
Abstract
Background: The Coping Questionnaire measures affected family members’ responses to their relatives’ substance misuse related problems. The Coping Questionnaire examines three main coping strategies: engaged, tolerant-inactive, and withdrawal coping. Objectives: The aim of the current study was to compare competing conceptual measurement models across two countries, including one-factor, three-factor, and higher order factor models. Methods: Secondary analysis of data from five previous studies was conducted. Samples of affected family members from England (N = 323) and Italy (N = 165) were aggregated into two country specific groups. Series of confirmatory factor analyses were performed to test the degree of model fit and the effects of socio-demographic variables on the coping factors. Results: A bifactor model fitted the data most closely relative to the one- and three-factor models. High rates of common variance (60–65%) were attributable to the general coping factor, while a high proportion of the variance related to the withdrawal coping subscale score was independent (66–89%) of the general coping factor. Family members’ country, age, gender, the type of relationship and the main problematic substance had significant effects on the coping factors. Conclusions: A bifactor model related to coping behaviors is consistent with the theoretical assumptions of the general coping literature. The concept of a general coping factor also fits the theoretical assumptions of the stress-strain-coping-support model, with family members showing a general tendency to cope with the harmful circumstances which arise due to substance misuse.
Introduction
Studies on adverse effects of alcohol misuse initially focused on the negative consequences on the drinker. A more thorough view of the harms caused by alcohol misuse should also include the negative impact of alcohol use on family members and other close personal relationships (Laslett, Callinan, & Pennay, Citation2013; Ramstedt et al., Citation2015; Rossow, Felix, Keating, & McCambridge, Citation2016). According to a national survey from Australia (N = 2649; Laslett et al., Citation2011), 16% of the adult participants experienced at least one harm during the last 12 month period due to the alcohol use of a household member, relative, or intimate. Family members could experience verbal or physical abuse due to a close relative or partner’s drinking, or they might have to care for the intoxicated person (Jiang, Callinan, Laslett, & Room, Citation2015; Storvoll, Moan, & Lund, Citation2016). As a consequence, those affected family members who were exposed to a harm from a partner or close relative’s drinking reported lower psychological well-being, higher distress, and symptoms of depression or anxiety (Greenfield, Karriker-Jaffe, Kaplan, Kerr, & Wilsnack, Citation2015; Karriker-Jaffe, Greenfield, & Kaplan, Citation2017).
The Stress-Strain-Coping-Support (SSCS) model provides a theoretical framework to examine the impact of a relative’s substance misuse on the family members’ well-being and adjustment to stressors (Orford, Copello, Velleman, & Templeton, Citation2010; Velleman & Templeton, Citation2003). The SSCS model assumes that a relative’s excessive alcohol or drug consumption could create a long-lasting and highly stressful family environment. Affected family members could experience a wide range of burdens related to the relative’s substance misuse, such as physical and verbal violence, financial problems, feelings of worry or uncertainty about the relative’s well-being, or negative effects on the family atmosphere. As a consequence, affected family members could be at risk of experiencing stress-related strain on their physical and mental health including substance use disorders, depression, decreased self-esteem, or psychosomatic symptoms (Orford, Copello, et al., Citation2010; Orford, Velleman, Copello, Templeton, & Ibanga, Citation2010; Orford, Velleman, Natera, Templeton, & Copello, Citation2013; Ray, Mertens, & Weisner, Citation2007; Velleman & Templeton, Citation2003).
Orford et al.s’ theoretical concept suggests that there might be a general tendency towards coping among affected family members, as they try to interpret and deal with the adverse conditions related to the misusing relative’s behavior (Orford, Copello, et al., Citation2010; Orford, Velleman, et al., Citation2010). By using a variety of different coping techniques, the family members have the ability to actively influence processes within the family, thereby possibly reducing the harmful effects of stress and strain (Orford, Copello, et al., Citation2010; Orford, Velleman, et al., Citation2010; Velleman & Templeton, Citation2003).
To measure and explore the affected family members’ responses to the substance misuse related problem within the family, Orford et al. designed the Coping Questionnaire (CQ). Originally, it contained 68 items with the purpose of reflecting a hypothesized eight-factor structure (Orford et al., Citation1992; Orford, Templeton, Velleman, & Copello, Citation2005, Citation2010). However, exploratory factor analysis yielded three factors underlying the various coping strategies: engaged, tolerant-inactive, and withdrawal coping (Orford et al., Citation1998, Citation2001). With engaged coping, the family member tries to control and protect the family processes via assertive, supportive, or emotional reactions. The tolerant-inactive coping factor contains elements of acceptance or support for the substance misuse and self-sacrificing behavior. Withdrawal coping refers to techniques which enable family members to focus on their own needs and to distance themselves from the misusing relative (Orford, Velleman, et al., Citation2010; Orford et al., Citation2013). The revised, 30 item-long version of the CQ was developed based on this three-factor model of coping behavior (Orford et al., Citation2005).
These three factor analytically derived categories of coping strategies have been measured in several countries and sociocultural groups over the last few decades (Arcidiacono et al., Citation2010; Lee et al., Citation2011; Orford et al., Citation1998, Citation2001; Orford, Padin, et al., Citation2017). In general, tolerant-inactive and engaged coping styles were positively associated and withdrawal coping was not associated with psychological or physical symptoms among family members. However, some possible differences between sociocultural groups were observed: for example it is assumed that family members from more individualistic cultural backgrounds might show higher levels of withdrawal coping, while family members from collectivistic countries might be more likely to react with tolerant-inactive coping and less likely with withdrawal coping strategies in response to a relative’s substance misuse (Ahuja, Orford, & Copello, Citation2003; Arcidiacono et al., Citation2010; Orford et al., Citation2001).
Previous studies have already provided evidence of similarities and differences in coping behavior among affected family members across various sociocultural groups. Therefore, the main aim of the current study is to compare competing conceptual measurement models across several samples from England and Italy. The present study compared the model fit of the original three-factor structure of the SSCS in comparison to a general one-factor and bifactor models; and examined the relationship between the coping factors and socio-demographic variables.
