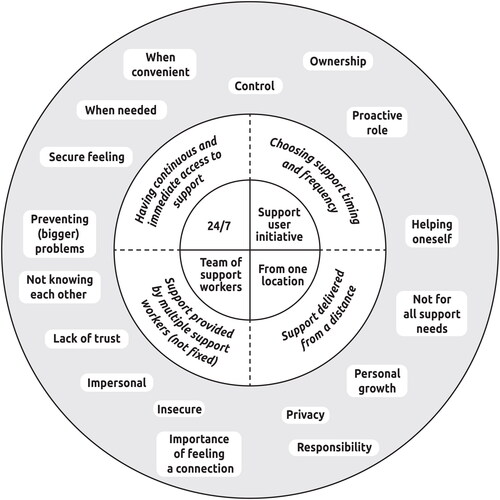
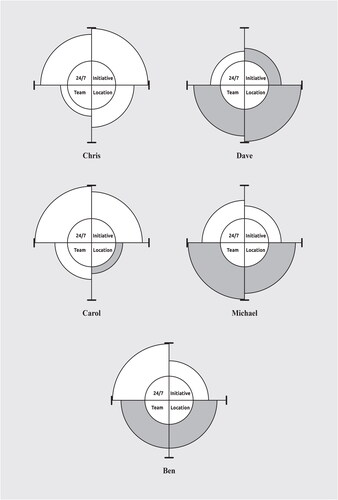
How the participants experienced and used online support seemed to be influenced by how they personally felt about the four online support characteristics and their implications: whether they valued them positively or negatively and the relative importance of these implications for them. Since this evaluation was based on internal values and personal contexts, this differed between participants. illustrates this by presenting the experiences of the participants in profiles. Online support seemed better aligned (more white than grey) with the preferences and needs of participants who found it relatively important to be able to choose and decide themselves when and how often support contacts were needed and/or to be able to seek support always without having to postpone contact (Chris and Carol). These participants employed online support as a way to get the type of support needed or preferred. At the same time, online support was less aligned (more grey than white) with the preferences and needs of participants for whom building a relationship with a fixed professional was a prerequisite for feeling safe enough to discuss problems and/or who found it important to have someone present to help with questions and problems (Dave and Michael). These participants merely used online support as a way to get (enough) support.
Figure 2. Participant profiles of the experiences with DigiContact. Each profile consists of four sectors that represent the participant’s experiences with the four unique online support characteristics and their implications. The colour of a sector represents whether a characteristic and its implications are experienced as predominantly positive (white) or negative (grey). The size of a sector represents the importance of the characteristic and its implications: the bigger the sector, the more important.
For each participant, the interplay between characteristics, their implications and experiences and attached meanings is a dynamic process which may shift over time and from one situation (or problem) to the next. For example, after a while a person can get used to certain online support characteristics and value them differently. Also, someone may prefer to contact the online support service for certain issues or questions and not for others (for example only when postponing is not desirable). People with access to both online and onsite services can make their own decisions regarding whom they seek contact with for what kind of support.
Discussion
This study provides insight into the lived experiences of five independently living people with ID with the nature and meaning of being supported by the remote, online support service DigiContact. The participants’ experiences demonstrated many facets which are dynamic as they move and change through time, situations and contexts. When seeking to understand what it is like to be supported online, it is therefore crucial to be sensitive to the contexts and lives of individual support users. The findings show that the participants varied in how they experienced the different aspects of being online supported. Nevertheless, there were also shared experiences that make up the essence of what it meant for them to be online supported. The main findings of this study are discussed using two key aspects within the participants’ experiences: (a) choice and control, and (b) interactions with support staff.
Choice and control
Being able to choose and control one’s support played a central role in the participants’ experiences with online support at two different levels of the support process: the planning of services (meso) and the day-to-day delivery of support (micro). Regarding the planning of services, participants generally felt that their level of control over their use of online support was limited as there were not always suitable and adequate alternative services to choose from. An advantage of having access to DigiContact was that this (at least) provided them with an (extra) source of support. Which services were available and in what intensity, was felt to be determined by local authorities in charge of assessing eligibility and the provider organization’s services portfolio. The national care reforms in the Netherlands and the consequences of related austerity measures for (the availability of) services made it difficult for some participants to get the support they needed and wanted. This corresponds to a recent review study on the effects of global austerity measures (Malli et al. Citation2018). This study concluded that cuts in (the funding of) disability services had led to poor alignment with care needs which in turn seemed to negatively affect the well-being of people with ID. Besides having few service options, we also found that family members and case workers had a strong influence on the participants’ decision to get connected to and use DigiContact. Especially case workers were highly influential as they were the ones who introduced the service to the participants, advised them to use it and arranged for its installation. Such (inter)dependency on other people in the planning of services was also described by others (e.g. Smith Citation2013; Williams and Porter Citation2017).