Materials and methods
Participants and procedure
In order to perform confirmatory factor analysis across sociocultural groups, the current research aggregated data from various samples. Participants from five, independent samples were involved in the study. They were categorized into two country-specific groups (England: N = 323; Italy: N = 165) to ensure a sufficient sample size for further data analysis. The inclusion criteria for the respondents across the different samples were similar, which supported the integration of the data from different sources. Generally, affected family members were eligible to participate if they had a close relationship (e.g. living together, or having frequent contacts) with a relative showing alcohol or drug misuse over the last six months, which contributed to the family member experiencing a high level of stress. Other than in the sample from the UK Alcohol Treatment Trial (UKATT), participants’ self-defined criteria were applied for defining alcohol or drug misuse. Because the original studies focused on the experiences of the affected family members, they did not aim to specify parameters for drinking or drug use among relatives.
However, in case of the aggregated sample from England, the family members might have had divergent characteristics related to their participation, as their data were gathered from three separate research projects. One group of family members were recruited for a research project to discover more about the impact of living with a relative with a substance problem (Sample 1, Family coping in South-West England; Orford et al., Citation1998, Citation2001); a second group of family members were recruited opportunistically in general practice health settings to participate in a research project to test an intervention aimed at helping them as affected family members (Sample 2, Primary Care Project II; Copello et al., Citation2009); while another group of participants (Sample 3) provided data as part of the UK Alcohol Treatment Trial (UKATT), 12 months after their misusing relatives started their own treatment. Possibly due to the fact that their substance misusing relative had received treatment, commencing 12 months previously, participants within Sample 3 (interviewed 12 months after their relative had entered treatment) showed significantly lower rates of coping strategies, family distress and psychosomatic symptoms compared to family members of Sample 2 (). Thus, some level of heterogeneity was present within the aggregated English sample. Nevertheless, family members from Sample 3 still reported frequent alcohol problem-induced distress in the family. For example, high proportions of these family members often experienced distress because their relatives had changeable moods, and often worried that the relative’s working ability, health and mental state were affected by the drinking problem (). Due to the relatively high level of distress experienced by these family members, it was reasonable to combine coping-related data from Sample 3 with Samples 1–2. It was also assumed that by merging these samples a broader spectrum of family members from the UK would be represented in the analyses. Interested readers can find more detailed data of the three subsamples from England in the Supplementary materials (see: and ). However, in the present study it was not proposed to examine differences in terms of coping, family impact and psychosomatic symptoms between the included subsamples.
Figure 1. Competing measurement models of the Coping Questionnaire.
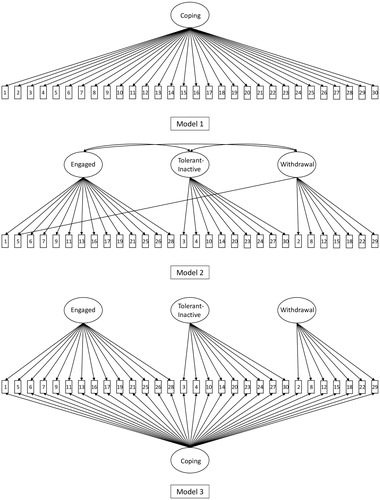
Table 1. Socio-demographic characteristics of the affected family members in the different samples.
The aggregated Italian sample combined participants from two separate studies. The majority of the Italian family members were recruited for a cross-sectional study which investigated the harmful effects of alcohol and drug use on the experiences of family members from three Italian regions (Sample 4; Arcidiacono et al., Citation2010). A second group of Italian individuals participated in an intervention which proposed to provide assistance for affected family members (Sample 5; Velleman, Arcidiacono, Procentese, Copello, & Sarnacchiaro, Citation2008).
Two of the data sources used a longitudinal design (Samples 2 & 5): in these cases, only data from the baseline or the pre-intervention were examined.
The participants were recruited from various sources; for example, the family members got in touch with local health (e.g. general practitioner) or social services, or they became involved through their misusing relative who was under treatment, or they got informed via public advertisement (Orford et al., Citation2005). No participant was paid to participate in any of these studies. Generally, the participants self-completed the CQ during a semi-structured interview. Affected family members also provided data on several other measures in each of the samples (Orford et al., Citation2005; Orford, Templeton, et al., Citation2010). For example, they estimated the degree of harmful impact and distress in the family’s life as a consequence of alcohol or drug misuse (Family Member Impact, FMI; Samples 2-4), and self-rated their own level of psychological and physical symptoms (Symptom Rating Test, SRT; Samples 1-5). As the present study set out to investigate the structure of coping, it was not proposed to examine associations between coping dimensions and family impact, psychosomatic symptoms, severity of alcohol or drug problem, especially as these analyses have been already reported in previous publications (Arcidiacono et al., Citation2010; Copello et al., Citation2009; Orford et al., Citation1998, Citation2001; Velleman et al., Citation2008, Citation2011).
The main socio-demographic characteristics of the selected samples are presented in . Further details of methodological procedure can be found in the original studies.
Instruments
Coping Questionnaire (CQ)
The scale developed by Orford et al. measures the characteristics of the coping strategies utilized by the affected family members related to their relative’s alcohol, drug or gambling misuse problem (Orford et al., Citation2005; Orford, Templeton, et al., Citation2010). Participants assess on a 4-point Likert-scale the extent to which they have used each coping technique during the last three months. The present research explored the structure of coping behavior by using the 30 item-long form of the CQ. For Sample 1 from England, the affected family members used the longer (68-item) version of the questionnaire (Orford et al., Citation1998); for this sample, the only items used for the present data analysis were those which correspond with the items of the revised 30 item form of the CQ.
Statistical analysis
The present study tested three different conceptual models of the CQ across two countries. During the confirmatory factor analyses the items of the questionnaire were specified as ordered categorical variables. Therefore, the models were estimated by using Weighted Least Squares Mean and Variance (WLSMV) adjusted estimation method with Delta parameterization. The competing measurement models are displayed in . As a default and reference model, the study tested a one-dimensional model, where all the items of the CQ were loaded on the general or global factor of coping (Model 1). To reflect on the original concept of the CQ, Model 2 contained three first-order factors (engaged, tolerant-inactive and withdrawal), where the latent factors were allowed to correlate with each other. As an alternative approach, the statistical analyses included the test of a bifactor model (Model 3). This model covered three specific coping factors (engaged, tolerant-inactive and withdrawal), and a general or global factor of coping. Therefore, each of the observed items was not only loaded on the related specific coping factors, but also on the general factor. Due to the assumption of the underlying general or global factor of coping, item 5 (“Sat down together with him and talked frankly about what could be done about his drinking [or drug use]”) was only allowed to load on the specific factor of engaged coping and on the general factor. As a general constraint on the bifactor model, the correlation between the specific coping factors and the general coping factor were specified at zero. The reliability and strength of the general and specific coping factors for the bifactor model were estimated by the values of Explained Common Variance (ECV), Omega, Omega Hierarchical, H- and PUC-index.