In contrast with the process of service planning, participants were able to choose and control their day-to-day use of online support. Being the one to initiate contact was generally seen as a positive aspect of online support, as the participants could decide for themselves if, when and how often they needed support. This enabled them to shape their contacts according to their needs and wishes, an advantage of eHealth that was also found by Frielink, Oudshoorn, and Embregts (Citation2020). It also seemed to have an empowering impact on some participants as they became aware of their own active role in solving their problems. Moreover, having continuous (24/7) and immediate access to online support meant that support could be mobilized without having to postpone contact, which not only gave some participants a secure feeling, but also made it possible to prevent problems and concerns from lingering on or increasing. This was also found in two previous studies on DigiContact (Zaagsma et al. Citation2019; Citation2020a). The current study shows that besides having several advantages, being the one to initiate support contacts can have a downside as having to decide when support is needed, maybe (too) stressful or too difficult for some.
Interactions with support staff
The interactions between DigiContact support staff and participants were characterized by the physical distance between both parties and the fact that participants did not have contacts with a fixed support staff member. The experiences of the participants show that although these characteristics can have an certain advantage, there can also be serious drawbacks. On the positive side, some participants felt that the physical distance between themselves and the online support staff stimulated an active role towards solving issues. By providing support from a distance, online staff were less likely to take over and instead adopted a ‘hands-on-the-back’ coaching style that facilitated personal growth in developing problem-solving skills and self-confidence. This is an interesting finding in the light of studies stressing that in their work, support staff often experience a conflict between having a duty to care, manage risks and protect on the one hand and having a duty to recognize and promote autonomy on the other hand (Hawkins, Redley, and Holland Citation2011). By providing support from a distance the focus seems to shift towards promoting the autonomy of support users. Online support staff helped participants to make choices and steer their life according to their own wishes, without there being a need for them to be completely self-reliant or independent. This corresponds with the idea of relational autonomy, meaning that people are (in varying degrees) interdependent on others in order to exert control and agency in one’s life (Dowling et al. Citation2019; Morris Citation2004; Perkins et al. Citation2012). Having an active role regarding initiating and designing their own support contacts as well as in solving their problems also resonates with the concept of self-management, as van de Velde et al. (Citation2019) found that actively participating in and taking responsibility for the care process are important attributes of self-management.
On the negative side, some participants felt that online support staff were limited in what they could do for them, because they were not physically present in the same room which made it impossible to carry out certain tasks together. This corresponds with a previous study in which we found that individual support users used DigiContact support mostly for mental health related issues and as an extra social contact (i.e. someone to see and talk to), and not so much for practical issues (Zaagsma et al. Citation2020a). In addition, some participants expressed the worry that online support staff are limited in what they can see and pick up on. Although beneficial for experiencing privacy, these participants also felt that this asks for a certain competence and responsibility of support users: being able and willing to signal potential problems timely and to be open about them.
Besides the physical distance between support staff and support users, to be supported online by DigiContact means having contacts with different support workers and not having a choice regarding whom one speaks to. At the time of writing this paper, the online support team consisted of 25 support workers. As a consequence, participants and online support workers did not know each other (well), which made their contacts feel relatively impersonal. According to the participants, this brings the risks of support users not feeling confident and secure enough to open up and discuss certain issues, and of support staff not knowing individual support users well enough to know how to optimally support them. Various studies have stressed the importance and value of creating trusting and caring relationships between people with ID and support staff (Clarkson et al. Citation2009; Giesbers et al. Citation2019; Pallisera et al. Citation2018; Petner-Arrey and Copeland Citation2014). Time, staff continuity and feeling ‘the right chemistry’ between both parties seem to be conditional for creating an optimal support relationship (Giesbers et al. Citation2019; Roeden, Maaskant, and Curfs Citation2011). In this respect, one might wonder whether a service like DigiContact is able to meet all support needs and be a suitable alternative for everyone to (onsite) support by a fixed support worker.