In order to test the fit of the proposed models, analyses were conducted by using Mplus 8.0 (Muthén & Muthén, Citation2017). First, the three different models were separately assessed and evaluated across the two countries based on multiple model fit indices. The index of Root Mean Squared Error of Approximation (RMSEA) shows optimal fit under 0.05 and satisfactory fit under 0.08. The Closeness of fit test related to RMSEA (Cfit of RMSEA) displays the probability that the estimate of RMSEA is not significantly different from 0.05; thus, non-significant p-values (p > .05) refers to excellent model fit. The value of Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) should be at least around 0.90-0.95 in case of adequate fit. Finally, a Multiple Indicator Multiple Causes (MIMIC) model was assessed to explore the relationship between socio-demographic covariates and coping factors. The direct effects of family members’ country, age, gender, the type of relationship between the misusing relative and family member, and the main problematic substance were tested in the model.
Results
Confirmatory factor analysis (CFA)
In order to find the best fitting model related to the CQ, three measurement models were assessed and contrasted with each other. The series of analyses was conducted separately on samples from England and Italy. contains the model fit results for the one-, three-factor and bifactor model.
Table 2. Degree of model fit of the three measurement models in England and Italy.
As a measure of absolute fit, the χ2 test showed significant (p < .001) results for all the proposed models in each of the two sociocultural groups. Significant results of the χ2 test indicated lack of model fit for the estimated models. The bifactor model (Model 3) demonstrated significantly better fit compared to the three-factor model (Model 2; England: Δχ2(26) = 442.09, p < .001; Italy: Δχ2(26) = 156.12, p < .001) and compared to the one-factor model (Model 1; England: Δχ2(30) = 544.72, p < .001; Italy: Δχ2(30) = 252.20, p < .001). Also, the three-factor model (Model 2) fitted the data more closely than the one-factor model (Model 1; England: Δχ2(4) = 105.55, p < .001; Italy: Δχ2(4) = 50.47, p < .001).
However, the χ2 test has substantial limitations in the case of analyses on larger samples or with indicators showing non-normal distribution (Hooper, Coughlan, & Mullen, Citation2008). Therefore, the extent of fit of the proposed models was also evaluated based on more permissive and flexible measures of model fitness (RMSEA, CFI, TLI). These fit indices showed an adequate level or close to the acceptable level of fit to the data in England and Italy for the bifactor model (Model 3). The one-factor model (Model 1) revealed unacceptable level of fit in both countries. Generally, the various fit indices did not indicate sufficient fit for the three-factor model (Model 2), with values only in a few cases reaching a satisfactory level.
The factor loadings and reliability estimates of the bifactor model are displayed in . Only two items (12., 29.) showed non-significant factor loadings on the global coping factor for both countries. Both items loaded significantly on the specific factor of withdrawal coping. In the case of the tolerant-inactive coping factor, four items (3., 4., 20., 27.) did not present significant factor loadings in either country. Instead of the specific coping factor, these items rather related to the general coping factor.
Table 3. Standardized factor loadings and reliability indices of the bifactor model.
The general coping factor explained 60-65% of the common variance, which indicated that a high proportion of the common variance was attributable to the general coping factor. Similarly, the PUC-index showed that 66% of the correlations in the models related directly to the general coping factor. The specific factors of engaged and withdrawal coping each explained smaller proportions of the common variance (15-16%), whereas tolerant-inactive coping explained only a marginal amount of the common variance (5-8%). According to the reliability results of omega and omega hierarchical, the general coping factor was measured accurately. In the case of the general coping factor, 92-95% of the variance of the total coping score was attributable to the combination of the general and specific coping factors (omega), and 78-81% of the variance of the total score was attributable only to the general coping factor (omega hierarchical). The specific factors of engaged and tolerant-inactive coping showed higher rates (79-93%) of explained variance due to the combination of the general and the given specific coping factor. As only 9-20% of the variance of the tolerant-inactive subscale score was explained by the underlying specific factor, this might indicate that the main part of the variance of the tolerant-inactive subscale score is attributable to the general coping factor. Contrary to that, the 51-63% of the variance of the withdrawal subscale score was explained only by the underlying specific factor. Thus, the high rates of the variance in the subscale score were independent (66–89%) of the general coping factor, and contained more diverse information relative to the general coping factor. The latent factors of general coping, engaged and withdrawal coping showed higher value than the defined cutoff for H-index (0.7), which might imply that these factors are satisfactorily specified.
MIMIC Model
The direct effects of family members’ country, age, gender, the type of relationship between the misusing relative and family member, and the main problematic substance on the coping factors of the bifactor model were tested in a MIMIC model. The standardized regression coefficients of the covariates predicting the coping factors are presented in . The MIMIC model displayed an adequate level of model fit. Higher levels of general coping were predicted if the family member was from England, and if the relative did not misuse alcohol. Family members reported higher rates of engaged coping if they were from Italy, were in the younger age group, and if the misusing relative was a partner or child. Being female, and being an Italian family member, and having a relative who misused alcohol, significantly predicted elevated rates of tolerant-inactive coping. Higher levels of withdrawal coping were significantly associated with English family member status and younger age group.
Table 4. Standardized regression coefficients of the covariates predicting the coping factors (MIMIC-model, Model 3).
Discussion
The present paper focused on the examination of the factor structure of the CQ across samples from England and Italy. The study compared three measurement models; only the bifactor model reached a level of sufficient fit in both countries. Therefore, the results of the confirmatory factor analysis did not support the original, three-factor model (Orford et al., Citation1998). Similarly, results of confirmatory factor analysis among Brazilian family members indicated insufficient model fit for the original, three-factor model (Sola et al., Citation2018).