Strengths and limitations of this study
The greatest strengths of this study lie in the appropriateness of our design and methods as well as in the rigour we adopted in our procedures. The phenomenological hermeneutic method we used for analysing our data (Lindseth and Norberg Citation2004) enabled us to get an in-depth account into the complexity of the experiences of people who use the online support service DigiContact as their main form of professional support. The techniques of prolonged engagement, peer debriefing and member checking have been used to assess and enhance the credibility and confirmability of our findings (Frambach, der Vleuten, and Durning Citation2013; Green and Thorgood Citation2014). Our participative strategy, in which a co-researcher with ID and an academically trained researcher worked together throughout all phases of this study, proved to be very valuable as it helped us to formulate interview questions more accessibly, to gain the trust of participants during interviews and to incorporate a broader view by interpreting the transcripts together.
The use of a small sample can be regarded as both a strength and a limitation of this study. While it allowed for a more in-depth engagement with each individual participant, it also strongly limits the generalizability of our findings. Besides small, our sample was in some respects specific. All participants were 35 years or older and used online support as their main form of professional support. Moreover, three participants had been receiving onsite ID services for more than 20 years. It is likely that these characteristics influenced the participants’ experiences with online support in such a way that others, for example young people or people new in ID services, might not recognize them. In future studies we would look for larger samples to include and compare the experiences of a broader group of online support users, including young people (18–25 years), people who use online support as a relatively small part of their professional supports and people who are new to the ID service delivery system. The findings of this current study provide valuable input on aspects regarding support user experiences and evaluation that can be included in such studies.
Implications for practice
The limited generalizability of this study’s findings does not affect its capacity to illustrate the complexity and nuance that are important within the discourse on the role and value of eHealth and remote support within the care for people with ID. The findings show that the suitability of online support seems to depend on the preferences, needs and capabilities of individual support users. For example, online support seems to be more suitable for persons who highly value being able to decide when and how often they need support than for persons for whom having a trusted relationship with a professional is a prerequisite for feeling secure enough to discuss concerns or issues. Such aspects are likely to make the difference between whether DigiContact can function as a full, all-round service able to stand on its own, or rather as an addition to support from a fixed onsite support worker.
As online support does not seem to suit every person equally well and in the same way, it is important that service organisations adopt a personalised approach to its planning and delivery. Not only should this approach be aimed at determining the suitability of online support for individual support users, it is also important to look at how the support itself can be adapted to match someone’s needs and preferences, for example with respect to contacts with or without video connection. As a person’s experiences with online support can change over time (for example due to changes in circumstances), a personalised approach remains important for as long as a person uses online support. Therefore, it is recommendable for service organisations to invest in an ongoing dialogue with each support user on his or her online support experiences. A personalised approach to online support corresponds with what various authors from the research field of disability studies and the use of assistive technology have stressed, namely the importance of matching technologies with the needs, preferences and expectations of individual persons and their environments (e.g. Federici, Scherer, and Borsci Citation2014; Krantz Citation2012; Leopold et al. Citation2015; Scherer and Federici Citation2015).
In contexts characterized by social care reforms, the use of remote, online support is often seen as a cost-saving measure from which organisations benefit more when its implementation concerns larger groups of support users. This study shows that although some people with ID experience online support as a valuable addition to (Carol) or worthy alternative for (Chris) onsite support, others consider it to be not useful for them (Dave). Such differences between people underline that online support cannot be regarded nor implemented as a generic solution to social and political challenges.
Conclusion
Exploring the experiences of support users is indispensable when evaluating new eHealth initiatives for people with ID, as it provides useful insights into the complexity of individual support arrangements. This study suggests that 24/7 online support can have both benefits and drawbacks for people with ID and that its suitability depends on the needs, preferences and capabilities of individual support users. Therefore, the online support service DigiContact is not a ‘one service fits all’ solution, which underlines the importance of a personalised approach to its planning and delivery.
Disclsoure statement
The authors declare that no restrictions were imposed during any phase of this study nor on the publication of the research data. This study was conducted as part of the dissertation research project of the first author.
Acknowledgements
We would like to thank the people who took part in this study for sharing their experiences and feelings with us. Our gratitude also goes out to those who helped us with sample selection, recruitment and member checks.
Additional information
Funding
References
- Brewer, J. L., T. Taber-Doughty, and S. Kubik. 2010. “Safety Assessment of a Home-Based Telecare System for Adults with Developmental Disabilities in Indiana: A Multi-Stakeholder Perspective.” Journal of Telemedicine and Telecare 16 (5): 265–269. doi:10.1258/jtt.2010.090902.
- Clarkson, R., G. H. Murphy, J. B. Coldwell, and D. L. Dawson. 2009. “What Characteristics Do Service Users with Intellectual Disability Value in Direct Support Staff within Residential Forensic Services?” Journal of Intellectual & Developmental Disability 34 (4): 283–289. doi:10.3109/13668250903285630.
- Dowling, S., V. Williams, J. Webb, M. Gall, and D. Worrall. 2019. “Managing Relational Autonomy in Interactions: People with Intellectual Disabilities.” Journal of Applied Research in Intellectual Disabilities: JARID 32 (5): 1058–1066. doi:10.1111/jar.12595.
- DSIN. 2017. “Code of Practice for Researchers 2016–2017.” Accessed 10 April 2018. https://disabilitystudies.nl/sites/disabilitystudies.nl/files/dsin_code_of_practice_for_research_complete.pdf
- EASPPD. 2020. “The COVID-19 Outbreak and Support Service Providers for Persons with Disabilities.” Accessed 6 June 2020. https://www.easpd.eu/en/content/covid-19-outbreak-andsupport-service-providers-persons-disabilities.
- Eysenbach, G. 2001. “What is E-Health?” Journal of Medical Internet Research 3 (2): e20. doi:10.2196/jmir.3.2.e20.
- Federici, S., M. J. Scherer, and S. Borsci. 2014. “An Ideal Model of an Assistive Technology Assessment and Delivery Process.” Technology and Disability 26 (1): 27–38. doi:10.3233/TAD-140402.
- Frambach, J. M., C. P. der Vleuten, and S. J. Durning. 2013. “AM Last Page. Quality Criteria in Qualitative and Quantitative Research.” Academic Medicine: Journal of the Association of American Medical Colleges 88 (4): 552. doi:10.1097/ACM.0b013e31828abf7f.
- Friedman, C., and M. C. Rizzolo. 2017. “Electronic Video Monitoring in Medicaid Home and Community-Based Services Waivers for People with Intellectual and Developmental Disabilities.” Journal of Policy and Practice in Intellectual Disabilities 14 (4): 279–284. doi:10.1111/jppi.12222.
- Frielink, N., C. E. Oudshoorn, and P. J. C. M. Embregts. 2020. “eHealth in Support for Daily Functioning of People with Intellectual Disability: Views of Service Users, Relatives, and Professionals on Both Its Advantages and Disadvantages and Its Facilitating and Impeding Factors.” Journal of Intellectual & Developmental Disability. 46 (2): 115–125. doi:10.3109/13668250.2020.1744878.
- Giesbers, S. A. H., L. Hendriks, A. Jahoda, R. P. Hastings, and P. J. C. M. Embregts. 2019. “Living with Support: Experiences of People with Mild Intellectual Disability.” Journal of Applied Research in Intellectual Disabilities: JARID 32 (2): 446–456. doi:10.1111/jar.12542.
- Goodley, D., and R. Lawthom. 2019. “Critical Disability Studies, Brexit and Trump: A Time of Neoliberal–Ableism.” Rethinking History 23 (2): 233–251. doi:10.1080/13642529.2019.1607476.
- Goodley, D., R. Lawthom, and K. Runswick-Cole. 2014. “Dis/Ability and Austerity: Beyond Work and Slow Death.” Disability & Society 29 (6): 980–984. doi:10.1080/09687599.2014.920125.
- Green, J., and N. Thorgood. 2014. Qualitative Methods for Health Research. 3rd ed.London: Sage.
- Hawkins, R., M. Redley, and A. J. Holland. 2011. “Duty of Care and Autonomy: How Support Workers Managed the Tension between Protecting Service Users from Risk and Promoting Their Independence in a Specialist Group Home.” Journal of Intellectual Disability Research: JIDR 55 (9): 873–884. doi:10.1111/j.1365-2788.2011.01445.x.