Bifactor models tend to be adequately suited to health and clinical psychology-related concepts (Rodriguez, Reise, & Haviland, Citation2016a). Thus such models have been applied to several psychological measures already, for example in the cases of psychopathological distress (Urbán et al., Citation2014), well-being (Jovanović, Citation2015) and depression (Yang, Tommet, & Jones, Citation2009). A bifactor model contains orthogonal general and specific group factors on the same conceptual level. Such models assume that covariance between the items could be explained by a common tendency and specific features of a psychological concept at the same time. In the case of a multidimensional measure, a bifactor model allows the provision of separate assessments of individual characteristics along the specific factors and the shared general tendency (Chen, Hayes, Carver, Laurenceau, & Zhang, Citation2012; Reise, Morizot, & Hays, Citation2007).
Current results indicate that each of the items of the CQ simultaneously loads on one of the specific and original coping factors (engaged, tolerant-inactive, withdrawal) and on the general coping factor. Based on that finding, among the affected family members, both specific coping styles and a general tendency to cope with the adverse circumstances could be detected. The application of a bifactor model of coping behaviors has shown consistency with the theoretical assumptions of the general coping literature. Skinner and colleagues hypothesized a multidimensional framework of coping, which was formed by specific coping instances and coping strategies at the lower level and higher level adaptive processes (Skinner, Edge, Altman, & Sherwood, Citation2003). In line with Skinner and colleagues’ concept, bifactor models showed satisfactory fit for questionnaires measuring general coping behaviors among high-school students and military officers (Ouyang, Xin, & Chen, Citation2016; Zhang et al., Citation2014). Overall, these studies identified a general coping resource factor beyond the specific coping factors (e.g. avoidance), which might play an important role in predicting psychological and physical health and maladjustment.
The concept of the general coping factor also fits the theoretical assumptions of the SSCS-model. Orford et al. proposed that affected family members show a general tendency to react to and understand the harmful circumstances in the family as a consequence of a relative’s substance misuse. Family members often experience uncertainty in deciding which coping techniques would be helpful; hence they tend to use different forms of coping strategies simultaneously (Orford, Copello, et al., Citation2010; Orford, Velleman, et al., Citation2010). Accordingly, the different forms of coping behavior cannot be clearly separated, contributing to the general coping factor which subsumes each of the CQ items irrespective of their relation to the specific factors. Contrary to the theory behind Al-Anon (Hurcom, Copello, & Orford, Citation2000), the concept of the general coping factor might indicate that it is not reasonable to separate coping behaviors into categories of ‘adequate’ or ‘undesirable’ reactions, as the broad trait of coping contains strategies with very different characteristics. The SSCS-model assumes that in different life circumstances there is no universally adequate coping reaction to attenuate the adverse effects of stress, as each of the coping styles might be beneficial or detrimental in different situations. Based on that, the 5-Step Method (an intervention based on the SSCS Model) aims to assist family members to explore the advantages and disadvantages of possible coping alternatives, and to cope in the way that they feel is best suited to their circumstances (Copello, Templeton, Orford, & Velleman, Citation2010b).
The overall score of coping attempts measured by the CQ in previous studies could be considered as a possible evaluation of the general coping factor. Higher levels of total coping imply that family members apply various coping techniques with higher frequency. Presumably, in the case of the CQ, the general coping factor is less likely to indicate general resourcefulness, but rather reflects family members’ pervasive ambivalence or uncertainty about how best to cope with the stressful impacts related to their relatives’ substance misuse. Studies which have assessed the effects of the 5-Step Method intervention have shown significant reductions in the overall coping score (Velleman et al., Citation2011), which might be related to the fact that the family members better understood the associations between the substance misuse and their own health status after the intervention (Copello, Templeton, Orford, & Velleman, Citation2010a). Previous results also showed that – similarly to the specific factors of engaged and tolerant-inactive – elevated rates of overall coping were associated with the relative’s active substance misuse, and with family members’ negative health outcomes (Arcidiacono et al., Citation2010; Velleman et al., Citation2011). The present findings demonstrate that considerable parts of the variance of the engaged and tolerant-inactive subscale scores were attributable to the general coping factor, which might indicate a correspondence between these specific and global factors. However, the subscale score of withdrawal coping contained more diverse information relative to the general coping factor, as these items emphasize the family members’ focus on their own lives instead of them directly reacting to their relatives’ misuse.
The identified bifactor measurement structure has important conceptual consequences. Moderate levels of the PUC and ECV values (< 0.70) related to the general coping factor indicated that coping strategies measured by the CQ should be considered as a multidimensional construct (Rodriguez et al., Citation2016a; Rodriguez, Reise, & Haviland, Citation2016b). Thus, most of the coping items’ variance drew on a specific, distinct coping dimension over and above the broad coping factor. In practical terms this would imply that the CQ could be used in two ways in research and practice. First, results of various reliability indices indicated adequate measurement of the general coping factor (i.e. substantial factor loadings, and high proportion of the variance attributable to the general factor). Thus, a high overall score of coping derived from the sum of all items of the CQ might represent family members’ broad feelings of ambivalence or uncertainty about how best to cope with the stressful impacts related to their relatives’ substance misuse. In practical or therapeutic terms, these issues are precisely what is discussed with affected family members who work with the 5-Step Method (Copello et al., Citation2010b), especially when they work on Step 3, which examines coping. Second, reliability indices provided evidence of reliable measurement and specification of the withdrawal latent coping factor (i.e. higher rates of Relative Omega, ECV and H-index). Therefore, reliability indices consistently suggested that scores on the general coping and specific withdrawal scales are sufficiently reliable to be used in research and practice.
However, the present findings also suggested that the questionnaire might show an inability to provide precise estimation of engaged and tolerant-inactive coping (i.e. low rates of ECV, H-index and Relative Omega). Due to that, the instrument’s clinical utility is reduced as it was not able to identify and measure engaged and tolerant-inactive coping distinctly. Omega estimates related to the engaged and tolerant-inactive factors substantially reduced after controlling for the effect of general coping. Thus the engaged and tolerant-inactive coping items should be estimated as a part of general coping and not specifically as separate entities (Rodriguez et al., Citation2016b). From a practical perspective, this indicates that, as well as the general coping score, the only sub-scale scores which should be used are ones relating to the withdrawal coping factor, as the other specific subscales did not contain unique information over and above the effect of the general coping factor.