- Krantz, O. 2012. “Assistive Devices Utilisation in Activities of Everyday Life-A Proposed Framework of Understanding a User Perspective.” Disability and Rehabilitation. Assistive Technology 7 (3): 189–198. doi:10.3109/17483107.2011.618212.
- Leopold, A., A. Lourie, H. Petras, and E. Elias. 2015. “The Use of Assistive Technology for Cognition to Support the Performance of Daily Activities for Individuals with Cognitive Disabilities Due to Traumatic Brain Injury: The Current State of the research.” NeuroRehabilitation 37 (3): 359–378. doi:10.3233/NRE-151267.
- Lindseth, A., and A. Norberg. 2004. “A Phenomenological Hermeneutical Method for Researching Lived Experience.” Scandinavian Journal of Caring Sciences 18 (2): 145–153. doi:10.1111/j.1471-6712.2004.00258.x.
- Malli, M. A., L. Sams, R. Forrester-Jones, G. Murphy, and M. Henwood. 2018. “Austerity and the Lives of People with Learning Disabilities. A Thematic Synthesis of Current Literature.” Disability & Society 33 (9): 1412–1435. doi:10.1080/09687599.2018.1497950.
- Morris, J. 2004. “Independent Living and Community Care: A Disempowering Framework.” Disability & Society 19 (5): 427–442. doi:10.1080/0968759042000235280.
- Niemeijer, A. R., B. J. M. Frederiks, I. I. Riphagen, J. Legemaate, J. A. Eefsting, and C. M. P. M. Hertogh. 2010. “Ethical and Practical Concerns of Surveillance Technologies in Residential Care for People with Dementia or Intellectual Disabilities: An Overview of the Literature.” International Psychogeriatrics 22 (7): 1129–1142. doi:10.1017/S1041610210000037.
- Oudshoorn, C. E. M., N. Frielink, S. L. P. Nijs, and P. J. C. M. Embregts. 2020. “eHealth in the People with Mild Intellectual Disability in Daily Life: A Systematic Review.” Journal of Applied Research in Intellectual Disabilities: JARID 33 (6): 1166–1187. doi:10.1111/jar.12758.
- Pallisera, M., M. Vilà, J. Fullana, G. Díaz-Garolera, C. Puyalto, and M.-J. Valls. 2018. “The Role of Professionals in Promoting Independent Living: Perspectives of Self-Advocates and Front-Line Managers.” Journal of Applied Research in Intellectual Disabilities: JARID 31 (6): 1103–1112. doi:10.1111/jar.12470.
- Patton, M. Q. 2005. Qualitative Research. Encyclopedia of Statistics in Behavioral Science. Saint Paul, MN: John Wiley & Sons, Ltd; Union Institute and University.
- Perkins, M., M. Ball, F. Whittington, and C. Hollingsworth. 2012. “Relational Autonomy in Assisted Living: A Focus on Diverse Care Settings for Older Adults.” Journal of Aging Studies 26 (2): 214–225. doi:10.1016/j.jaging.2012.01.001.
- Perry, J., and S. Beyer. 2012. “Ethical Issues around Telecare. The Views of People with Intellectual Disabilities and People with Dementia.” Journal of Assistive Technologies 6 (1): 71–75. doi:10.1108/17549451211214382.
- Perry, J., S. Beyer, and S. Holm. 2009. “Assistive Technology, Telecare and People with Intellectual Disabilities: Ethical Considerations.” Journal of Medical Ethics 35 (2): 81–86. doi:10.1136/jme.2008.024588.
- Petner-Arrey, J., and S. R. Copeland. 2014. “‘You Have to Care.’ Perceptions of Promoting Autonomy in Support Settings for Adults with Intellectual Disability.” British Journal of Learning Disabilities 43 (1): 38–48. doi:10.1111/bld.12084.
- Ricoeur, P. 1976. Interpretation Theory: Discourse and the Surplus of Meaning. Fort Worth, TX: Texas Christian University Press.
- Roeden, J. M., M. A. Maaskant, and L. M. G. Curfs. 2011. “The Views of Clients with Mild Intellectual Disabilities regarding Their Working Relationships with Caregivers.” Journal of Applied Research in Intellectual Disabilities 24 (5): 398–406. doi:10.1111/j.1468-3148.2010.00622.x.
- Scherer, M. J., and S. Federici. 2015. “Why People Use and Don’t Use Technologies: Introduction to the Special Issue on Assistive Technologies for Cognition/Cognitive Support Technologies.” NeuroRehabilitation 37 (3): 315–378. doi:10.3233/NRE-151264.
- Smith, S. 2013. “Liberal Ethics and Well-Being Promotion in the Disability Rights Movement, Disability Policy and Welfare Practice.” Ethics and Social Welfare 7 (1): 20–35. doi:10.1080/17496535.2012.671839.
- Taber-Doughty, T., J. Shurr, J. Brewer, and S. Kubik. 2010. “Standard Care and Telecare Services: Comparing the Effectiveness of Two Service Systems with Consumers with Intellectual Disabilities.” Journal of Intellectual Disability Research: JIDR 54 (9): 843–859. doi:10.1111/j.1365-2788.2010.01314.x.
- Tassé, M. J., J. B. Wagner, and M. Kim. 2020. “Using Technology and Remote Support Services to Promote Independent Living of Adults with Intellectual Disability and Related Developmental Disabilities.” Journal of Applied Research in Intellectual Disabilities: JARID 33 (3): 640–647. doi:10.1111/jar.12709.
- Vázquez, A., C. Jenaro, N. Flores, M. J. Bagnato, M. C. Pérez, and M. Cruz. 2018. “E-Health Interventions for Adult and Aging Population with Intellectual Disability: A Review.” Frontiers in Psychology 9: 2323. doi:10.3389/fpsyg.2018.02323.
- van de Velde, D., F. de Zutter, T. Satink, U. Costa, S. Janquart, D. Senn, and P. de Vriendt. 2019. “Delineating the Concept of Self-Management in Chronic Conditions: A Concept Analysis.” Bmj Open 9 (7): e027775. doi:10.1136/bmjopen-2018-027775.
- Vijfhuizen, E., and K. M. Volkers. 2016. “E-health bij burgers met een verstandelijke beperking. Beschrijving van de ontwikkeling aan een digitaal programma [E-Health for Civilians with an Intellectual Disability. Description of the Development of a Digital Program].” In Disability Studies in de Lage Landen, edited by G. van Hove, A. Schippers, M. Cardol, and E. de Schauwer, 304–319. Antwerpen, Belgium: Garant.
- Wennberg, B., and A. Kjellberg. 2010. “Participation When Using Cognitive Assistive devices-from the perspective of people with intellectual disabilities.” Occupational Therapy International 17 (4): 168–176. doi:10.1002/oti.296.
- Williams, V., and S. Porter. 2017. “The Meaning of ‘choice and control’ for People with Intellectual Disabilities who are Planning their Social Care and Support.” Journal of Applied Research in Intellectual Disabilities: JARID 30 (1): 97–108. doi:10.1111/jar.12222.
- de Wit, J., E. Dozeman, J. Ruwaard, J. Alblas, and H. Riper. 2015. “Web-Based Support for Daily Functioning of People with Mild Intellectual Disabilities or Chronic Psychiatric Disorders: A Feasibility Study in Routine Practice.” Internet Interventions. 2 (2): 161–168. doi:10.1016/j.invent.2015.02.007.
- Zaagsma, M., K. M. Volkers, M. H. M. Koning, G. van Hove, and A. P. Schippers. 2020a. “The Usefulness of Offering 24/7 Online Support within a Wider Mix of Professional Services for People with Intellectual and Developmental Disabilities Living Independently: A Qualitative, Multiple Case Study.” Inclusion 8 (2): 138–154. doi:10.1352/2326-6988-8.2.138.
- Zaagsma, M., K. M. Volkers, A. P. Schippers, J. A. Wilschut, and G. van Hove. 2019. “An Exploratory Study of the Support Needs in 24/7 Online Support for People with Mild Intellectual Disabilities.” Journal of Policy and Practice in Intellectual Disabilities 16 (1): 78–87. doi:10.1111/jppi.12275.
- Zaagsma, M., K. M. Volkers, E. A. K. Swart, A. P. Schippers, and G. van Hove. 2020b. “The Use of Online Support by People with Intellectual Disabilities Living Independently during COVID-19.” Journal of Intellectual Disability Research: JIDR 64 (10): 750–756. doi:10.1111/jir.12770.