These findings might indicate that two broad categories represent coping among affected family members: approach and avoidance. The former dimension incorporates engaged and tolerant-inactive coping. Thus, approach coping reflects strategies which focus on the relative with substance misuse problems and attempts a problem- or emotional-focused engagement towards the relative. Scores on the general coping factor might be considered to measure this coping category. Avoidance coping might be represented by the specific factor of withdrawal coping. This structure also corresponds with the general coping literature. It was suggested that inclusion of higher-order constructs of approach/engagement and avoidance/disengagement coping might allow more precise categorization of coping behaviors (Skinner et al., Citation2003; Tobin, Holroyd, Reynolds, & Wigal, Citation1989). As a supplementary analysis, the present study tested model fitness of an alternative, bifactor measurement model which simultaneously consisted a general coping factor and two specific factors: one comprised of engaged and tolerant-inactive subscale items and the second comprised of withdrawal coping strategy items. This solution reached an adequate level of model fitness in both samples (). However, at an item-level the bifactor model with two specific factors demonstrated a less appropriate solution, since more items did not have significant factor loadings on the general and specific factors than was the case for the bifactor model with three specific factors ().
In general, findings from the present study have indicated that use of the CQ is recommended in research and practice to measure coping behavior among affected family members. Previous studies presented the validity of the questionnaire in various populations, such as among family members with relatives showing alcohol, drug or gambling problems (Orford et al., Citation2005; Orford, Templeton, et al., Citation2010). Moreover, the CQ has been considered as a widely-used instrument in psychosocial interventions for addiction-affected family members (Rane et al., Citation2017). It is recommended for use as a longitudinal assessment tool for interventions which primarily focus on the needs of affected family members (Copello et al., Citation2010a), and for family-based interventions where the substance misusing relative and affected family members jointly participate, such as behavioral couples therapy or the community reinforcement approach (Copello, Velleman, & Templeton, Citation2005). The instrument is also suitable for monitoring affected family members’ reactions related to the behavior of the substance misusing relative. Therefore, future, therapeutic community-based studies might consider monitoring changes in family members’ coping responses over time by changing the defined time perspective of the CQ from the past three months to the past week or month. However, because coping strategies may vary over time, retrospective measurement of coping might be biased (Stone et al., Citation1998). Therefore, in the future, we suggest that coping of family members might be measured with experience sampling methods or daily diary data (Aldridge-Gerry et al., Citation2011; Roesch et al., Citation2010; Stone et al., Citation1998). Orford et al. now recommend using one scale (the Short Questionnaire for Family Members Affected by Addiction) which examines all four components of the Stress-Strain-Coping-Support model, and which includes a shortened, 12 item-long version of the CQ measuring four dimensions of coping strategies: (i) Engaged-Emotional, (ii) Engaged-Assertive, (iii) Tolerant-Inactive and (iv) Withdrawal-Independent coping (Buchner, Koytek, Fischer, Wodarz, & Wolstein, Citation2016; Orford, Cousins, Smith, & Bowden-Jones, Citation2017).
From a practical perspective, it would be also important to explore how affected family members perceive the usefulness of each specific coping strategy. The present study did not aim to measure this aspect, nor, to our knowledge, have other quantitative studies using the CQ done so. However, previous qualitative findings have provided some indication about family members’ own views on coping behavior (Copello et al., Citation2010a, Citation2010b; Orford, Templeton, Patel, Copello, & Velleman, Citation2007; Orford, Velleman, et al., Citation2010). In general, family members recognize that there are both advantages and disadvantages related to each of the coping strategies, supporting the assumption that their effectiveness depends on the particular situation that family members find themselves in. Nevertheless, these qualitative findings do suggest that family members perceive both withdrawal and assertive coping strategies generally to be more useful. By using these types of coping they report gaining an elevated focus on their own needs, greater feelings of self-efficacy, and calmer and more direct communication with the substance misusing relative. By contrast, more emotional coping strategies were viewed as detrimental in many circumstances, as these approaches sometimes lead to higher rates of fighting and aggressive acts within the family. Coping strategies tolerant of the substance using relatives’ continued use (such as providing money for them to buy substances) were also often perceived as counterproductive actions by family members (Copello et al., Citation2010a, Citation2010b; Orford et al., Citation2007; Orford, Velleman, et al., Citation2010).
Finally, the present study also tested the effects of socio-demographic variables on the coping factors. The results of the MIMIC model supported the approach which assumes that the affected family members’ experiences and coping attempts might differ based on socio-demographic factors, such as the relationship of the family member with the misusing relative (Orford, Citation2017). Similarly to previous studies, the analysis detected differences in the level of coping between the two countries (Arcidiacono et al., Citation2010). Family members from Italy showed higher levels of tolerant-inactive and engaged coping, whereas family members from England had higher rates of general and withdrawal coping. More family-oriented cultural values might explain the pattern of the coping profile among family members from Italy (Arcidiacono et al., Citation2010). In case of tolerant-inactive coping a significant effect of gender was also presented, as women were more likely to use tolerant-inactive coping attempts. As a consequence of sex-role socialization, women might react with more self-sacrificing coping techniques, or might be more likely to tolerate the stressful family environment; or it simply might be safer for women to be tolerant-inactive as opposed to being either more engaged or more withdrawing (Orford et al., Citation2001; Orford, Velleman, et al., Citation2010). Moreover, the type of relationship between the family member and the misusing relative also affected the frequency of coping attempts. Family members reported higher rates of engaged coping if the misusing relative was a partner or a child. It is possible that, in general, being a partner or a parent implies a closer relationship between the family member and the substance using relative. If that is the case, the family members might increasingly experience burden and feelings of concern, due to the substance misuse; implying that it is possible that partners and parents of misusing relatives might more actively try to control and influence their relatives’ behavior (Orford, Citation2017; Orford, Padin, et al., Citation2017).
The SSCS-model assumes that experiences and coping of affected family members show substantial similarities, but that characteristics of family members and relatives (e.g. type of problematic substance and relationship) might moderate these outcomes among family members (Orford, Velleman, et al., Citation2010). Depending on the type of relationship with the substance misusing relative, family members have different options for coping with the experienced difficulties. For example, those family members who have a more dependent structural position with the relative (e.g. children of parents who drink excessively) might have less opportunities to apply assertive or independent coping strategies (Orford, Citation2017). Subgroup specific examination of coping strategies among affected family members would be recommended, with a special focus on testing the structural subordination and dependence hypothesis (Orford, Citation2017). For example, exploring significant interaction effects between these characteristics (e.g. nature of the problematic substance X type of relationship) would provide a more precise and subgroup-specific description and comparison of coping behaviors among family members. From a practical perspective, these findings would provide additional details for therapists or counselors when exploring coping resources among different subgroups of family members (e.g. for a given coping strategy different advantages and disadvantages might be relevant for an affected child as opposed to a mother).
Limitations and future direction
Several limitations have been identified related to the present research. Although the study examined the factor structure of the CQ across two countries, in the case of the Italian sample the results must be interpreted with caution due to the smaller sample size. Further bias might be caused by the aggregated nature of the English data gathered from three separate studies. As a consequence, family members might have experienced different severities of substance misuse depending on which study they were included in. It is possible that there is heterogeneity that is unaccounted for in the English samples, in that participants within Sample 1 were recruited for an exploratory research project about the experiences of affected family members, participants within Sample 2 were family members opportunistically recruited in primary healthcare for a treatment RCT to help affected family members, and participants within Sample 3 were recruited via their misusing relative, 12-months after these relatives had started their own treatment. Family members in Sample 2 showed significantly higher levels of use of coping strategies, distress in the family, and psychosomatic symptoms compared to participants from Sample 3 (family members of those treated in the UKATT project). Similarly, as not all of the included studies used the same version of the CQ, there might have been discrepancies between the datasets for that reason as well. Some of the datasets also contained missing socio-demographic data, which might have affected the results of the MIMIC model. Finally, the present results are dependent on the breadth and adequacy of the set of items included in the questionnaire. It is possible that certain ways of coping, including those recommended by Al-Anon, might be insufficiently represented (e.g. marital games). Future research might consider exploring alternative ways of coping.
Conclusions
The present research examined the factor structure of the CQ in two different countries. The findings suggest that a bifactor model fits most accurately to the coping attempts measured by the questionnaire. Future research might explore the relationship between the specific factors and the general coping factor, for example measuring the potential mediating role of self-efficacy or appraisal (Zhang et al., Citation2014). Based on Skinner’s theoretical model, the general coping factor might have a key role in predicting health-related outcomes (Skinner et al., Citation2003); therefore it would be important for future research to clarify the possible mechanisms related to the general coping factor. Moreover, a person-oriented examination of the coping styles might allow the identification of latent classes or subgroups of family members in future research. Finally, more precise measurement of coping strategies among affected family members would be possible through longitudinal design, for example using experience sampling methods or daily diary data (Roesch et al., Citation2010; Stone et al., Citation1998).
Supplemental Material
Download MS Word (27.6 KB)Acknowledgements
The present study reanalyzed and summarized data from previous studies (Arcidiacono et al., Citation2010; Copello et al., Citation2009; Orford et al., Citation1998; The UKATT Research Team, Citation2001; Velleman et al., Citation2008). Original studies were funded by the West Midlands Regional Health Authority and the Alcohol Education and Research Council, the Avon and Wiltshire Regional Health Authorities (Copello et al., Citation2009); the Medical Research Council, National Health Service Executive in England, and Wales Office for Research and Development in Health and Social Care (The UKATT Research Team, Citation2001), the ‘‘National Fund for the Fight against Drugs’’, Ministry of Health, Prevention and Communication Department, Government of Italy (Velleman et al., Citation2008).
Disclosure statement
The authors declare that all procedures of the original studies followed the ethical standards of the Declarations of Helsinki. Informed consent for inclusion in the original studies was obtained from all the participants. The original studies were all approved by the appropriate research and ethical committees.
Zsolt Horváth (ZsH), Jim Orford (JO), Richard Velleman (RV) and Róbert Urbán (RU) wrote the manuscript. JO and RV designed the original studies and performed data collection. ZsH conducted statistical analysis under RU’s supervision.
Additional information
Funding
References
- Ahuja, A., Orford, J., & Copello, A. (2003). Understanding how families cope with alcohol problems in the UK West Midlands Sikh Community. Contemporary Drug Problems, 30(4), 839–873.
- Aldridge-Gerry, A. A., Roesch, S. C., Villodas, F., McCabe, C., Leung, Q. K., & Da Costa, M. (2011). Daily stress and alcohol consumption: Modeling between-person and within-person ethnic variation in coping behavior*. Journal of Studies on Alcohol and Drugs, 72(1), 125–134. doi:10.15288/jsad.2011.72.125
- Arcidiacono, C., Velleman, R., Procentese, F., Berti, P., Albanesi, C., Sommantico, M., & Copello, A. (2010). Italian families living with relatives with alcohol or drugs problems. Drugs: Education, Prevention and Policy, 17(6), 659–680. doi:10.3109/09687630902824262
- Buchner, U., Koytek, A., Fischer, U., Wodarz, N., & Wolstein, J. (2016). Psychometrische Evaluation des deutschen Kurzfragebogens für suchtbelastete Familienmitglieder SQFM-AA (Version Glücksspiel) [Psychometric Evaluation of the German Version of the Short Questionnaire for Family Members – Affected by Addiction SQFM-AA (Gambling)]. Ppmp - Psychotherapie · Psychosomatik · Medizinische Psychologie, 66(3–4), 155–162. doi:10.1055/s-0042-100812
- Chen, F. F., Hayes, A., Carver, C. S., Laurenceau, J.-P., & Zhang, Z. (2012). Modeling general and specific variance in multifaceted constructs: A comparison of the bifactor model to other approaches: Bifactor modeling of multifaceted constructs. Journal of Personality, 80(1), 219–251. doi:10.1111/j.1467-6494.2011.00739.x
- Copello, A., Templeton, L., Orford, J., & Velleman, R. (2010a). The 5-Step Method: Evidence of gains for affected family members. Drugs: Education, Prevention and Policy, 17(sup1), 100–112. doi:10.3109/09687637.2010.514234
- Copello, A., Templeton, L., Orford, J., & Velleman, R. (2010b). The 5-Step Method: Principles and practice. Drugs: Education, Prevention and Policy, 17(sup1), 86–99. doi:10.3109/09687637.2010.515186
- Copello, A., Templeton, L., Orford, J., Velleman, R., Patel, A., Moore, L., … Godfrey, C. (2009). The relative efficacy of two levels of a primary care intervention for family members affected by the addiction problem of a close relative: A randomized trial. Addiction, 104(1), 49–58. doi:10.1111/j.1360-0443.2008.02417.x
- Copello, A., Velleman, R., & Templeton, L. (2005). Family interventions in the treatment of alcohol and drug problems. Drug and Alcohol Review, 24(4), 369–385. doi:10.1080/09595230500302356
- Greenfield, T. K., Karriker-Jaffe, K. J., Kaplan, L. M., Kerr, W. C., & Wilsnack, S. C. (2015). Trends in Alcohol’s Harms to Others (AHTO) and Co-occurrence of Family-Related AHTO: The Four US National Alcohol Surveys, 2000–2015. Substance Abuse: Research and Treatment, 9(S2), 23–31. doi:10.4137/SART.S23505
- Hooper, D., Coughlan, J., & Mullen, M. (2008). Structural equation modelling: Guidelines for determining model fit. The Electronic Journal of Business Research Methods, 6(1), 53–60.
- Hurcom, C., Copello, A., & Orford, J. (2000). The family and alcohol: Effects of excessive drinking and conceptualizations of spouses over recent decades. Substance Use & Misuse, 35(4), 473–502. doi:10.3109/10826080009147469
- Jiang, H., Callinan, S., Laslett, A.-M., & Room, R. (2015). Correlates of caring for the drinkers and others among those harmed by another’s drinking: Caring for others. Drug and Alcohol Review, 34(2), 162–169. doi:10.1111/dar.12175
- Jovanović, V. (2015). Structural validity of the Mental Health Continuum-Short Form: The bifactor model of emotional, social and psychological well-being. Personality and Individual Differences, 75, 154–159. doi:10.1016/j.paid.2014.11.026
- Karriker-Jaffe, K. J., Greenfield, T. K., & Kaplan, L. M. (2017). Distress and alcohol-related harms from intimates, friends, and strangers. Journal of Substance Use, 22(4), 434–441. doi:10.1080/14659891.2016.1232761
- Laslett, A.-M., Callinan, S., & Pennay, A. (2013). The increasing significance of alcohol’s harm to others research. Drugs and Alcohol Today, 13(3), 163–172. doi:10.1108/DAT-11-2012-0010
- Laslett, A.-M., Room, R., Ferris, J., Wilkinson, C., Livingston, M., & Mugavin, J. (2011). Surveying the range and magnitude of alcohol’s harm to others in Australia: Alcohol’s harm to others. Addiction, 106(9), 1603–1611. doi:10.1111/j.1360-0443.2011.03445.x
- Lee, K. M. T., Manning, V., Teoh, H. C., Winslow, M., Lee, A., Subramaniam, M., … Wong, K. E. (2011). Stress-coping morbidity among family members of addiction patients in Singapore: Stress-coping among relatives of the addicted. Drug and Alcohol Review, 30(4), 441–447. doi:10.1111/j.1465-3362.2011.00301.x
- Muthén, L. K., & Muthén, B. O. (2017). Mplus: Statistical analysis with latent variables. User’s guide (8th ed.). Los Angeles, CA: Muthén & Muthén.
- Orford, J. (2017). How does the common core to the harm experienced by affected family members vary by relationship, social and cultural factors? Drugs: Education, Prevention and Policy, 24(1), 9–16. doi:10.1080/09687637.2016.1189876
- Orford, J., Copello, A., Velleman, R., & Templeton, L. (2010). Family members affected by a close relative’s addiction: The stress-strain-coping-support model. Drugs: Education, Prevention and Policy, 17(sup1), 36–43. doi:10.3109/09687637.2010.514801
- Orford, J., Cousins, J., Smith, N., & Bowden-Jones, H. (2017). Stress, strain, coping and social support for affected family members attending the National Problem Gambling Clinic, London. International Gambling Studies, 17(2), 259–275. doi:10.1080/14459795.2017.1331251
- Orford, J., Natera, G., Davies, J., Nava, A., Mora, J., Rigby, K., … Velleman5, R. (1998). Tolerate, engage or withdraw: A study of the structure of families coping with alcohol and drug problems in South West England and Mexico City. Addiction, 93(12), 1799–1813. doi:10.1046/j.1360-0443.1998.931217996.x
- Orford, J., Natera, G., Velleman, R., Copello, A., Bowie, N., Bradbury, C., … Tiburcio, M. (2001). Ways of coping and the health of relatives facing drug and alcohol problems in Mexico and England. Addiction, 96(5), 761–774. doi:10.1046/j.1360-0443.2001.96576111.x
- Orford, J., Padin, M., de, F. R., Canfield, M., Sakiyama, H. M. T., Laranjeira, R., & Mitsuhiro, S. S. (2017). The burden experienced by Brazilian family members affected by their relatives’ alcohol or drug misuse. Drugs: Education, Prevention and Policy, 26(2), 157–165. doi:10.1080/09687637.2017.1393500
- Orford, J., Rigby, K., Miller, T., Tod, A., Bennett, G., & Velleman, R. (1992). Ways of coping with excessive drug use in the family: A provisional typology based on the accounts of 50 close relatives. Journal of Community & Applied Social Psychology, 2(3), 163–183. doi:10.1002/casp.2450020302
- Orford, J., Templeton, L., Patel, A., Copello, A., & Velleman, R. (2007). The 5-Step family intervention in primary care: I. Strengths and limitations according to family members. Drugs: Education, Prevention and Policy, 14(1), 29–47. doi:10.1080/09687630600997451
- Orford, J., Templeton, L., Velleman, R., & Copello, A. (2005). Family members of relatives with alcohol, drug and gambling problems: A set of standardized questionnaires for assessing stress, coping and strain. Addiction, 100(11), 1611–1624. doi:10.1111/j.1360-0443.2005.01178.x
- Orford, J., Templeton, L., Velleman, R., & Copello, A. (2010). Methods of assessment for affected family members. Drugs: Education, Prevention and Policy, 17(sup1), 75–85. doi:10.3109/09687637.2010.514783
- Orford, J., Velleman, R., Copello, A., Templeton, L., & Ibanga, A. (2010). The experiences of affected family members: A summary of two decades of qualitative research. Drugs: Education, Prevention and Policy, 17(sup1), 44–62. doi:10.3109/09687637.2010.514192
- Orford, J., Velleman, R., Natera, G., Templeton, L., & Copello, A. (2013). Addiction in the family is a major but neglected contributor to the global burden of adult ill-health. Social Science & Medicine, 78, 70–77. doi:10.1016/j.socscimed.2012.11.036
- Ouyang, X., Xin, T., & Chen, F. (2016). Construct Validity of the Children’s Coping Strategies Scale (CCSS): A Bifactor Model Approach. Psychological Reports, 118(1), 199–218. doi:10.1177/0033294116628362
- Ramstedt, M., Sundin, E., Moan, I. S., Storvoll, E. E., Lund, I. O., Bloomfield, K., … Tigerstedt, C. (2015). Harm experienced from the heavy drinking of family and friends in the general population: A comparative study of six Northern European countries. Substance Abuse: Research and Treatment, 9(S2), 107–118. doi:10.4137/SART.S23746
- Rane, A., Church, S., Bhatia, U., Orford, J., Velleman, R., & Nadkarni, A. (2017). Psychosocial interventions for addiction-affected families in Low and Middle Income Countries: A systematic review. Addictive Behaviors, 74, 1–8. doi:10.1016/j.addbeh.2017.05.015
- Ray, G. T., Mertens, J. R., & Weisner, C. (2007). The excess medical cost and health problems of family members of persons diagnosed with alcohol or drug problems. Medical Care, 45(2), 116–122. doi:10.1097/01.mlr.0000241109.55054.04
- Reise, S. P., Morizot, J., & Hays, R. D. (2007). The role of the bifactor model in resolving dimensionality issues in health outcomes measures. Quality of Life Research, 16(S1), 19–31. doi:10.1007/s11136-007-9183-7
- Rodriguez, A., Reise, S. P., & Haviland, M. G. (2016). Applying bifactor statistical indices in the evaluation of psychological measures. Journal of Personality Assessment, 98(3), 223–237. doi:10.1080/00223891.2015.1089249
- Rodriguez, A., Reise, S. P., & Haviland, M. G. (2016). Evaluating bifactor models: Calculating and interpreting statistical indices. Psychological Methods, 21(2), 137–150. doi:10.1037/met0000045
- Roesch, S. C., Aldridge, A. A., Stocking, S. N., Villodas, F., Leung, Q., Bartley, C. E., & Black, L. J. (2010). Multilevel factor analysis and structural equation modeling of daily diary coping data: Modeling trait and state variation. Multivariate Behavioral Research, 45(5), 767–789. doi:10.1080/00273171.2010.519276
- Rossow, I., Felix, L., Keating, P., & McCambridge, J. (2016). Parental drinking and adverse outcomes in children: A scoping review of cohort studies: Parental drinking and harms to children. Drug and Alcohol Review, 35(4), 397–405. doi:10.1111/dar.12319
- Skinner, E. A., Edge, K., Altman, J., & Sherwood, H. (2003). Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychological Bulletin, 129(2), 216–269. doi:10.1037/0033-2909.129.2.216
- Sola, V., Sakiyama, H. M. T., Rato Padin, M. D F., Canfield, M., Bortolon, C. B., Laranjeira, R., & Mitsuhiro, S. S. (2018). Measuring stress, coping, strain and hopefulness of Brazilian family members of substance misusers: Factor structure of a set of measures. Journal of Substance Use, 24(2), 130–139. doi:10.1080/14659891.2018.1523963
- Stone, A. A., Schwartz, J. E., Neale, J. M., Shiffman, S., Marco, C. A., Hickcox, M., … Cruise, L. J. (1998). A comparison of coping assessed by ecological momentary assessment and retrospective recall. Journal of Personality and Social Psychology, 74(6), 1670–1680. doi:10.1037/0022-3514.74.6.1670
- Storvoll, E. E., Moan, I. S., & Lund, I. O. (2016). Negative consequences of other people’s drinking: Prevalence, perpetrators and locations: Harm from other people’s drinking. Drug and Alcohol Review, 35(6), 755–762. doi:10.1111/dar.12376
- The UKATT Research Team. (2001). United Kingdom Alcohol Treatment Trial (UKATT): Hypotheses, design and methods. Alcohol and Alcoholism, 36(1), 11–21. 10.1093/alcalc/36.1.11
- Tobin, D. L., Holroyd, K. A., Reynolds, R. V., & Wigal, J. K. (1989). The hierarchical factor structure of the coping strategies inventory. Cognitive Therapy and Research, 13(4), 343–361. doi:10.1007/BF01173478
- Urbán, R., Kun, B., Farkas, J., Paksi, B., Kökönyei, G., Unoka, Z., … Demetrovics, Z. (2014). Bifactor structural model of symptom checklists: SCL-90-R and Brief Symptom Inventory (BSI) in a non-clinical community sample. Psychiatry Research, 216(1), 146–154. doi:10.1016/j.psychres.2014.01.027
- Velleman, R., Orford, J., Templeton, L., Copello, A., Patel, A., Moore, L., … Godfrey, C. (2011). 12-Month follow-up after brief interventions in primary care for family members affected by the substance misuse problem of a close relative. Addiction Research & Theory, 19(4), 362–374. doi:10.3109/16066359.2011.564691
- Velleman, R., Arcidiacono, C., Procentese, F., Copello, A., & Sarnacchiaro, P. (2008). A 5-step intervention to help family members in Italy who live with substance misusers. Journal of Mental Health, 17(6), 643–655. doi:10.1080/09638230701677761
- Velleman, R., & Templeton, L. (2003). Alcohol, drugs and the family: Results from a Long-Running Research Programme within the UK. European Addiction Research, 9(3), 103–112. doi:10.1159/000070978
- Yang, F. M., Tommet, D., & Jones, R. N. (2009). Disparities in self-reported geriatric depressive symptoms due to sociodemographic differences: An extension of the bi-factor item response theory model for use in differential item functioning. Journal of Psychiatric Research, 43(12), 1025–1035. doi:10.1016/j.jpsychires.2008.12.007
- Zhang, J., Cui, M., Wang, W., Lu, H., Wu, Q., Zhu, X., … Xiao, W. (2014). The coexistence of coping resources and specific coping styles in stress: Evidence from full information item bifactor analysis. PLoS ONE, 9(5), e96451. doi:10.1371/journal.pone.0096451